
Graded vitamin D deficiency significantly influences hip fracture patterns, with moderate deficiency linked to intertrochanteric fractures and severe deficiency to femoral neck fractures.
Dr Madhan Jeyaraman, Department of Orthopaedics, ACS Medical College and Hospital, Dr MGR Educational and Research Institute, Chennai, Tamil Nadu, India. E-mail: madhanjeyaraman@gmail.com
Abstract
Introduction: Hip fractures represent a major public health problem in India, associated with significant morbidity, mortality, and socioeconomic burden. Vitamin D deficiency, highly prevalent in the Indian population, is a modifiable risk factor for osteoporosis, muscle weakness, falls, and fragility fractures. While the association between hypovitaminosis D and hip fractures is well established, limited Indian data exist examining fracture patterns across different severities of vitamin D deficiency. The study is to evaluate the association between varying levels of serum vitamin D deficiency and types of hip fractures in the Indian population.
Materials and Methods: This hospital-based cross-sectional observational study was conducted in the Department of Orthopaedics, School of Medical Sciences and Research, Sharda University, Greater Noida, from April 2024 to November 2025. Fifty patients aged >50 years (females) and >60 years (males) presenting with low-energy hip fractures were included. Serum 25-hydroxyvitamin D levels were measured using a VITROS 5600 dry chemistry autoanalyser. Vitamin D status was categorised as severe deficiency (<10 ng/mL), moderate deficiency (10–20 ng/mL), insufficiency (20–30 ng/mL), and sufficiency (>30 ng/mL). Statistical analysis was performed using the Statistical Package for the Social Sciences v22 with the chi-square test and analysis of variance.
Results: The majority of patients were aged 70–79 years (52%). Intertrochanteric fractures were the most common fracture type (60%), followed by neck of femur fractures (34%). Vitamin D deficiency (severe + moderate) was present in 72% of patients. Moderate deficiency (10–20 ng/mL) was the predominant category (60%). Intertrochanteric fractures were most frequently associated with moderate deficiency, whereas severe deficiency was more common among neck-of-femur fractures. The association between vitamin D status and fracture type was statistically significant (P < 0.05).
Conclusion: Vitamin D deficiency is highly prevalent among Indian patients with hip fractures and shows a significant association with fracture subtype. Graded vitamin D deficiency appears to influence both fracture occurrence and anatomical pattern. Routine screening and early correction of vitamin D deficiency may play a critical role in hip fracture prevention in the elderly Indian population.
Keywords: Vitamin D deficiency, hip fracture, intertrochanteric fracture, neck of femur fracture, osteoporosis
Hip fractures constitute a growing global public health concern, particularly among the elderly, due to their association with increased morbidity, mortality, prolonged hospitalization, and long-term functional dependence [1,2,3]. These fractures significantly impair quality of life and frequently result in permanent loss of independence. Projections suggest that by 2050, the annual global incidence of hip fractures may exceed 6 million, with a substantial proportion arising from Asia, including India [4,5]. In India, the incidence of hip fractures is increasing in parallel with demographic aging, urbanization, and lifestyle changes [6,7,8]. Notably, Indian patients tend to sustain hip fractures nearly a decade earlier than Western populations, suggesting population-specific risk factors. The economic burden is considerable, especially in resource-limited settings, where treatment costs often result in catastrophic out-of-pocket expenditure. Vitamin D plays a central role in calcium homeostasis, bone mineralization, muscle strength, and neuromuscular coordination. Deficiency leads to impaired bone quality, secondary hyperparathyroidism, sarcopenia, and increased fall risk [8,9]. Despite abundant sunlight, Vitamin D deficiency is alarmingly prevalent in India due to factors such as high skin melanin content, limited sun exposure, air pollution, dietary inadequacies, and lack of food fortification. Prevalence rates of hypovitaminosis D in India range from 50% to 90% across different age groups [10,11,12,13,14,15]. Although the association between Vitamin D deficiency and hip fractures is well documented, most studies focus on deficiency as a binary variable rather than examining graded levels of deficiency. Understanding how different severities of Vitamin D deficiency relate to fracture patterns may help refine preventive strategies and clinical guidelines.
