
Fixed flexion deformities in osteoarthritic knees can be effectively corrected during total knee arthroplasty using a graded release protocol, resulting in durable deformity correction and high patient satisfaction.
Dr Shravani Jagadabi, Department of Orthopaedics, Nizams Institute of Medical Sciences, Punjagutta, Hyderabad, Telangana, India. E-mail: jagadabishravani@gmail.com
Abstract
Introduction: Fixed flexion deformity (FFD) in advanced knee osteoarthritis (OA) presents a significant intraoperative challenge during total knee arthroplasty (TKA), primarily due to soft-tissue contractures and bony deformities that impede optimal alignment and functional recovery. This study aims to evaluate the effectiveness of intraoperative correction of FFD and to assess short-term functional outcomes following TKA.
Materials and Methods: In this prospective observational study, 55 knees (mean age 57.28 ± 9.35 years) with Grade 4 OA and FFD underwent TKA between March 2022 and March 2024. Correction was achieved using graded posterior soft-tissue releases and distal femoral resections. Functional outcomes were assessed at 6 months using the Knee Society Score (KSS) and the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC).
Results: The mean pre-operative FFD of 23.04° was significantly corrected intraoperatively. At 6 months, the mean KSS improved from 51.29 to 81.93, whereas the WOMAC decreased from 80.93 to 20.1 (P < 0.001). Full knee extension was achieved in all cases, with excellent/good outcomes in 89.08% of patients. No significant differences were observed between primary and secondary OA groups.
Conclusion: Systematic intraoperative correction of FFD using algorithm-based soft-tissue release and distal femoral resection during TKA gave reliable deformity correction, excellent functional recovery, and high patient satisfaction in this study. However, longer-term studies with larger sample sizes are needed to confirm the durability of these outcomes.
Keywords: Total knee arthroplasty, fixed flexion deformity, posterior soft-tissue release, distal femoral resection, osteoarthritis, functional outcomes, Western Ontario and McMaster Universities Osteoarthritis Index score, Knee Society score.
Osteoarthritis (OA) is a chronic degenerative disease that affects synovial joints. It is characterised by gradual softening and fibrillation of articular cartilage, along with marginal osteophyte growth and changes in the subchondral bone [1,2]. Fixed flexion deformities (FFD) are common in osteoarthritic knees. FFD results from chronic knee flexion, leading to tightening of the posterior capsule, shortening of ligaments and muscles, and bone changes at the posterior tibial plateau and femoral condyles [3,4]. These deformities disrupt knee movement and increase stress on the knee compartments [5,6,7]. Problems with full knee extension can cause quadriceps contractures, increase energy expenditure while walking, reduce speed, and lead to abnormal gait patterns [6]. Incomplete correction of FFD during total knee arthroplasty (TKA) leads to worse outcomes, making full correction during surgery critical [7]. TKA is considered the gold standard treatment for advanced knee OA refractory to conservative therapies [2]. Present-day TKA prostheses, encompassing cruciate-retaining and posterior-stabilised configurations, have substantially enhanced post-operative functional recovery [8]. Range of motion is a critical determinant of TKA success. Standard TKA aims to restore post-operative range of motion from 0° to 120°, although 0° to 95° frequently suffices for proper function [5]. The presence of residual fixed flexion deformity (FFD) is a hurdle in achieving these kinematic targets, necessitating tailored surgical modifications. Surgical management of FFD mandates specialised techniques, which include adequate bone resection, ligamentous releases, posterior osteophyte excision, and posterior capsular lengthening to optimise ligament balancing and restore the joint line [8,9,10,11]. This prospective study aims to analyse the degree of FFD preoperatively, intraoperatively, and postoperatively and the systematic surgical approach to treat FFD in osteoarthritic knees using TKA, i.e., soft-tissue contracture release, bone resections, and functional outcome evaluation using KSS and WOMAC scoring systems.
