
Continuous local antibiotic perfusion (CLAP) may be a feasible adjunctive treatment for refractory musculoskeletal infections, providing favourable infection control, functional recovery, and patient satisfaction.
Dr. Shingo Kurahashi, Department of Orthopaedic Surgery, Chubu Rosai Hospital, Nagoya, Aichi, 455-8530, Japan. E-mail: shingo.kurahashi@gmail.com
Abstract
Introduction: Continuous local antibiotic perfusion (CLAP), a novel treatment for bone and soft-tissue infections, maintains high local antimicrobial concentrations while minimising systemic toxicity. Despite its effectiveness against biofilm-related infections and ability to preserve implants, the clinical indications, protocols, and patient-reported outcomes remain unclear. This study assessed the clinical outcomes and patient satisfaction following CLAP for musculoskeletal infections of varied aetiologies and anatomical sites.
Materials and Methods: This retrospective series included consecutive patients undergoing CLAP at a single institution between January 2020 and March 2025. Eligible patients had fracture-related infections, osteomyelitis, soft-tissue abscesses, or post-operative wound infections diagnosed according to the 2018 Musculoskeletal Infection Society criteria. CLAP comprised gentamicin (1.2 mg/mL) delivered through infusion combined with negative-pressure wound therapy. Intravenous antibiotics were administered based on culture and sensitivity results. Primary outcomes included additional surgical procedures after CLAP initiation. Secondary outcomes included infection resolution, length of hospital stay, functional recovery, and patient satisfaction, assessed using a structured Likert-scale survey and the net promoter score (NPS). Most patients had undergone prior surgical debridement and systemic antibiotic therapy, and CLAP was introduced as an adjunct or salvage treatment in cases with persistent or difficult-to-control infection. Infection clearance was defined as the absence of clinical signs of infection, wound healing, and no requirement for further surgical intervention. Functional recovery was defined according to ambulation status in lower-extremity cases and ability to perform activities of daily living in upper-extremity cases.
Results: Thirteen patients (median age, 75 years; 76.9% men) were included. Infections comprised fracture-related infection (n=8), osteomyelitis (n=2), and soft-tissue infection (n=3). Median CLAP duration was 21 days, and median hospital stay was 69 days. Infection clearance was achieved in 12 patients (92%) within a median of 37 days. Six patients (46.2%) required implant removal, and the median number of additional procedures was four. Functional recovery was good or partial in nine patients (69.3%). Satisfaction was high: 84.6% indicated that they would undergo the procedure again, and the mean NPS was 8.2, with no detractors. Implant removal was mainly performed because of persistent infection or compromised bone and soft-tissue conditions. In fracture-related infection cases, radiographic bone healing and clinical pain improvement were also observed during follow-up.
Conclusion: CLAP achieved high infection-clearance rates and favourable functional and satisfaction outcomes, supporting its feasibility as an adjunctive option within surgical and systemic antibiotic management for refractory musculoskeletal infections.
Keywords: Continuous local antibiotic perfusion, refractory musculoskeletal infections, fracture-related infection, osteomyelitis
Continuous local antibiotic perfusion (CLAP) is an emerging therapeutic approach for bone and soft-tissue infections designed to eradicate biofilms by maintaining sustained, high local concentrations of antimicrobial agents at the infection site [1]. Unlike systemic antibiotic therapy, CLAP delivers concentrations exceeding the minimum biofilm eradication threshold while minimising systemic exposure and adverse effects such as nephrotoxicity and ototoxicity [2]. Preclinical and early clinical studies have shown that continuous local administration of gentamicin at 1.2 mg/mL achieves levels sufficient to disrupt biofilms in bone and soft-tissue environments [3]. Importantly, CLAP may enable infection control without implant removal, making it a promising option for implant-associated refractory infections [2]. Although treatment outcomes have been investigated, patient satisfaction has not been reported. CLAP therapy has demonstrated efficacy in chronic osteomyelitis and implant-related infections; however, its effectiveness in acute or extensive infections remains uncertain [4]. Clinical indications – such as infection type, anatomical site, and optimal timing – are yet to be clearly defined. Furthermore, treatment variables, including antibiotic selection, concentration, and perfusion protocols, lack standardisation. While favourable results have been described in individual cases, existing evidence is constrained by small cohorts and the absence of prospective or randomised studies. Broader evaluation across diverse clinical presentations is necessary to clarify the therapeutic scope and limitations of CLAP therapy. This study describes the treatment methods and clinical courses of patients who received CLAP therapy for fracture-related and soft-tissue infections. The series encompasses various anatomical sites and infection types – including phalangeal osteomyelitis, femoral osteomyelitis, soft-tissue abscesses, and postoperative wound infections – allowing comparative analysis of CLAP effectiveness across different clinical contexts. Although the sample size is modest, inclusion of more than ten cases permits preliminary statistical evaluation. In addition, three questionnaire items were used to assess patient satisfaction, with responses obtained directly from patients.