An observational cross-sectional study was carried out in the Department of Orthopaedics, School of Medical Sciences and Research, Sharda University, Greater Noida, India, between April 2024 and November 2025. The study was initiated after obtaining approval from the Institutional Ethics Committee (SU/SMS&R/76-A/2024/116 dated April 04, 2024), and all procedures were performed in accordance with the ethical standards laid down in the Declaration of Helsinki. Written informed consent was obtained from all participants or their legally authorised representatives before enrolment. The study population comprised adult patients presenting with hip fractures following low-energy trauma. Female patients aged 50 years and above and male patients aged 60 years and above were included in the study, reflecting the age groups at higher risk for osteoporotic and fragility fractures. Eligible fracture types included fractures of the neck of the femur, intertrochanteric fractures, and subtrochanteric fractures. Patients with high-velocity injuries such as road traffic accidents; pathological fractures; isolated avulsion fractures of the greater or lesser trochanter; previous fractures at the same site; or those already receiving Vitamin D supplementation were excluded to avoid confounding factors. The sample size was calculated using Cochran’s formula, taking an estimated prevalence of hip fractures of 10%, a confidence interval of 95%, and a margin of error of 10%. The calculated minimum sample size was 35; however, to improve the robustness of the analysis, a total of 50 patients were ultimately enrolled. On admission, detailed demographic information, including age and sex, was recorded for each participant. Fracture diagnosis and classification were confirmed using standard radiographic evaluation. Fracture types were categorised as intertrochanteric, neck of femur, or subtrochanteric fractures, and laterality was documented. Venous blood samples were collected from all participants at the time of admission, before any surgical intervention or initiation of supplementation. Serum 25-hydroxyvitamin D levels were measured using the VITROS 5600 dry chemistry autoanalyser in the central laboratory of Sharda Hospital. Based on serum vitamin D concentrations, patients were categorised into four groups: severe deficiency (<10 ng/mL), moderate deficiency (10–20 ng/mL), insufficiency (20–30 ng/mL), and sufficiency (>30 ng/mL). The primary objective of the study was to assess the association between graded levels of vitamin D deficiency and the occurrence of hip fractures. The secondary objectives included evaluation of fracture patterns across age groups and genders and determination of the relationship between fracture subtype and vitamin D status. All data were entered into Microsoft Excel and subsequently analysed using the Statistical Package for the Social Sciences version 26.0, IBM Corp, Chicago, Illinois, USA. The distribution of quantitative variables was assessed for normality using the Kolmogorov–Smirnov test. Categorical variables were expressed as frequencies and percentages. Associations between categorical variables, including age group, gender, fracture type, and vitamin D status, were analysed using the chi-square test. A P < 0.05 was considered statistically significant for all analyses.
A total of 50 patients with hip fractures were included in the present study. The study population predominantly comprised elderly individuals. As shown in Table 1, the highest proportion of patients belonged to the 70–79 years age group (52.08%), followed by the 60–69 years group (20.83%) and those aged ≥70 years (14.58%).