This prospective observational study was conducted at the Department of Orthopaedics, Nizams Institute of Medical Sciences (NIMS), Hyderabad, India – a tertiary care academic medical centre – following approval by the NIMS Institutional Ethics Committee (EC/NIMS/3083/2022, held on October 29, 2022, approved on February 03, 2023). Between March 2022 and March 2024, 55 knees (28 males, 27 females; including five bilateral cases) with Grade 4 OA (Kellgren–Lawrence scale) and FFD exceeding 10° underwent TKA (Table 1).
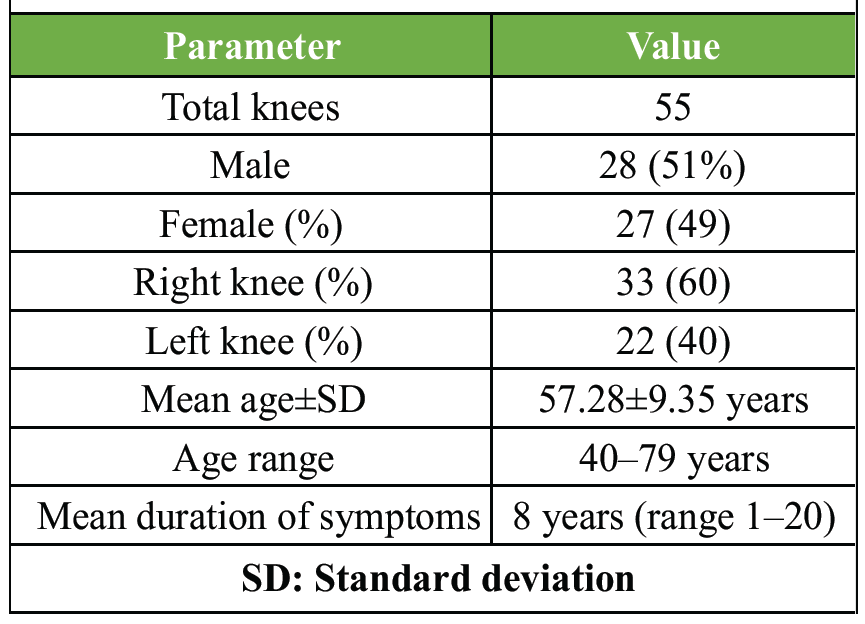
Table 1: Patient demographics
Method of assessment:
Pre-operative planning included a comprehensive clinical and radiographic evaluation of FFD. The degree of FFD was quantified using an image-based measurement system (Fig. 1), along with assessment of coronal plane deformity.

Figure 1: Pre-operative clinical image of both knees showing fixed flexion deformity.
Standard weight-bearing anteroposterior and lateral radiographs were obtained and graded according to the Kellgren–Lawrence classification. Baseline functional status was evaluated using the Knee Society Score (KSS) and the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC). Informed consent was obtained from all patients before surgery.
Surgical details:
All procedures were performed with the patient in the supine position under tourniquet control, with intravenous cefuroxime–sulbactam administered 30 min before incision. A posterior-stabilised TKA system was used in all patients (Fig. 2).
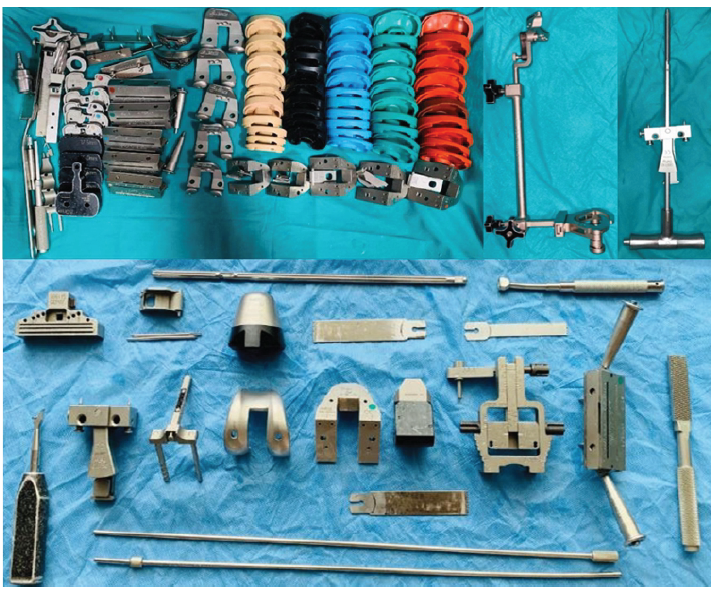
Figure 2: Posterior-stabilized instrument system from Depuy Inc. with standard cutting blocks and tibial and femoral alignment jigs.