Study design:
This retrospective case series was conducted at a single institution. This study was approved by the Clinical Ethics Committee of Chubu Rosai Hospital on October 27, 2025. No approval number was assigned by the committee. All patients provided written informed consent.
Patient selection:
Consecutive patients with bone or soft-tissue infections who underwent CLAP therapy between January 2020 and March 2025 were included. Patients were excluded if the data were incomplete or if the duration of perfusion was <7 days. Most patients had undergone prior surgical debridement and systemic antibiotic therapy. CLAP was introduced as an adjunct or salvage treatment in cases with persistent or difficult-to-control infection.
Diagnosis:
Infections were diagnosed according to the 2018 Musculoskeletal Infection Society criteria, the 2018 definition of periprosthetic hip and knee infection: an evidence-based and validated criteria [5]. Included conditions comprised fracture-related infections (FRIs), osteomyelitis, soft-tissue abscesses, and post-operative wound infections.
CLAP therapy protocol:
CLAP therapy was administered using a double-lumen tube placed at the infection site connected to an external pump delivering continuous antibiotic perfusion. Gentamicin (1.2 mg/mL) was the primary agent in most cases. Negative-pressure wound therapy was combined with CLAP to allow continuous circulation, with exudate and residual antibiotic solution drained and collected. The perfusion period was typically 1–2 weeks. Intravenous antibiotics were co-administered according to bacterial culture and sensitivity results at the physician’s discretion.
Outcome measures:
The primary outcome was the number of additional surgical procedures (e.g., debridement, implant removal, and revision) required following CLAP initiation. Infection clearance was defined as the absence of clinical signs of infection (e.g., no drainage or erythema), wound healing, and no requirement for further surgical intervention for infection control. In fracture-related infection cases, bone healing was assessed using serial plain radiographs and clinical findings, including pain improvement during weight-bearing or activity. Secondary outcomes included hospital stay length, systemic antibiotic duration, post-operative functional status (walking ability for lower-extremity cases and hand function for upper-extremity cases), and patient satisfaction. ‘Functional recovery’ was defined as the following: Lower extremity: Ambulation status compared to pre-injury level and upper extremity: Ability to perform activities of daily living. Patient satisfaction was assessed through a structured telephone survey using Likert scale-based questions (five-point scale: 1 = very dissatisfied to 5 = very satisfied, with higher scores indicating greater satisfaction) and the net promoter score (NPS) (single-item question: 0 = not at all likely to 10 = extremely likely to recommend; scores ≥9 = promoters, 7–8 = passives, and ≤6 = detractors, with higher scores reflecting greater likelihood of recommending the treatment) [6,7,8].
Statistical analysis:
Descriptive statistics were used to summarise patient demographics, treatment characteristics, and outcomes.
Clinical trial number:
Not applicable.
Thirteen consecutive patients were included. Patient demographics and infection characteristics are summarised in Table 1.