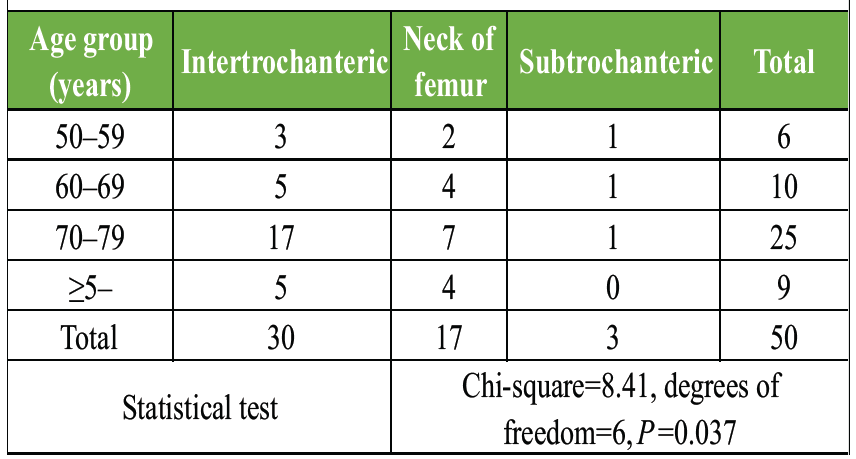
Table 1: Distribution of fracture type by age group
Patients aged 50–59 years constituted the smallest proportion (12.5%). With regard to gender distribution, there was a near-equal representation, with 27 males (54%) and 23 females (46%). In both males and females, the 70–79-year age group accounted for the highest number of fractures, contributing to more than half of the total cases. Males slightly predominated in the 60–69 and ≥60 years age groups, whereas females marginally outnumbered males in the 70–79 years group. However, statistical analysis revealed no significant association between age group and gender (χ2 = 0.36, P = 0.949), indicating a similar age-wise fracture distribution across both sexes. Intertrochanteric fractures were the most common, observed in 30 patients (60%), followed by neck of femur fractures in 17 patients (34%). Subtrochanteric fractures were relatively uncommon, accounting for only 3 cases (6%). The distribution of fracture types was found to be statistically significant (P < 0.001), with intertrochanteric fractures occurring more frequently than other types. When fracture patterns were analysed across different age groups (Table 1 and Fig. 1), intertrochanteric fractures predominated in all age categories, particularly in the 70–79 years group, which alone contributed 17 of the 30 intertrochanteric fractures.
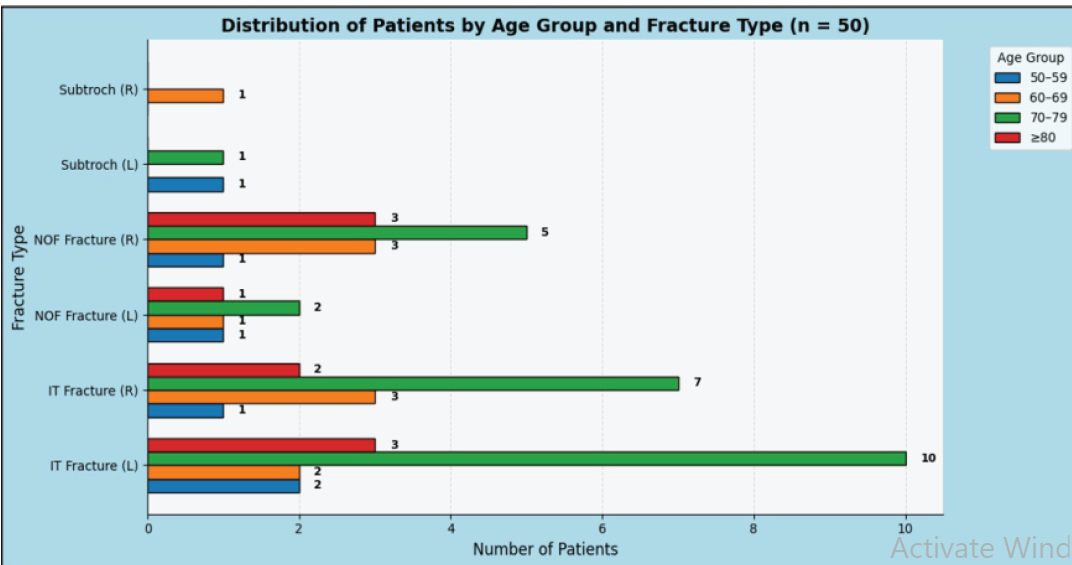
Figure 1: Distribution of patients by age group and fracture type (n=50).