A standard medial parapatellar approach was employed. Surgical correction followed a stepwise algorithm tailored to the degree of deformity, with emphasis on balanced flexion–extension gaps. Tibial resection of 8 mm was performed first from the least affected plateau, perpendicular to the mechanical axis, using an extramedullary guide, while avoiding excessive posterior slope. In cases with restricted flexion, a greater tibial resection was done. Systematic removal of anterior and posterior osteophytes from the distal femur, proximal tibia, and patella was undertaken to relieve mechanical blocks to extension. Distal femoral resection was performed using an intramedullary guide with 5°–7° valgus alignment to restore the joint line, and femoral rotation was set at 3° external rotation based on the posterior condylar axis and Whiteside’s line. Posterior osteophyte excision and posterior capsular release from the femoral attachment using a mop (to prevent neurovascular injury) and a curved osteotome were performed to improve extension. If residual flexion deformity persisted after soft-tissue balancing and standard bone cuts, an additional distal femoral resection of approximately 2 mm was undertaken to balance the extension and flexion gaps. Trial reduction was performed after confirming stability and patellar tracking. Thorough irrigation with pulse lavage was performed. Definitive cementation and implantation were then completed, and the wound was closed in layers over a negative suction drain (Fig. 3).
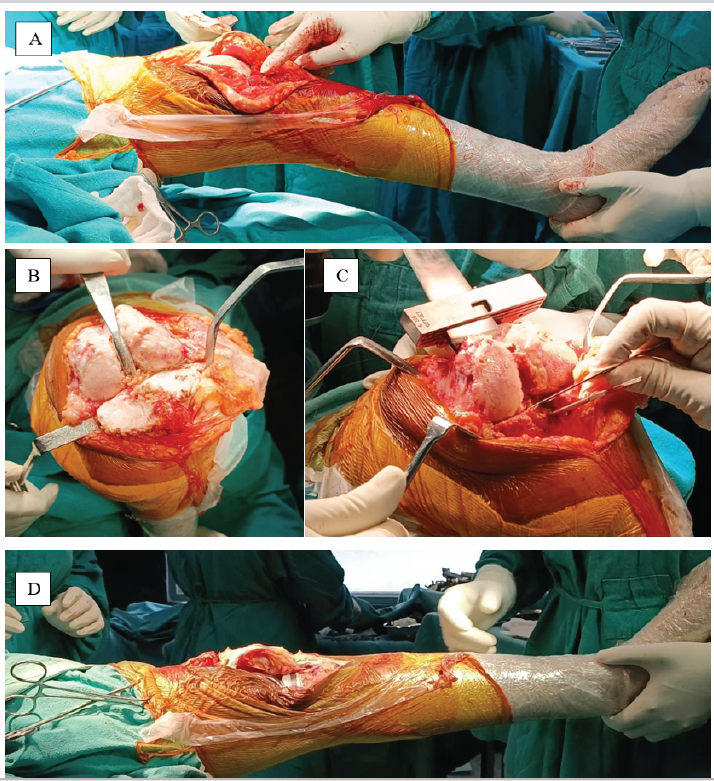
Figure 3: (A) Intraoperative arthrotomy and removal of patellofemoral osteophytes, (B) subluxation of tibia for tibial cut, (C) distal femur cut, (D) intraoperative image after correction of flexion deformity.
The stepwise algorithm depicting the graded, stepwise correction of FFD based on severity is shown in Fig. 4. Post-operative evaluation included day-2 radiographs, serial goniometric clinical assessments, imaging, and functional scoring using the KSS/WOMAC at follow-up intervals (10 days, 3 months, and 6 months).