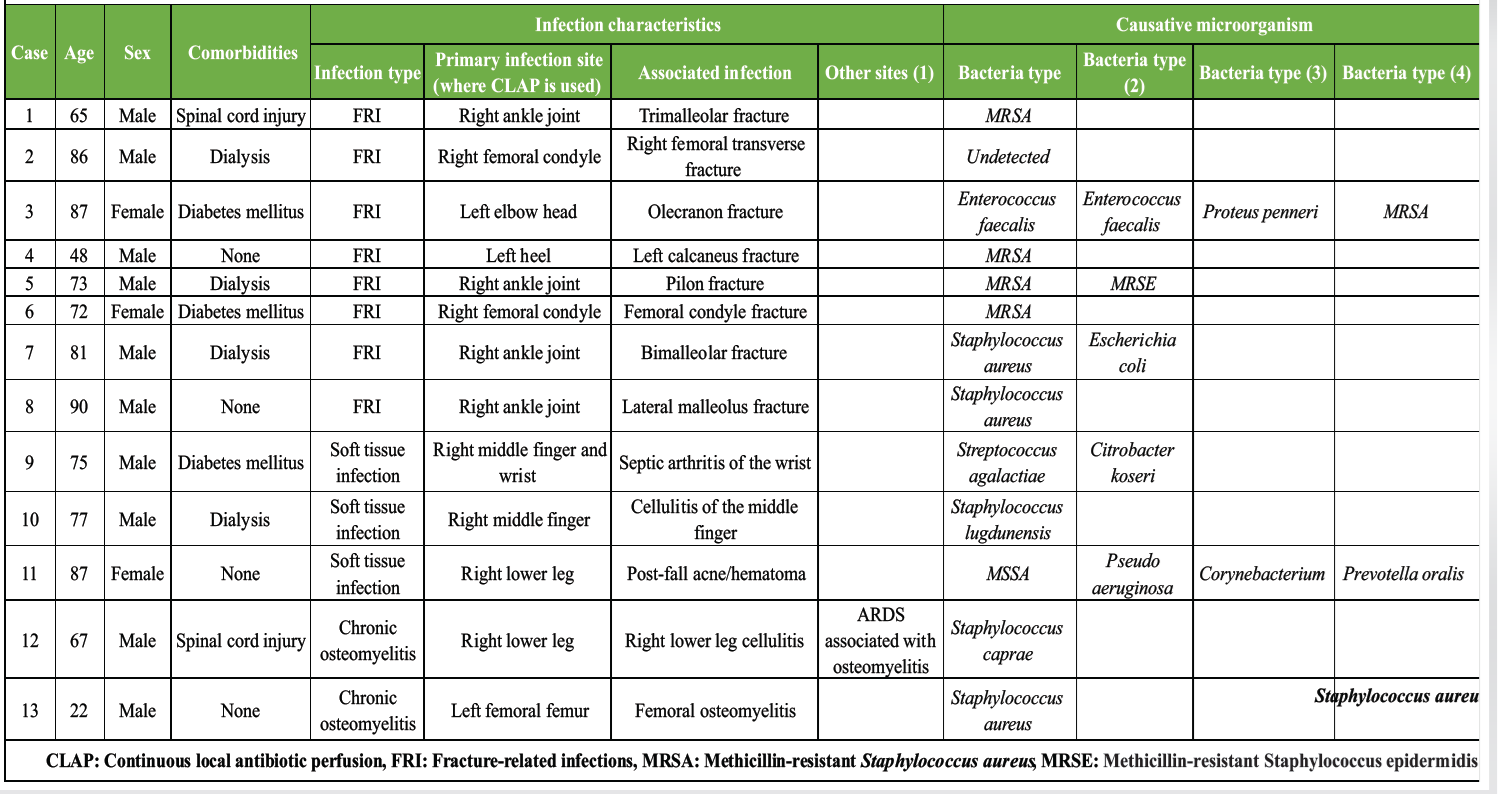
Table 1: Patient characteristics
The median age was 75 years (IQR 67–86, range 22–90), and 10 patients (76.9%) were male. Comorbidities included chronic kidney disease requiring dialysis in four patients (30.8%), diabetes mellitus in three (23.1%), and spinal cord injury in two (15.4%), while four (30.8%) had no significant comorbidities. FRI was the most common condition (eight cases, 61.5%), followed by chronic osteomyelitis (two cases, 15.4%) and soft-tissue infection (three cases, 23.1%). Ten cases (76.9%) were acute, and three (23.1%) were chronic. Causative pathogens included Staphylococcus aureus (MSSA and MRSA), Enterococcus faecalis, and Pseudomonas aeruginosa. Treatment details are shown in Table 2.