Neck of femur fractures were also common in the elderly, especially in patients aged ≥70 years, while subtrochanteric fractures were infrequent across all age groups. The association between age group and fracture type was found to be statistically significant (χ2 = 8.41, P = 0.037), suggesting age-related variation in fracture patterns. Serum vitamin D status of the study population is summarised in Table 2.
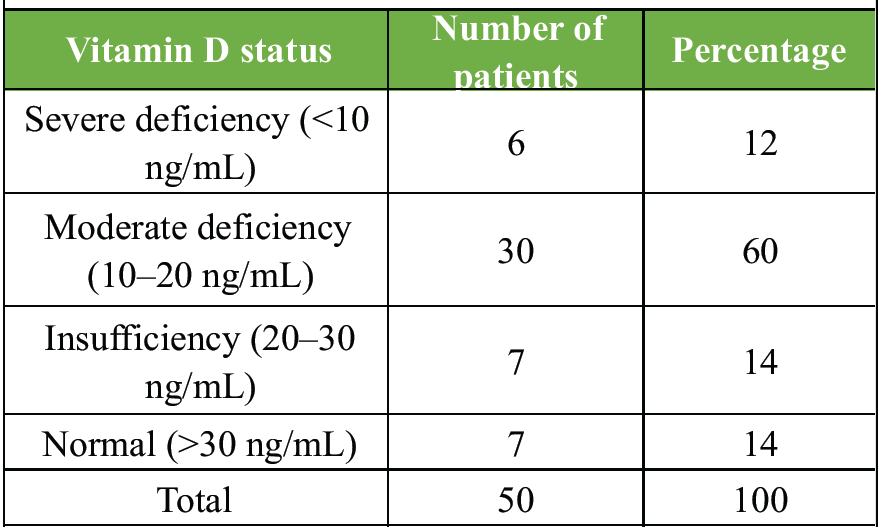
Table 2: distribution of patients by serum Vitamin D status
A substantial majority of patients exhibited vitamin D deficiency. Moderate deficiency (10–20 ng/mL) was the most prevalent category, observed in 60% of patients, followed by severe deficiency (<10 ng/mL) in 12%. Vitamin D insufficiency (20–30 ng/mL) and normal levels (>30 ng/mL) were each observed in 14% of patients. Overall, 72% of patients had vitamin D deficiency (severe or moderate) in Fig. 2.
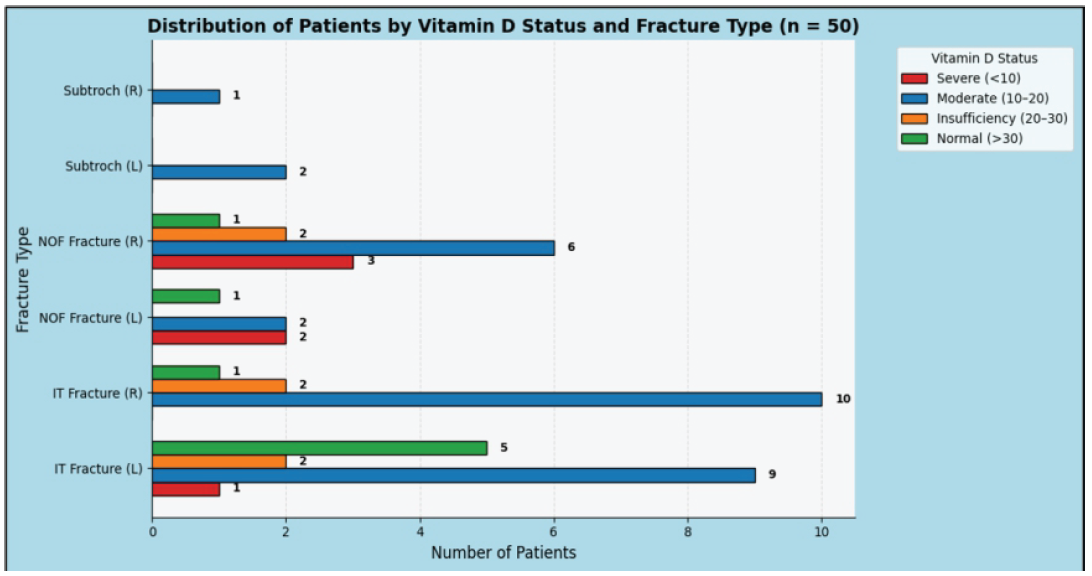
Figure 2: Distribution of patients by Vitamin D status and fracture type (n=50).