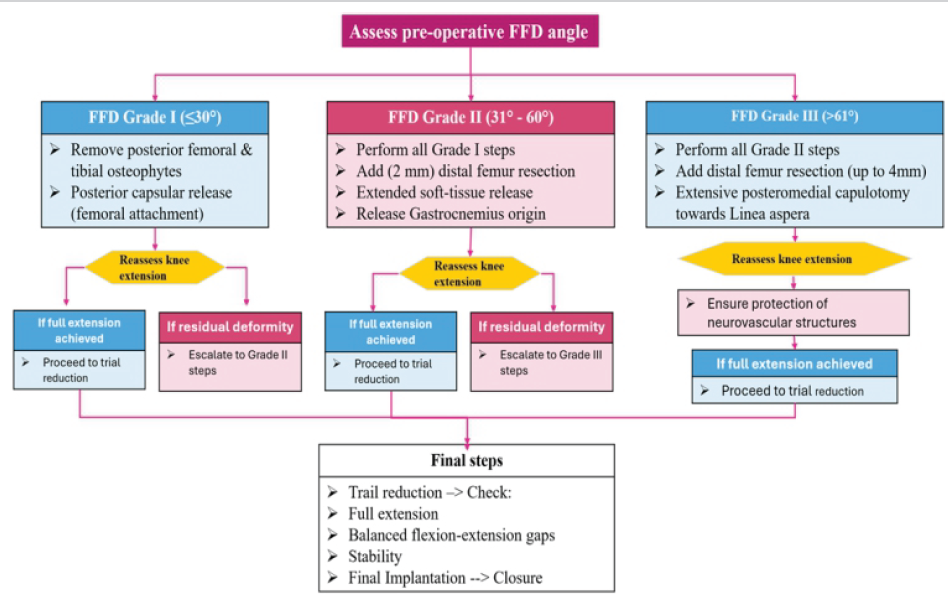
Figure 4: Algorithm depicting the graded, stepwise correction of fixed flexion deformity based on severity.
Rehabilitation protocol: Stepwise approach:
Pre-operative physiotherapy included patient counselling, targeted strengthening of the quadriceps, hamstrings, hip abductors, and hip flexors, skin traction to relax the posterior capsule, flexibility exercises, and gait and balance training. Post-operative rehabilitation was structured into three phases. Phase I (Days 1–10) focused on pain and oedema control using cryotherapy and limb elevation, with early mobilisation through ankle-toe movements, static quadriceps and hamstring exercises, gluteal isometrics, pelvic bridging, assisted and active range of motion exercises, short arc quadriceps, passive knee extension stretching, patellar mobilisation, and initiation of partial weight-bearing ambulation with walker support. Phase II (weeks 2–6) emphasised improving the range of motion, strength, and stability through quadriceps sets, heel slides, long-arc quadriceps, straight-leg raises, hamstring curls, knee extension exercises, stretching, independent ambulation, and balance training. Phase III (>6 weeks) aimed at achieving knee flexion ≥115°, enhancing muscular strength and endurance, improving eccentric and concentric control, and facilitating return to functional and daily activities.
Statistical analysis:
Descriptive statistics (mean, median, mode, standard deviation, and range) were computed for all variables. Analysis of variance was used to evaluate the associations between age and functional outcomes, whereas paired t-tests were used to compare pre-operative and post-operative metrics. Statistical significance was set at P < 0.05.
The study included 55 knees from 28 males and 27 females, with a mean age of 57.28 years, comprising primary OA in 43 knees (78.18%) and secondary arthritis (rheumatoid) in 12 knees (21.82%). FFD distribution is shown in Table 2; 37 cases had associated varus deformity, 4 had valgus, and others had no deformity.