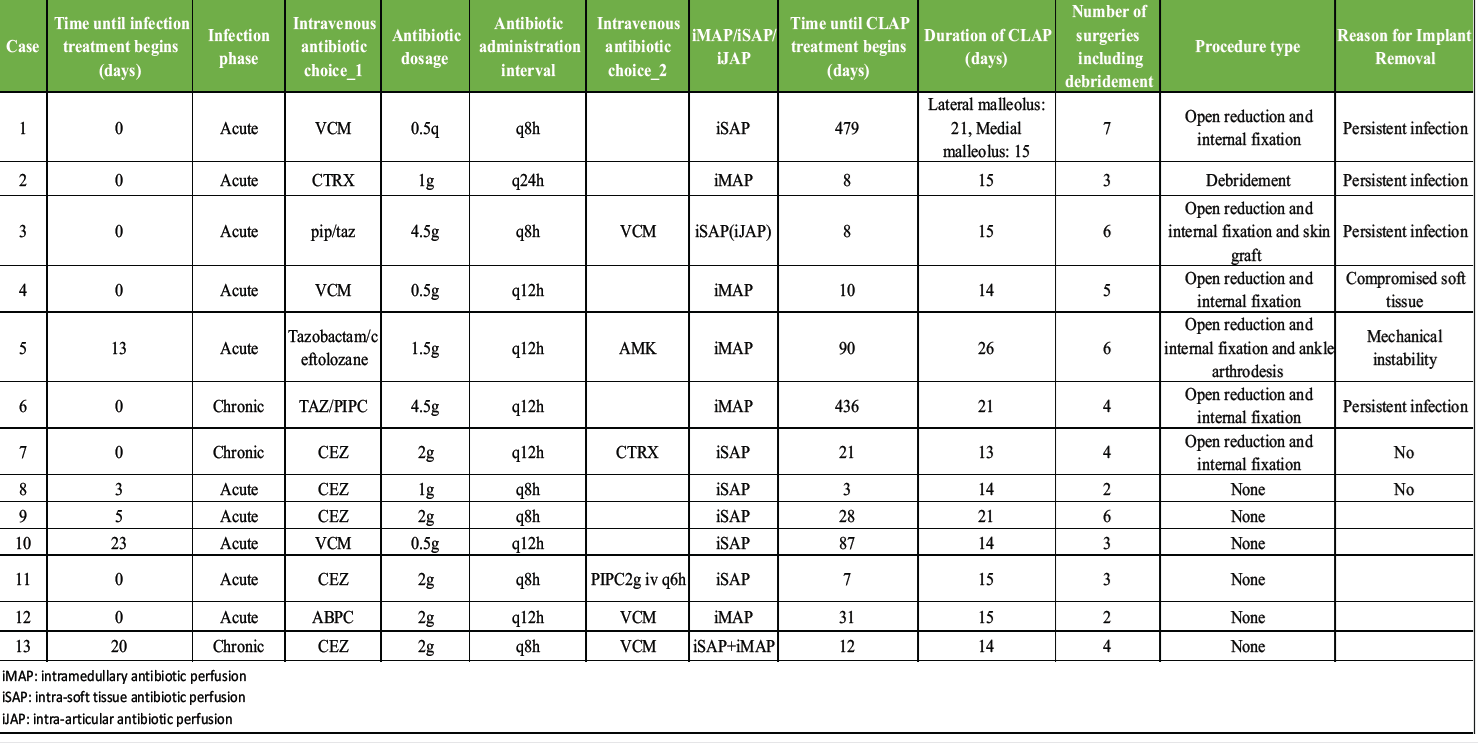
Table 2: Treatment details
The median CLAP duration was 21 days (interquartile range [IQR] 8–31). Patients underwent a median of four additional surgical procedures (IQR 3–6), comprising both major procedures – such as implant removal, open reduction and internal fixation, arthrodesis, and skin grafting – and minor procedures, including repeated debridement, drainage, and wound irrigation. Implant removal was required in six cases (46.2%). Reasons for implant removal included persistent infection, mechanical instability, and compromised bone or soft-tissue conditions. Clinical outcomes are summarised in Table 3.