The relationship between vitamin D status and fracture type is illustrated in Table 3.
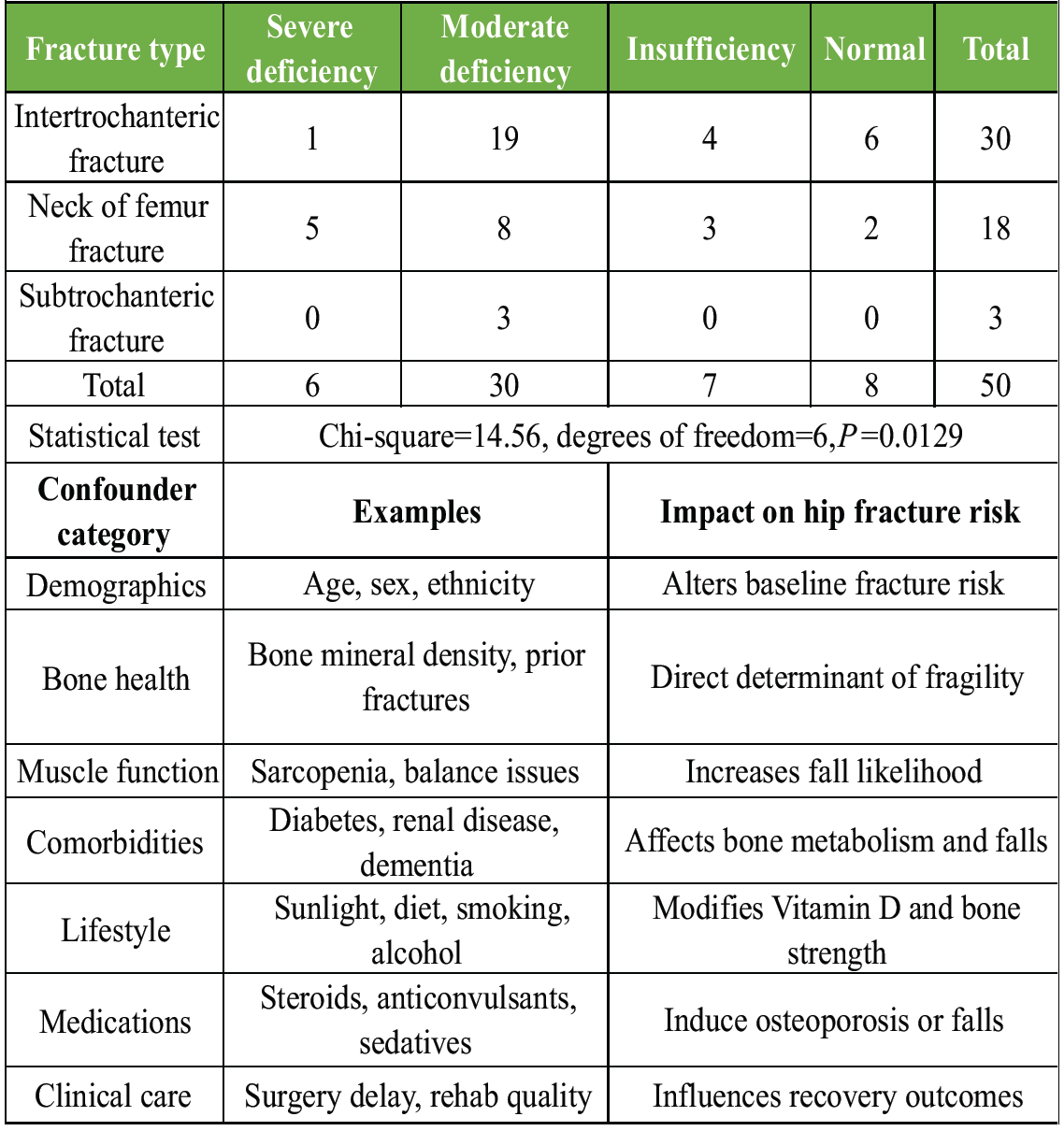
Table 3: Association between Vitamin D status and fracture type
Among patients with intertrochanteric fractures, the majority had moderate vitamin D deficiency, accounting for 19 of 30 cases (63.3%), while severe deficiency was uncommon in this group. In contrast, neck-of-femur fractures showed a higher proportion of severe vitamin D deficiency, with 5 of 17 patients (29.4%) falling into this category. All subtrochanteric fractures were observed exclusively in patients with moderate vitamin D deficiency. Statistical analysis demonstrated a significant association between serum vitamin D levels and fracture type (χ2 = 14.56, P = 0.0129). Overall, the results indicate that hip fractures in the Indian population predominantly affect the elderly, with intertrochanteric fractures being the most common subtype. Vitamin D deficiency was highly prevalent and showed a significant relationship with fracture patterns, with increasing severity of deficiency being more pronounced in neck-of-femur fractures. These findings support the role of vitamin D status as an important modifiable factor influencing hip fracture risk and fracture subtype.
The present cross-sectional study evaluated the association between different levels of serum vitamin D deficiency and hip fractures in an Indian population. The analysis focused on demographic characteristics, fracture patterns, and the relationship between graded Vitamin D deficiency and fracture subtype. The findings provide clinically relevant insights into the metabolic and epidemiological determinants of hip fractures in India. Hip fractures in the present study predominantly affected the elderly, with more than half of the patients belonging to the 70–79 years age group. This age-related predominance is well documented and reflects the cumulative effects of aging on skeletal integrity, including reduced bone mineral density (BMD), sarcopenia, impaired balance, and increased fall risk [1,2,3]. Similar age distributions have been reported in Indian and international studies, confirming that hip fracture incidence peaks in the seventh and eighth decades of life [2,3]. These findings emphasize aging as a critical, non-modifiable risk factor for hip fractures. With respect to gender distribution, the present study showed a near-equal representation of males and females, with no statistically significant difference in fracture occurrence. This finding contrasts with several Western studies that report a female predominance due to postmenopausal osteoporosis [1,3]. However, Indian studies have demonstrated more balanced gender distributions, possibly reflecting