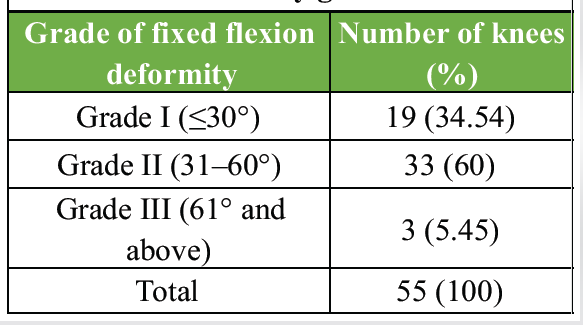
Table 2: Distribution of fixed flexion deformity grades
The mean pre-operative FFD was 23.04° (standard deviation ± 10.5°; range 5–70°), with 3 cases having Grade 3 deformity that is more than 60° (65° in two patients and 70° in the other). Mean bone resections were 9 mm ± 1.2 mm (femoral) and 8 mm ± 0.9 mm (tibial), with a posterior slope of 3°. Complete intraoperative FFD correction could be achieved in most cases, with full extension maintained at 6 months in 54 knees (98.2%); one knee had a 2° lag without functional issues. Post-operative KSS were excellent in 21 knees (38.18%), good in 28 (50.90%), fair in 4 (7.2%), and poor in 2 (3.63%), yielding 89.08% good/excellent results and a mean KSS improvement of 30.64 points (51.29–81.93). WOMAC scores improved by 60.83 points (80.93–20.10) across pain, stiffness, and function domains as shown in Table 3. No significant age/gender or primary/secondary arthritis differences. Patient satisfaction levels were very high in 71%, satisfied in 24.5%, and moderate in 4.5%, driven primarily by pain relief and mobility.
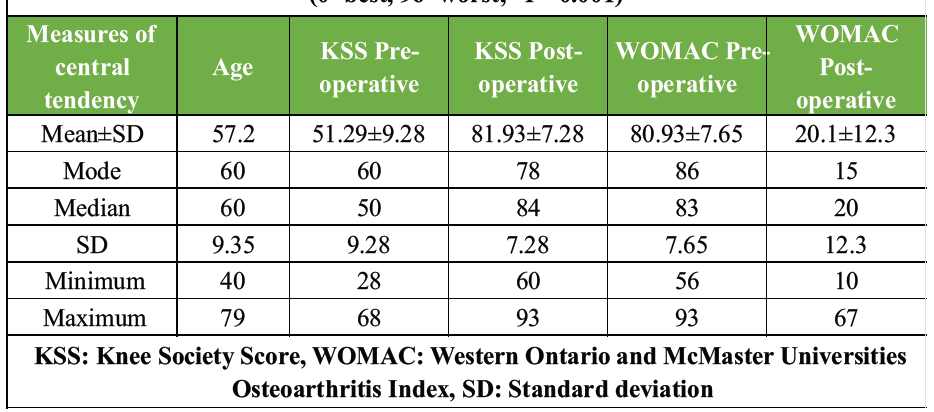
Table 3: Patient outcomes based on KSS score (*P<0.001), WOMAC score outcomes (0=best, 96=worst; *P<0.001)
This prospective study demonstrates a stepwise approach to correcting FFD during TKA. The high rate of complete correction and maintenance of extension at 6 months aligns with previously published studies emphasising the importance of systematic soft-tissue balancing and deformity correction [6,7]. Previous literature suggests that residual flexion contracture >15° at 3 months postoperatively may persist long-term, underscoring the need for adequate intraoperative correction [4]. Our findings are consistent with studies reporting that patients with corrected FFD achieve comparable outcomes to those without pre-operative deformities [6]. The observed improvement in KSS and WOMAC scores in this study is comparable to or exceeds outcomes reported in existing literature, where functional gains are closely associated with restoration of full extension and balanced flexion-extension gaps [6,7]. Post-operative range of motion in our cohort, although slightly below the ideal range, was functionally adequate and consistent with previous studies comparing prosthesis designs and kinematic outcomes [5,14]. No significant differences were observed between the primary OA and rheumatoid arthritis groups, consistent with prior studies demonstrating that posterior-stabilised implants provide reliable outcomes in inflammatory arthritis when combined with appropriate soft-tissue balancing [13]. The surgical approach in this study focused on a stepwise, graded correction of deformity. Distal femoral resection was a key component in managing flexion contracture, with careful additional resection improving knee extension while preserving joint stability [12] and restoring the joint line [10]. Sequential removal of posterior osteophytes, followed by posterior capsular release, was performed to achieve a balanced extension gap [9]. Gap-balancing techniques were used to maintain appropriate ligament tension and alignment, thereby supporting favourable postoperative outcomes [11]. The use of posterior-stabilised implants further contributed to deformity correction by enhancing stability through the cam–post mechanism and promoting femoral rollback during knee flexion [14,16], which has been widely supported in the literature. Unlike previous studies, such as the Ranawat Award study by Franklin et al., which evaluated the influence of patient-related factors, including quadriceps strength and metabolic status, on post-operative outcomes, our study did not include these variables in the analysis [15]. The findings in this study support a comprehensive, protocol-driven approach that integrates surgical technique and rehabilitation to achieve consistent results across patient subgroups.