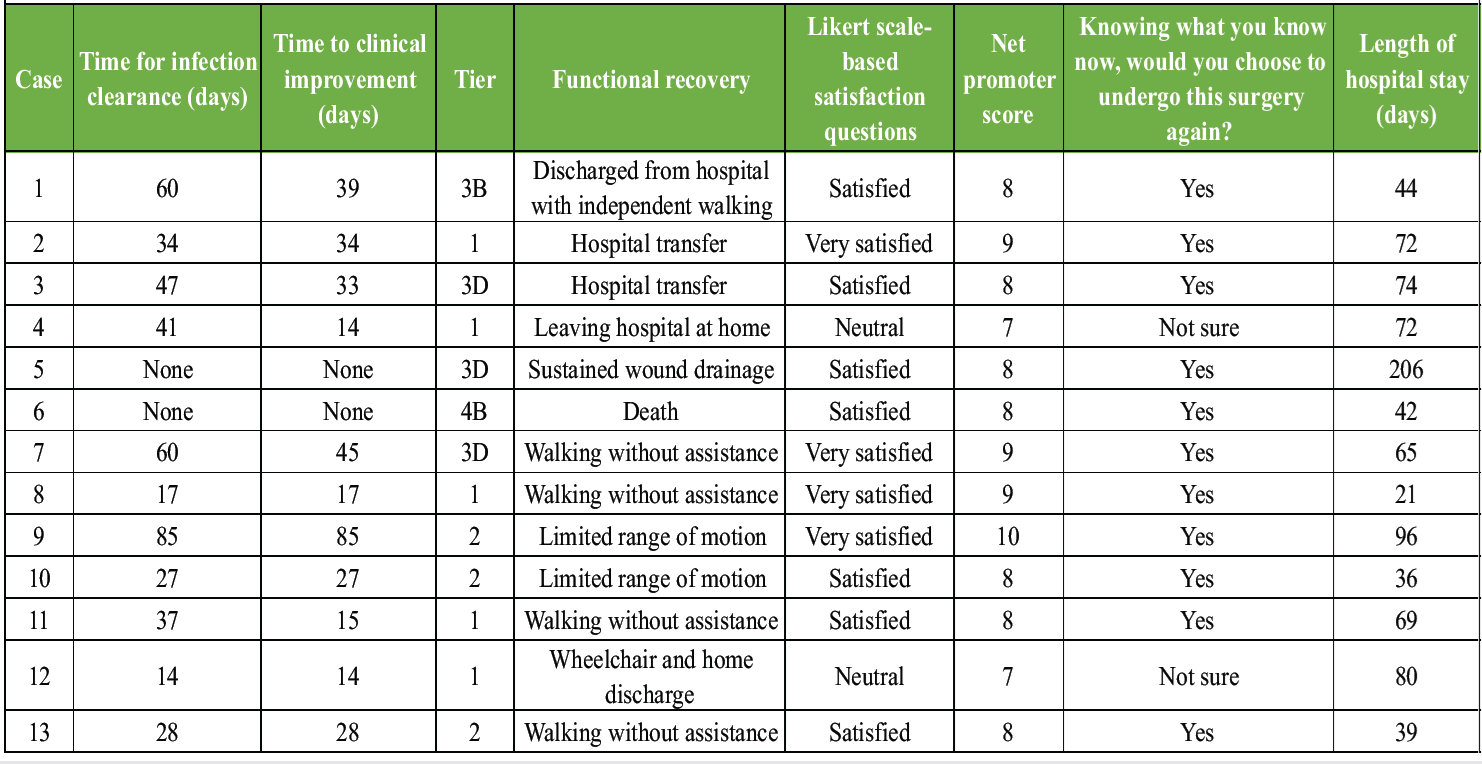
Table 3: Outcomes
The median time to infection clearance was 37 days (IQR 27.5–53.5, range 14–85), and the median hospital stay was 69 days (IQR 42–74, range 21–206). Functional recovery was classified as good in five patients (38.5%), partial in four (30.8%), and poor in four (30.8%). Patient satisfaction was generally high: four patients (30.8%) were very satisfied, seven (53.8%) satisfied, and two (15.4%) neutral. The mean NPS was 8.2, with four patients (30.8%) identified as promoters, nine (69.2%) as passives, and none as detractors. When asked whether they would undergo CLAP therapy again, 11 patients (84.6%) responded “Yes”, and two (15.4%) answered “Not sure”. In fracture-related infection cases, radiographic bone healing and clinical pain improvement were confirmed during follow-up in evaluable patients.