differences in lifestyle, occupational exposure, nutritional status, and sun exposure [2,9]. Khan et al. similarly reported no significant gender-based difference in fracture risk once Vitamin D deficiency was considered [13]. These observations suggest that, in the Indian context, metabolic factors and aging may play a more dominant role than sex alone. Intertrochanteric fractures were the most common fracture subtype in this study, accounting for 60% of cases, followed by neck of femur fractures (34%) and subtrochanteric fractures (6%). This pattern is consistent with previous Indian studies and epidemiological data from Asia, where intertrochanteric fractures predominate among elderly individuals with fragility fractures [9,10]. The intertrochanteric region, rich in cancellous bone, is particularly susceptible to metabolic bone disease and secondary hyperparathyroidism associated with Vitamin D deficiency [8]. Age-wise analysis revealed that intertrochanteric fractures predominated across all age groups, especially in patients aged 70–79 years, whereas neck of femur fractures were relatively more frequent among those aged ≥ge years. Subtrochanteric fractures were uncommon across all age categories. These findings align with the observations of Kanno et al., who demonstrated that different hip fracture subtypes exhibit distinct biochemical profiles, particularly with respect to serum Vitamin D and parathyroid hormone levels [11]. The higher proportion of neck of femur fractures in the oldest age group may reflect more severe cortical bone loss and advanced skeletal fragility. Vitamin D deficiency emerged as a striking and consistent finding in the present study. Overall, 72% of patients had Vitamin D deficiency, with moderate deficiency (10–20 ng/mL) being the most prevalent category. These results are in close agreement with multiple Indian and international studies, which consistently report high rates of hypovitaminosis D among patients presenting with hip fractures [6,7,8,10]. Dhanwal et al. demonstrated that Indian hip fracture patients commonly have Vitamin D deficiency accompanied by secondary hyperparathyroidism, further exacerbating bone loss and fracture risk [8]. A key observation of this study was the statistically significant association between fracture type and vitamin D status. Intertrochanteric fractures were most frequently associated with moderate Vitamin D deficiency, whereas severe deficiency was disproportionately observed among patients with neck of femur fractures. All subtrochanteric fractures occurred in patients with moderate deficiency. This suggests that while moderate deficiency acts as a broad predisposing factor for hip fractures, severe deficiency may have a more specific