
Iatrogenic instability during spine surgery is one of the known complications of spine surgery and should be assessed intraoperatively and dealt with in the same sitting with instrumented fusion; otherwise, it can lead to progressive degeneration and instability.
Dr Parimal Vairagade, Department of Orthopaedic Surgery, Apulki Vairagade Hospital, Nagpur, Maharashtra, India E-mail: pvairagade01@gmail.com
Abstract
Introduction: Lumbar canal stenosis is a common cause of low back pain occurring in the elderly population. It is treated with posterior decompression with or without fusion surgery. However, decompression can lead to iatrogenic instability in some cases and, if suspected, must be assessed intraoperatively and treated with instrumented fusion. If not addressed, it can lead to progressive degeneration and instability.
Case Report: A 58-year-old male presented with severe low back pain and functional limitation 2 years after undergoing an L4 wide laminectomy for lumbar canal stenosis. While initial post-operative recovery was favourable, the patient developed progressive pain and immobility within 2 months post-surgery, ultimately becoming bedridden. Clinical examination revealed localised lumbosacral tenderness with a Visual Analogue Scale (VAS) score of 7/10 and no neurological deficits. Laboratory investigations were unremarkable, ruling out infection. Radiological evaluation demonstrated severe osteoporosis, significant angular instability at L4-L5, and intra-discal degeneration, consistent with iatrogenic post-operative spinal instability. Given the patient’s compromised bone quality, a surgical plan was devised involving posterior fixation spanning two levels above and below the instability, using pedicle screws and a bone graft mixture without a cage to minimise the risk of implant failure. Intraoperatively, clear discal fluid was aspirated for culture and tuberculosis testing, both of which returned negative. Postoperatively, the patient was placed on strict bed rest. At 1-month follow-up, substantial clinical improvement was noted with reduced pain (VAS 4/10), improved mobility, and radiological evidence of stable instrumentation and early fusion.
Conclusion: This case report highlights the importance of recognising progressive postoperative instability as a potential delayed complication of lumbar laminectomy, particularly in osteoporotic patients, which should be addressed with a management strategy tailored to bone quality and biomechanical demands. Posterior instrumentation with interbody fusion using bone graft and bone graft substitutes has shown accelerated fusion results.
Keywords: Lumbar laminectomy, post-operative instability, iatrogenic spinal instability, osteoporosis, lumbar fixation, bone graft substitute, pedicle screw instrumentation, intra-discal fluid, aseptic disk degeneration, spinal fusion, lumbar spine surgery complications, delayed spinal instability.
Lumbar canal stenosis is a common degenerative spinal condition in elderly patients, often managed surgically through decompressive procedures such as laminectomy. While laminectomy effectively relieves neural compression and improves function, it can compromise the structural stability of the spine – particularly when wide decompression involves the resection of posterior elements, including the posterior tension band [1]. Post-operative spinal instability is a recognised complication, especially in patients with underlying risk factors such as severe osteoporosis [2,3]. Instability may present months or even years after surgery, often with progressive pain, reduced mobility, and functional decline, despite initial post-operative improvement. Accurate diagnosis through clinical evaluation and radiological imaging is essential, as symptoms can mimic infection or recurrent stenosis. Timely surgical stabilisation, tailored to bone quality and biomechanical considerations, is critical to restore spinal stability and improve patient outcomes [4,5,6,7,8,9,10,11,12].
• A 58-year-old male operated 2 years back for lumbar canal stenosis. The patient underwent an L4 wide laminectomy. After index surgery, the patient improved initially and was doing well. He started to do his daily activities and gradually lift heavy weight as well.
• Two months after index surgery, the patient developed severe low back pain. Progressively, his standing and walking distance reduced.
• Gradually, due to pain, the patient started to move due to pain and was bedridden. He could not stand due to pain
● Patient presented to our outpatient department 2 years after index surgery with significant low back ache and difficulty in turning in bed, unable to stand and walk. On further asking, he had no history of fever after surgery.
● On examination
o Severe tenderness in the lumbosacral region. Visual Analogue Scale (VAS) score 7 out of 10
The passive straight leg raising test was free, and the distal pulses okay.
o Neurology was intact.