In this retrospective case series, CLAP therapy achieved high infection eradication and favourable functional recovery across musculoskeletal infections. Among 13 patients with acute and chronic infections, including FRI, osteomyelitis, and soft-tissue infection, the median CLAP duration was 21 days, and infection clearance was achieved in most cases within a median of 37 days. Approximately half required implant removal, with a median of four additional surgical procedures. Functional recovery was generally good, and patient satisfaction was high, with most respondents indicating willingness to undergo the therapy again. These findings suggest that CLAP therapy can be an effective and well-accepted option for managing musculoskeletal infections. This study should be interpreted as an exploratory descriptive case series reflecting real-world clinical practice rather than a comparative study establishing definitive treatment indications. CLAP should not be interpreted as a guarantee of implant retention, particularly in severe or complex infections. Infection eradication was achieved in 12 of 13 cases (92%), with a median clearance time of 37 days, indicating that CLAP can provide effective infection control within a relatively short duration. Conventional regimens for osteomyelitis or implant-associated infections typically require parenteral antibiotic courses lasting 4–6 weeks or longer. Compared with systemic therapy, completing infection treatment in a shorter period may reduce complications such as antibiotic resistance and diminished patient ADL. This favourable infection control may be explained by the ability of CLAP to maintain sustained high local antibiotic concentrations that exceed biofilm eradication thresholds while minimising systemic exposure. Our findings align with previous reports on CLAP. A multicentre study on spinal surgical site infections reported an 81% implant retention rate with CLAP therapy, although infection types in that study were more limited [1]. In our cohort, seven FRI cases were included; despite higher case complexity, eradication rates were similarly high, though treatment duration was slightly longer. Infection control was also achieved in osteomyelitis and soft-tissue infections, demonstrating the broader applicability of CLAP beyond implant-related infections. Specifically, three osteomyelitis cases achieved remission, extending the observations of Oe et al. (2021), who reported successful outcomes in chronic osteomyelitis. Likewise, three cases of soft-tissue infections were successfully treated, consistent with the results of Takahashi et al. (2025), who achieved an 81% implant retention rate in spinal surgical site infections. These outcomes suggest that CLAP therapy may be effective across a wide spectrum of musculoskeletal and soft-tissue infections, irrespective of anatomical site or chronicity. These findings suggest that CLAP may have broader applicability as an adjunctive strategy across different musculoskeletal infection settings. The need for implant removal and the number of additional surgical procedures were relatively low compared with conventional management. In prior CLAP case series, implant removal rates have often been reported as negligible. In a previous series of nine FRI cases, all implants were preserved, with infection eradication achieved in all patients [10]. In contrast, 46.2% of our cases required implant removal, reflecting a higher surgical burden due to greater case diversity and severity. In several patients, implant removal was unavoidable because of extensive infection or compromised bone and soft-tissue integrity. Hieda et al. [10] reported a 90.9% implant survival rate in hip periprosthetic joint infection (PJI) treated with debridement, antibiotics, and implant retention (DAIR) plus CLAP, compared with 70% in non-CLAP controls. These comparisons suggest that while CLAP can reduce implant removal relative to standard therapy, outcomes depend on infection complexity and comorbidities. Accordingly, implant preservation should be regarded as a potential advantage in selected cases rather than an expected outcome of CLAP. Functional recovery and patient-reported satisfaction were also favourable. The need for implant removal and the number of additional surgeries were modest compared with traditional approaches. In our series, implant removal was necessary in 46.2% of cases, and the median number of additional procedures was four (IQR 3–6). By contrast, conventional treatment of chronic osteomyelitis or implant-associated infections often requires multiple operations. Jerzy et al. reported an average of 1.5 operations (range 1–5) per patient in non-implant osteomyelitis, while Piuzzi et al. described frequent complications and reoperations during staged revisions for PJI. These comparisons suggest that CLAP may lower surgical burden while maintaining infection control. However, the number of additional procedures should be interpreted primarily as a surrogate of treatment burden rather than as a