association with femoral neck fractures. Similar fracture subtype–specific biochemical variations have been reported by Kanno et al., supporting the concept that metabolic severity may influence fracture location [11]. The clinical implications of Vitamin D deficiency extend beyond fracture occurrence. Meta-analyses by Llombart et al. and Wang et al. have demonstrated that vitamin D deficiency is associated with significantly increased post-fracture mortality [14,15]. Furthermore, Vitamin D deficiency has been linked to impaired muscle function, reduced mobility, delayed functional recovery, and poorer quality of life following hip fracture surgery [4,5]. These findings highlight Vitamin D deficiency as a modifiable risk factor with implications for both fracture prevention and post-fracture outcomes. The strength of the present study lies in its evaluation of graded Vitamin D deficiency in relation to hip fracture subtypes within an Indian population, addressing an important gap in existing literature. However, the study is limited by its modest sample size and single-center design, which may limit generalizability. In addition, confounding parameters such as diabetes mellitus, chronic kidney disease, bone health (BMD and prior fractures), muscle function (sarcopenia), lifestyle changes (smoking, alcohol, and diet), medications (steroids, anticonvulsants, and sedatives), and nutritional status were not evaluated and may have influenced vitamin D levels and fracture risk [13].
High prevalence of vitamin D deficiency was observed among Indian patients with hip fractures, with intertrochanteric fractures most common and femoral neck fractures linked to severe deficiency. Findings indicate hypovitaminosis D contributes to skeletal fragility and may influence fracture patterns. Routine screening and timely supplementation in elderly individuals, particularly those at risk of falls, could reduce fracture incidence and severity. Larger multicentric studies incorporating broader metabolic and clinical variables are warranted to clarify the relationship between vitamin D status, fracture types, and long-term outcomes, reinforcing its role as a modifiable risk factor.
- Vitamin D deficiency is highly prevalent among elderly Indian patients with hip fractures, underscoring the need for routine screening in at-risk populations
- Graded severity of deficiency influences fracture subtype – moderate deficiency is most often linked to intertrochanteric fractures, while severe deficiency shows a stronger association with femoral neck fractures
- Early correction of hypovitaminosis D may reduce fracture incidence and improve outcomes, making supplementation a practical, cost-effective preventive strategy in geriatric care.