● Patient was admitted for further management
Diagnostic assessment and interpretation
• Routine blood investigations to rule out infection were done. Complete blood count (CBC), erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP) were normal.
• X-rays, anteroposterior and lateral views, were done. The anteroposterior view showed a previous laminectomy and severe osteoporosis. Flexion-extension view in the lateral view showed severe angular instability at L4-L5 and end-plate sclerosis (Fig. 1).
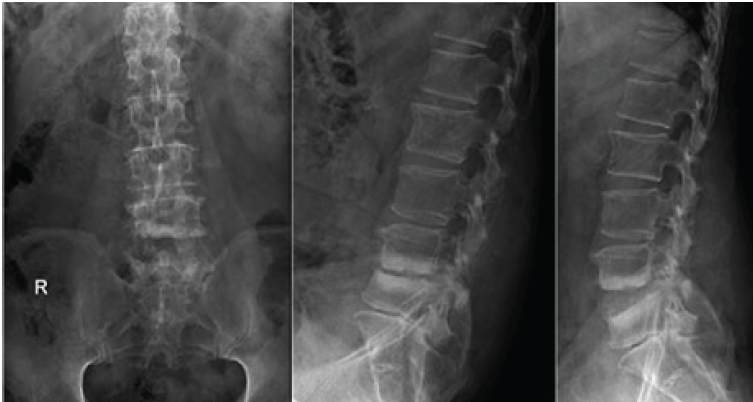
Figure 1: X-rays done at initial visit.
• Magnetic resonance imaging (MRI) done showed significant intradiscal degeneration and fluid accumulation in the disk (Fig. 2)

Figure 2: Magnetic resonance images at the time of presentation.
• Surrounding facet degeneration was also seen
• We considered that this could be the following:
o Post-operative infection
To rule that out, we did routine blood investigations such as CBC, ESR and CRP. It came out to be normal [13].
o Post-operative Instability
• Studies have shown that the chances of postoperative instability range from 43 to 55%. However, if the facets are spared, the incidence reduces to 10–43% [1,14,15,16].
• In a single-level lumbar spine surgery where the posterior tension band has been removed, the chances of postoperative instability, which leads to spondylolisthesis, are higher. As the number of decompressed levels increases, the chances of instability further increase.
Intervention
● On pre-operative planning
o On pre-operative X-rays (Fig. 1), we could anticipate severe osteoporosis. Due to this
▪ Our plan was on fixing 2 levels above and 2 levels below it.
▪ There was significant angular instability and osteoporosis, so if we were to put in a cage, there would be chances of cage back-out.
● Hence, to achieve fusion, we decided to locally harvest the bone graft and mix it with a bone graft substitute and insert it into the disc space.
● Intraoperative findings (Fig. 3 and 4)

Figure 3: Intraoperative images showing locally harvested bone graft mixed with bone graft substitute.

Figure 4: Inserting graft material into disk space with funnel.
o Violated L4 facet bilaterally,
o Broken L4 pars interarticularis
o Osteoporotic bones
o Intra-discal fluid aspirated out – clear fluid obtained and sent for culture and sensitivity, and Tubercular testing
o Pedicle screws put in, and disc space curetted and packed in with bone graft harvested locally, mixed with bone graft substitute using a funnel.
● Post-operative period
o Patient was kept lying in bed with the allowance of log rolling.
o The cultures sent for testing came out to be negative. Hence, we could conclude that this was an aseptic pathology and the causative etiology was iatrogenic instability that was caused during the index surgery and was not addressed then, which lead to progressive angular instability and disk degeneration
o Patient was discharged on post-operative day 3 after dressing and removal of the drain.
An immediate post-operative X-ray was done (Fig. 5).