Limitations:
- Small sample size,
- Absence of a control group, and
- Inadequate analysis of pre-operative comorbidities, such as metabolic and nutritional factors, may confound outcomes.
- Larger prospective comparative studies are needed to validate these findings.
This study demonstrates the use of a standardized intraoperative algorithm for managing FFD in osteoarthritic knees. This is effective in achieving near-complete deformity correction. Improvements in KSS and WOMAC scores suggest that this method improves post-operative function and patient satisfaction in the early follow-up period. However, longer-term studies with larger sample sizes are needed to confirm the durability of these outcomes.
Meticulous, algorithm-based correction of fixed flexion deformity during total knee arthroplasty enables complete extension and significantly improves functional outcomes.
References
- 1. Felson DT. Osteoarthritis as a disease of mechanics. Osteoarthritis Cartilage. 2013 Jan;21(1):10-5. doi: 10.1016/j.joca.2012.09.012. Epub 2012 Oct 4. PMID: 23041436; PMCID: PMC3538894. [Google Scholar] [PubMed] [CrossRef]
- 2. Sharma L. Osteoarthritis of the Knee. N Engl J Med. 2021 Jan 7;384(1):51-59. doi: 10.1056/NEJMcp1903768. PMID: 33406330. [Google Scholar] [PubMed] [CrossRef]
- 3. Bellemans J, Robijns F, Duerinckx J, Banks S, Vandenneucker H. The influence of tibial slope on maximal flexion after total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2005 Apr;13(3):193-6. doi: 10.1007/s00167-004-0557-x. Epub 2004 Oct 26. PMID: 15824934. [Google Scholar] [PubMed] [CrossRef]
- 4. Mitsuyasu H, Matsuda S, Miura H, Okazaki K, Fukagawa S, Iwamoto Y. Flexion contracture persists if the contracture is more than 15° at 3 months after total knee arthroplasty. J Arthroplasty. 2011 Jun;26(4):639-43. doi: 10.1016/j.arth.2010.04.023. Epub 2010 Jun 11. PMID: 20541887. [Google Scholar] [PubMed] [CrossRef]
- 5. Kim YH, Choi Y, Kwon OR, Kim JS. Functional outcome and range of motion of high-flexion posterior cruciate-retaining and high-flexion posterior cruciate-substituting total knee prostheses. A prospective, randomized study. J Bone Joint Surg Am. 2009 Apr;91(4):753-60. doi: 10.2106/JBJS.H.00805. PMID: 19339558. [Google Scholar] [PubMed] [CrossRef]
- 6. Cheng K, Ridley D, Bird J, McLeod G. Patients with fixed flexion deformity after total knee arthroplasty do just as well as those without: ten-year prospective data. Int Orthop. 2010 Jun;34(5):663-7. doi: 10.1007/s00264-009-0801-6. Epub 2009 May 14. PMID: 19437018; PMCID: PMC2903176. [Google Scholar] [PubMed] [CrossRef]
- 7. Ritter MA, Lutgring JD, Davis KE, Berend ME, Pierson JL, Meneghini RM. The role of flexion contracture on outcomes in primary total knee arthroplasty. J Arthroplasty. 2007 Dec;22(8):1092-6. doi: 10.1016/j.arth.2006.11.009. PMID: 18078875. [Google Scholar] [PubMed] [CrossRef]
- 8. Meloni MC, Hoedemaeker RW, Violante B, Mazzola C. Soft tissue balancing in total knee arthroplasty. Joints. 2014 May 8;2(1):37-40. PMID: 25606540; PMCID: PMC4295665. [Google Scholar] [PubMed]