direct efficacy endpoint. Few previous studies have systematically evaluated patient-reported outcomes after CLAP therapy. Kosugi et al. reported that CLAP enabled infection control without extensive tissue resection in FRI, supporting functional preservation. Similarly, Hieda et al. found that CLAP allowed implant retention and favourable function compared with conventional DAIR alone. Together, these findings suggest that CLAP supports both infection control and functional recovery, although patient-centred outcomes remain underreported. In our study, both the Likert satisfaction score (mean 4.1/5) and the NPS (mean 8.2) reflected strong patient acceptance, with most patients willing to undergo the procedure again. Kosugi et al. suggested that CLAP preserves function by minimising tissue damage, yet patient perspectives were not assessed. Hieda et al. demonstrated favourable function after CLAP in PJIs; however, subjective satisfaction data were lacking. Our findings provide new evidence that CLAP not only achieves infection eradication and functional recovery but is also associated with high patient-reported satisfaction – an aspect seldom addressed previously. Patient-reported outcomes should therefore be interpreted as complementary measures and not as substitutes for objective clinical or functional endpoints. This study has several strengths and novel contributions. First, unlike earlier disease-specific or small-scale reports, this series included a heterogeneous cohort encompassing FRI, osteomyelitis, and soft-tissue infections, many in patients with comorbidities such as dialysis dependence and spinal cord injury. To our knowledge, no prior study has systematically reported such a diverse population with detailed data on pathogens, infection phase (acute vs. chronic), and antibiotic regimens, reflecting the real-world spectrum of refractory musculoskeletal infections. Second, this study uniquely incorporated patient-centred outcomes, including functional recovery, discharge status, and satisfaction assessed by validated tools such as the Likert scale and the NPS. Such outcomes are seldom evaluated in CLAP research but are vital for assessing treatment value. To our knowledge, no prior report has systematically examined patient satisfaction after CLAP therapy. Earlier studies have emphasised infection eradication and implant retention but rarely considered patient experience or perceived benefit. By quantifying satisfaction and willingness to repeat the procedure, our findings provide the first empirical evidence of CLAP acceptability from the patient’s perspective. This approach advances the integration of patient-reported outcomes into musculoskeletal infection research, bridging the gap between clinical success and patient-perceived benefit. Clinically, these results indicate that CLAP therapy is effective for infection eradication and feasible in patients with complex comorbidities and varied infection types. Favourable functional and satisfaction outcomes support its value as an adjunct to surgical and systemic antibiotic management in musculoskeletal infections. In fracture-related infection, bone union remains a critical goal; the radiographic bone healing and pain improvement observed in follow-up support the need to incorporate union-related outcomes in future studies.
This study has several limitations that warrant acknowledgement. First, the number of cases was relatively small. Second, this was a retrospective case series without a control group, preventing direct comparison with patients managed without CLAP therapy. In addition, selection bias is possible, as CLAP was preferentially used in cases where implant retention was considered feasible, whereas patients for whom implant preservation was not possible may have been under-represented. Third, the availability of long-term outcomes was inconsistent. Some patients lacked extended follow-up, hindering full assessment of the durability of infection control and prevention of reinfection after completion of CLAP therapy. Fourth, the single-centre setting in Japan may limit generalisability as the patient population, comorbidity patterns, causative organisms, and healthcare resources may differ from those in other regions. Additional limitations include cohort heterogeneity, lack of a standardised CLAP protocol, absence of validated functional outcome scores, limited formal safety evaluation regarding systemic gentamicin exposure, and incomplete long-term assessment of recurrence and bone union.
CLAP therapy achieved infection clearance in most musculoskeletal infections, including fracture-related infections, osteomyelitis, and soft-tissue infections. Although additional surgical procedures and implant removal were often required, functional recovery and patient satisfaction were generally favourable. These findings suggest that CLAP is a feasible adjunctive option for managing complex musculoskeletal infections. Further studies are needed to establish standardised indications and treatment protocols.