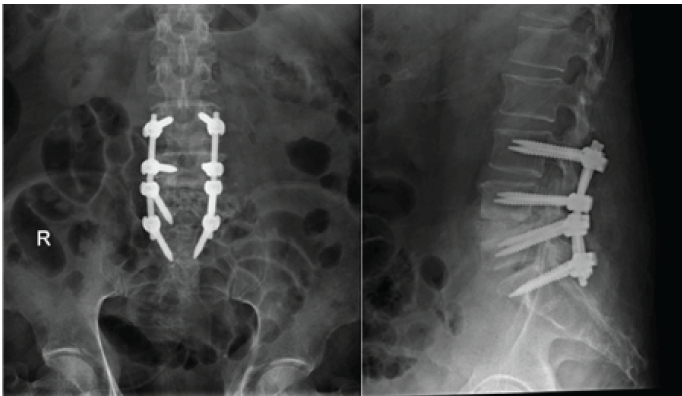
Figure 5: Immediate post-operative X-rays showing pedicle screw fixation done from L3 to S1 and L4-L5 disk space packed with bone graft and bone graft substitute.
● Postoperatively, after 1 month – the patient came for follow-up. Pain was reduced drastically.
o VAS score – 4 out of 10.
o Patient could comfortably turn in bed
o Suture line was healthy without any pus discharge
● A post-operative 1-month X-ray was done (Fig. 6)
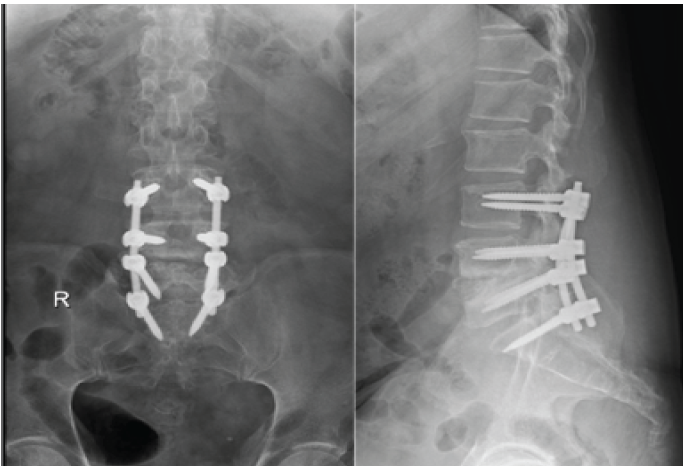
Figure 6: One-month follow-up X-ray.
o Showed good implant position; the patient was mobilized
o Satisfactory bone formation in the intradiscal area was noted
o Patient was mobilized. On mobilisation, the patient was walking with a walker, and his walking distance was improving.
Posterior lumbar decompression remains a cornerstone in the management of lumbar canal stenosis, particularly in elderly patients. While decompressive laminectomy effectively alleviates neural compression, it may inadvertently compromise spinal stability, especially when wide decompression involves resection of posterior stabilising elements such as the lamina, spinous processes, interspinous ligaments, and facet joints [1]. Iatrogenic post-operative instability is a well-recognised but often underestimated complication, with reported incidence varying widely depending on the extent of decompression, number of levels involved, and preservation of the posterior tension band [3] (Fig. 7).
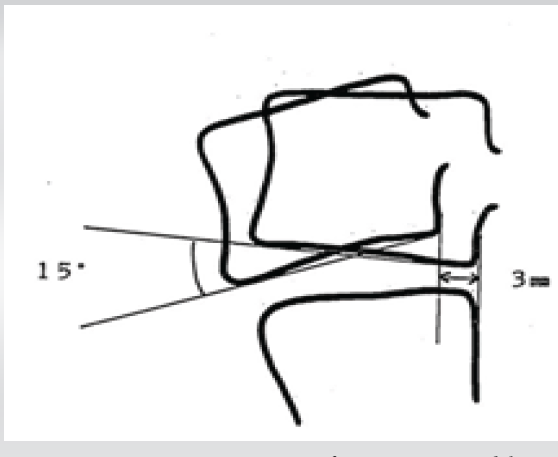
Figure 7: Diagrammatic representation of post-operative instability and how is measured.
Several studies have demonstrated that a wide laminectomy significantly alters the biomechanics of the lumbar spine, increasing segmental motion and shear forces, thereby predisposing it to progressive instability and spondylolisthesis [1,2,16]. Yang et al. [17] and Bisschop et al. [18] highlighted that factors such as facet joint violation, pre-existing degenerative changes, disc degeneration, and poor bone quality markedly increase the risk of post-operative instability. In single-level decompression, the incidence of instability may be relatively low; however, when the posterior tension band is disrupted, the likelihood of delayed instability rises substantially [14,15], as also reported by Ramhmdani et al. [19] in their case series on iatrogenic spondylolisthesis following lumbar laminectomy.