- 9. Baldini A, Scuderi GR, Aglietti P, Chalnick D, Insall JN. Flexion-extension gap changes during total knee arthroplasty: effect of posterior cruciate ligament and posterior osteophytes removal. J Knee Surg. 2004 Apr;17(2):69-72. doi: 10.1055/s-0030-1248201. PMID: 15124658. [Google Scholar] [PubMed] [CrossRef]
- 10. Bellemans J. Restoring the joint line in revision TKA: does it matter? Knee. 2004 Feb;11(1):3-5. doi: 10.1016/S0968-0160(03)00099-1. PMID: 14967319. [Google Scholar] [PubMed] [CrossRef]
- 11. Daines BK, Dennis DA. Gap balancing vs. measured resection technique in total knee arthroplasty. Clin Orthop Surg. 2014 Mar;6(1):1-8. doi: 10.4055/cios.2014.6.1.1. Epub 2014 Feb 14. PMID: 24605183; PMCID: PMC3942594. [Google Scholar] [PubMed] [CrossRef]
- 12. Liu DW, Reidy JF, Beller EM. The Effect of Distal Femoral Resection on Fixed Flexion Deformity in Total Knee Arthroplasty. J Arthroplasty. 2016 Jan;31(1):98-102. doi: 10.1016/j.arth.2015.07.033. Epub 2015 Jul 22. PMID: 26321077. [Google Scholar] [PubMed] [CrossRef]
- 13. Tang WM, Chiu KY, Ng TP, Yau WP. Posterior cruciate ligament-substituting total knee arthroplasty in young rheumatoid patients with advanced knee involvement. J Arthroplasty. 2004 Jan;19(1):49-55. doi: 10.1016/j.arth.2003.08.009. PMID: 14716651. [Google Scholar] [PubMed] [CrossRef]
- 14. Miner AL, Lingard EA, Wright EA, Sledge CB, Katz JN; Kinemax Outcomes Group. Knee range of motion after total knee arthroplasty: how important is this as an outcome measure? J Arthroplasty. 2003 Apr;18(3):286-94. doi: 10.1054/arth.2003.50046. PMID: 12728419. [Google Scholar] [PubMed] [CrossRef]
- 15. Franklin PD, Li W, Ayers DC. The Chitranjan Ranawat Award: Functional outcome after total knee replacement varies with patient attributes. Clin Orthop Relat Res. 2008;466:2597-604. [Google Scholar] [PubMed]
- 16. Insall JN, Lachiewicz PF, Burstein AH. The posterior stabilized condylar prosthesis: a modification of the total condylar design. Two to four-year clinical experience. J Bone Joint Surg Am. 1982 Dec;64(9):1317-23. PMID: 7142239. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Comparative Analysis of Functional Outcomes in Robotic-assisted versus Conventional Total Knee Arthroplasty
June 1, 2026 Comparative Analysis of Functional Outcomes in Robotic-assisted versus Conventional Total Knee Arthroplasty June 1, 2026 The Prevalence of Complex Regional Pain Syndrome after Primary Total Knee Arthroplasty – A Longitudinal Study
June 1, 2026 The Prevalence of Complex Regional Pain Syndrome after Primary Total Knee Arthroplasty – A Longitudinal Study May 1, 2026 Coronal Plane Alignment of the Knee Classification and Its Correlation with Post-operative Functional Outcomes in Total Knee Arthroplasty: A Prospective Cohort Study
May 1, 2026 Coronal Plane Alignment of the Knee Classification and Its Correlation with Post-operative Functional Outcomes in Total Knee Arthroplasty: A Prospective Cohort Study February 1, 2026 Conventional Total Knee Arthroplasty in Severe Anterolateral Femoral Bowing: Lateralized Femoral Entry Point to Approach Navigation Level Alignment – A Case Report
February 1, 2026 Conventional Total Knee Arthroplasty in Severe Anterolateral Femoral Bowing: Lateralized Femoral Entry Point to Approach Navigation Level Alignment – A Case Report