Continuous local antibiotic perfusion (CLAP) may be a useful adjunctive treatment for refractory musculoskeletal infections, achieving favourable infection control while preserving function and supporting patient satisfaction.
References
- 1. Kosugi K, Zenke Y, Sato N, Hamada D, Ando K, Okada Y, et al. Potential of continuous local antibiotic perfusion therapy for fracture-related infections. Infect Dis Ther 2022;11:1741-55. [Google Scholar] [PubMed]
- 2. Iwamoto K, Yamamoto N, Saiga K, Maruo A, Noda T, Kawasaki K, et al. Prosthetic joint infection after total talar replacement: An implant-retained case treated with combined continuous local antibiotic perfusion (CLAP). J Orthop Sci 2024;29:349-53. [Google Scholar] [PubMed]
- 3. Takahara S, Maruo A, Takayama H, Harada T. Continuous local antibiotics perfusion therapy for acute deep infections after open fractures. Case Rep Orthop 2022;2022:2563939. [Google Scholar] [PubMed]
- 4. Maruo A, Oda T, Mineo R, Miya H, Muratsu H, Fukui T, et al. Continuous local antibiotic perfusion: A treatment strategy that allows implant retention in fracture-related infections. J Orthop Surg (Hong Kong) 2022;30:10225536221111902. [Google Scholar] [PubMed]
- 5. Parvizi J, Tan TL, Goswami K, Higuera C, Della Valle C, Chen AF, et al. The 2018 definition of periprosthetic hip and knee infection: An evidence-based and validated criteria. J Arthroplasty 2018;33:1309-14.e2. [Google Scholar] [PubMed]
- 6. Zammit M, Siau R, Williams C, Hussein A. Patient satisfaction from ENT telephone consultations during the coronavirus disease 2019 pandemic. J Laryngol Otol 2020;134:917-924. [Google Scholar] [PubMed]
- 7. Allen AZ, Zhu D, Shin C, Glassman DT, Abraham N, Watts KL. Patient satisfaction with telephone versus video-televisits: A cross-sectional survey of an urban, multiethnic population. Urology 2021;156:110-6. [Google Scholar] [PubMed]
- 8. Krol MW, De Boer D, Delnoij DM, Rademakers JJ. The net promoter score-an asset to patient experience surveys? Health Expect 2015;18:3099-109. [Google Scholar] [PubMed]
- 9. Besal R, Adamič P, Beović B, Papst L. Systemic antimicrobial treatment of chronic osteomyelitis in adults: A narrative review. Antibiotics (Basel) 2023;12:944. [Google Scholar] [PubMed]
- 10. Hieda Y, Choe H, Maruo A, Abe K, Shimoda M, Ike H, et al. Clinical outcomes of continuous local antibiotic perfusion in combination with debridement antibiotics and implant retention for periprosthetic hip joint infection. Sci Rep 2025;15:26017. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Management of Chronic Osteomyelitis Bone Defect Titanium Cage Combined with the Masquelet Technique: A Case Report
July 1, 2026 Management of Chronic Osteomyelitis Bone Defect Titanium Cage Combined with the Masquelet Technique: A Case Report June 1, 2026 Ceftazidime-Avibactam/Aztreonam Combination for the Treatment of Carbapenem-resistant Klebsiella pneumoniae-induced Osteomyelitis: A Case Series with Review of Literature
June 1, 2026 Ceftazidime-Avibactam/Aztreonam Combination for the Treatment of Carbapenem-resistant Klebsiella pneumoniae-induced Osteomyelitis: A Case Series with Review of Literature May 1, 2026 Tibial Osteomyelitis due to Burkholderia pseudomallei in a Non-diabetic Patient: A Case Report
May 1, 2026 Tibial Osteomyelitis due to Burkholderia pseudomallei in a Non-diabetic Patient: A Case Report April 1, 2026 A Rare Case of Chronic Pan-Diaphyseal Osteomyelitis of the Fibula in a Child Treated by Near Total Fibulectomy: A Case Report
April 1, 2026 A Rare Case of Chronic Pan-Diaphyseal Osteomyelitis of the Fibula in a Child Treated by Near Total Fibulectomy: A Case Report