The present case illustrates a classic but delayed presentation of post-operative iatrogenic instability, where the patient initially experienced symptomatic relief after surgery but subsequently developed progressive mechanical low back pain and functional deterioration. The absence of neurological deficits, normal inflammatory markers, and lack of systemic symptoms posed a diagnostic challenge, as post-operative infection and recurrent stenosis are often considered first [13]. However, dynamic radiographs demonstrating significant angular instability at the operated level, along with MRI findings of intradiscal degeneration and fluid accumulation, were key in establishing the diagnosis. Intradiscal fluid accumulation following decompression may mimic infectious spondylodiscitis [13]; however, negative laboratory parameters and sterile intraoperative aspirate confirmed an aseptic degenerative pathology. Such aseptic disc degeneration has been described in the setting of chronic instability, where abnormal micromotion leads to disc hydration changes, endplate sclerosis, and progressive collapse [20,21]. This emphasises the importance of correlating clinical, radiological, and laboratory findings to avoid misdiagnosis and inappropriate management. Bone quality plays a pivotal role in both the development of post-operative instability and the success of revision surgery. Severe osteoporosis, as seen in our patient, not only predisposes to instability but also limits surgical options. Interbody cages, though biomechanically advantageous, carry a significant risk of subsidence, migration, and retropulsion in osteoporotic spines. Studies by Park and Chung [22] and Zhang et al. [23] have demonstrated increased implant-related complications in patients with poor bone mineral density [24]. Therefore, in the present case, a long-segment posterior fixation spanning two levels above and below the unstable segment was chosen to distribute stresses over a larger construct and minimise the risk of implant failure [25,26,27,28,29]. The decision to avoid cage insertion and instead use locally harvested autograft mixed with bone graft substitute for interbody fusion was guided by both biomechanical and biological considerations. Bone grafting provides a favourable osteoconductive and osteoinductive environment while reducing the risk of cage-related complications. Previous studies have shown satisfactory fusion rates using bone grafts and graft substitutes, particularly when combined with rigid posterior instrumentation, even in osteoporotic patients [20,21,30,31,32,33]. This case underscores the critical importance of intraoperative assessment of spinal stability during index decompression surgery. Preservation of facet joints and posterior elements, whenever feasible, and a low threshold for adding instrumented fusion in the presence of suspected instability are essential to prevent delayed complications. Newer decompression techniques, such as unilateral laminotomy for bilateral decompression [14] and “over-the-top” approaches [34] (Fig. 8), have been shown to reduce the risk of iatrogenic instability by preserving posterior stabilising structures [1,15].
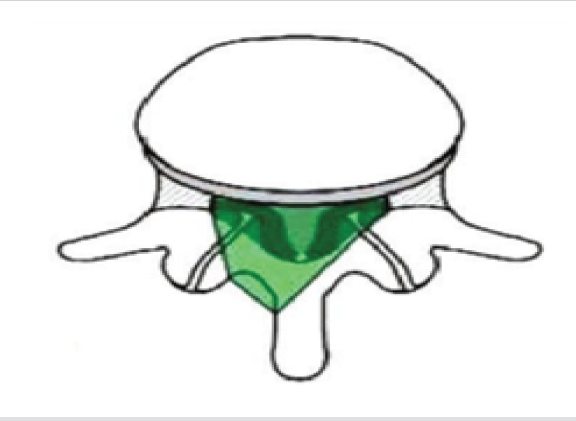
Figure 8: Diagramatic representation of over-the-top decompression.
• A good pre-operative assessment of various anatomical factors must be done using radiological images, such as X-rays and MRI, to rule out instability or factors that may contribute to instability
• When possible – Protection of posterior tension band should be done using newer techniques
• Intraoperatively – Protecting facet joint, assessment of stability must be done – if instability suspected, it must be addressed using instrumented fusion
• Multiple factors (ex: destruction of pedicle or facet, bone quality, location of instability) help in deciding levels of fixation.