References
- 1. Johnell O, Kanis JA. An estimate of the worldwide prevalence, mortality and disability associated with hip fracture. Osteoporosis Int 2004;15:897-902. [Google Scholar] [PubMed]
- 2. Dhanwal DK, Dennison EM, Harvey NC, Cooper C. Epidemiology of hip fracture: Worldwide geographic variation. Indian J Orthop 2011;45:15-22. [Google Scholar] [PubMed]
- 3. Cooper C, Campion G, Melton LJ 3rd. Hip fractures in the elderly: A world-wide projection. Osteoporos Int 1992;2:285-9. [Google Scholar] [PubMed]
- 4. Holick MF. Vitamin D deficiency. N Engl J Med 2007;357:266-81. [Google Scholar] [PubMed]
- 5. Bischoff-Ferrari HA, Dawson-Hughes B, Staehelin HB, Orav JE, Stuck AE, Theiler R, et al. Fall prevention with supplemental and active forms of vitamin D: A meta-analysis of randomized controlled trials. BMJ 2009;339:b3692. [Google Scholar] [PubMed]
- 6. Harinarayan CV, Joshi SR. Vitamin D status in India–Its implications and remedial measures. J Assoc Physicians India 2009;57:40-8. [Google Scholar] [PubMed]
- 7. Cauley JA, Lacroix AZ, Wu L, Horwitz M, Danielson ME, Bauer DC, et al. Serum 25-hydroxyvitamin D concentrations and risk for hip fractures. Ann Intern Med 2008;149:242-50. [Google Scholar] [PubMed]
- 8. Dhanwal DK, Sahoo S, Gautam VK, Saha R. Hip fracture patients in India have vitamin D deficiency and secondary hyperparathyroidism. Osteoporosis Int 2013;24:553-7. [Google Scholar] [PubMed]
- 9. Ahuja K, Sen S, Dhanwal D. Risk factors and epidemiological profile of hip fractures in Indian population: A case-control study. Osteoporos Sarcopenia 2017;3:138-48. [Google Scholar] [PubMed]
- 10. Khadgawat R, Brar KS, Gahlo M, Yadav CS, Malhotra R, Guptat N, et al. High prevalence of vitamin D deficiency in Asian-Indian patients with fragility hip fracture: A pilot study. J Assoc Physicians India 2010;58:539-42. [Google Scholar] [PubMed]
- 11. Kanno A, Aizawa T, Mori Y, Aizawa T. Different types of hip fragility fractures have different values of 25-hydroxyvitamin D and parathyroid hormone. J Orthop Sci 2022;28:567-73. [Google Scholar] [PubMed]
- 12. Rehman S, Bukhari S, Khan Z, Shah S. Frequency of vitamin D deficiency in patients with low energy hip fracture. Pak J Intensive Care Med 2025;5:125. [Google Scholar] [PubMed]
- 13. Khan Z, Swati M, Zeb S, Ashraf, Rumman, Sohail A, et al. Assessing the predictive value of serum vitamin D levels for hip fracture risk in older adults and identifying associated risk factors. Cureus 2025;17:e82603. [Google Scholar] [PubMed]
- 14. Llombart R, Mariscal G, Barrios C, De la Rubia Ortí JE, Llombart-Ais R. Impact of vitamin D deficiency on mortality in patients with hip fracture: A meta-analysis. J Am Geriatr Soc 2023;72:268-79. [Google Scholar] [PubMed]
- 15. Wang K, Xia C, Zhou L, Zheng Y, Wang X, Cheng L. Association between vitamin D deficiency and mortality after hip fractures: A systematic review and meta-analysis. J Nutr Sci Vitaminol (Tokyo) 2024;70:89-97. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Intertrochanteric Fracture Secondary to Solitary Osteochondroma: A Case Report and Literature Review
July 1, 2026 Intertrochanteric Fracture Secondary to Solitary Osteochondroma: A Case Report and Literature Review July 1, 2026 Aseptic Discitis with Instability after Posterior Spine Surgery
July 1, 2026 Aseptic Discitis with Instability after Posterior Spine Surgery July 1, 2026 Retrograde Nailing of an Unstable Distal-Third Femoral Shaft Fracture Using Pure Indirect Reduction: A Case Report in Osteoporotic Bone
July 1, 2026 Retrograde Nailing of an Unstable Distal-Third Femoral Shaft Fracture Using Pure Indirect Reduction: A Case Report in Osteoporotic Bone July 1, 2026 Assessment of Osteoporotic Fracture Risk in Patients above 50 Years Using Quantitative Ultrasonography and Fracture Risk Assessment Tool: A Cross-sectional Study
July 1, 2026 Assessment of Osteoporotic Fracture Risk in Patients above 50 Years Using Quantitative Ultrasonography and Fracture Risk Assessment Tool: A Cross-sectional Study