• Lumbar canal stenosis is one of the common pathologies causing low back pain and dysfunction in elderly populations. During surgical planning, radiological images such as X-rays and MRI should be used to rule out instability or factors that can contribute to instability.
• Posterior decompression with or without fusion is one of the most commonly performed surgeries for lumbar canal stenosis. However, many factors can lead to instability.
• Intraoperative assessment of instability must be done, and if suspected or proven, it must be addressed with instrumented fusion. Because if left unaddressed, it can lead to progressive degeneration over time, causing progressive instability.
• This progressive instability can be addressed with long segment instrumentation, and interbody fusion using bone graft can be done. To accelerate fusion, this bone graft can be mixed with a bone graft substitute.
References
- 1. Postacchini F, Cinotti G, Perugia D, Gumina S. The surgical treatment of central lumbar stenosis. Multiple laminotomy compared with total laminectomy. J Bone Joint Surg Br 1993;75:386-92. [Google Scholar] [PubMed]
- 2. Berlemann U, Jeszenszky DJ, Bühler DW, Harms J. Facet joint remodeling in degenerative spondylolisthesis: An investigation of joint orientation and tropism. Eur Spine J 1998;7:376-80. [Google Scholar] [PubMed]
- 3. Lavelle WF, Marawar S, Bell G. Degenerative lumbar instability. Semin Spine Surg 2013;25:92-9. [Google Scholar] [PubMed]
- 4. Resnick DK, Choudhri TF, Dailey AT, Groff MW, Khoo L, Matz PG, et al. Guidelines for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 1: Introduction and methodology. J Neurosurg Spine 2005;2:637-8. [Google Scholar] [PubMed]
- 5. Resnick DK, Choudhri TF, Dailey AT, Groff MW, Khoo L, Matz PG, et al. Guidelines for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 2: Assessment of functional outcome. J Neurosurg Spine 2005;2:639-46. [Google Scholar] [PubMed]
- 6. Resnick DK, Choudhri TF, Dailey AT, Groff MW, Khoo L, Matz PG, et al. Guidelines for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 3: Assessment of economic outcome. Neurosurg Spine 2005;2:647-52. [Google Scholar] [PubMed]
- 7. Resnick DK, Choudhri TF, Dailey AT, Groff MW, Khoo L, Matz PG, et al. Guidelines for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 4: Radiographic assessment of fusion. J Neurosurg Spine 2005;2:653-7. [Google Scholar] [PubMed]
- 8. Dhall SS, Choudhri TF, Eck JC, Groff MW, Ghogawala Z, Watters WC, et al. Guideline update for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 5: Correlation between radiographic outcome and function. J Neurosurg Spine 2014;21:31-6. [Google Scholar] [PubMed]
- 9. Eck JC, Sharan A, Ghogawala Z, Resnick DK, Watters WC, Mummaneni RV, et al. Guideline update for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 7: Lumbar fusion for intractable low-back pain without stenosis or spondylolisthesis. J Neurosurg Spine 2014;21:42-7. [Google Scholar] [PubMed]
- 10. Resnick DK, Choudhri TF, Dailey AT, Groff MW, Khoo L, Matz PG, et al. Guidelines for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 8: Lumbar fusion for disk herniation and radiculopathy. J Neurosurg Spine 2005;2:673-8. [Google Scholar] [PubMed]
- 11. Resnick DK, Choudhri TF, Dailey AT, Groff MW, Khoo L, Matz PG, et al. Guidelines for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 9: Fusion in patients with stenosis and spondylolisthesis. J Neurosurg Spine 2005;2:679-85. [Google Scholar] [PubMed]
- 12. Resnick DK, Choudhri TF, Dailey AT, Groff MW, Khoo L, Matz PG, et al. Guidelines for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 10: Fusion following decompression in patients with stenosis without spondylolisthesis. J Neurosurg Spine 2005;2:686-91. [Google Scholar] [PubMed]
- 13. Krishnan A, Dave BR, Degulmadi D, Mayi S, Rai R, Bang P, et al. Early intervention in post-operative infectious spondylodiscitis: Outcome of aggressive transforaminal lumbar interbody fusion. Malays Orthop J 2024;18:16-26. [Google Scholar] [PubMed]
- 14. Tuli SM, Kapoor V, Jain AK, Jain S. Spinaplasty following lumbar laminectomy for multilevel lumbar spinal stenosis to prevent iatrogenic instability. Indian J Orthop 2011;45:396-403. [Google Scholar] [PubMed]
- 15. Lv B, Sun S, Wang H, Xiao L, Xu T, Ji P, et al. Clinical efficacy and rehabilitation of microscopic “Over the Top” for bilateral decompression in degenerative lumbar stenosis: A retrospective study. Biomed Res Int 2020;2020:7174354. [Google Scholar] [PubMed]
- 16. Rai RR, Shah Y, Shah S, Palliyil NS, Dalvie S. A radiological study of the association of facet joint tropism and facet angulation with degenerative spondylolisthesis. Neurospine 2019;16:742-7. [Google Scholar] [PubMed]
- 17. Yang JC, Kim SG, Kim TW, Park KH. Analysis of factors contributing to postoperative spinal instability after lumbar decompression for spinal stenosis. Korean J Spine 2013;10:149-54. [Google Scholar] [PubMed]
- 18. Bisschop A, Van Royen BJ, Mullender MG, Paul CP, Kingma I, Jiya TU, et al. Which factors prognosticate spinal instability following lumbar laminectomy? Eur Spine J 2012;21:2640-8. [Google Scholar] [PubMed]
- 19. Ramhmdani S, Xia Y, Xu R, Kosztowski T, Sciubba D, Witham T, et al. Iatrogenic spondylolisthesis following open lumbar laminectomy: Case Series and review of the literature. World Neurosurg 2018;113:e383-90. [Google Scholar] [PubMed]
- 20. Sims NA, Gooi JH. Bone remodeling: Multiple cellular interactions required for coupling of bone formation and resorption. Semin Cell Dev Biol 2008;19:444-51. [Google Scholar] [PubMed]
- 21. Park SB, Chung CK. Strategies of spinal fusion on osteoporotic spine. J Korean Neurosurg Soc 2011;49:317-22. [Google Scholar] [PubMed]
- 22. Zhang M, Liu X, Wang G, Liu H, Zhu F, Mou H. Risk factors associated with cage retropulsion after lumbar interbody fusion. Turk Neurosurg 2024;34:274-82. [Google Scholar] [PubMed]
- 23. Cook SD, Barbera J, Rubi M, Salkeld SL, Whitecloud TS 3rd. Lumbosacral fixation using expandable pedicle screws: An alternative in reoperation and osteoporosis. Spine J 2001;1:109-14. [Google Scholar] [PubMed]
- 24. Ferguson SJ, Winkler F, Nolte LP. Anterior fixation in the osteoporotic spine: Cut-out and pullout characteristics of implants. Eur Spine J 2002;11:527-34. [Google Scholar] [PubMed]
- 25. Aydogan M, Ozturk C, Karatoprak O, Tezer M, Aksu N, Hamzaoglu A. The pedicle screw fixation with vertebroplasty augmentation in the surgical treatment of the severe osteoporotic spines. J Spinal Disord Tech 2009;22:444-7. [Google Scholar] [PubMed]
- 26. Burval DJ, Mclain RF, Milks R, Inceoglu S. Primary pedicle screw augmentation in osteoporotic lumbar vertebrae: Biomechanical analysis of pedicle fixation strength. Spine (Phila Pa 1976) 2007;32:1077-83. [Google Scholar] [PubMed]
- 27. Kim KH, Lee SH, Lee DY, Shim CS, Maeng HM. Anterior bone cement augmentation in anterior lumbar interbody fusion and percutaneous pedicle screw fixation in patients with osteoporosis. J Neurosurg Spine 2010;12:525-32. [Google Scholar] [PubMed]
- 28. Takahata M, Ito M, Abe Y, Abumi K, Minami A. The effect of anti-resorptive therapies on bone graft healing in an ovariectomized rat spinal arthrodesis model. Bone 2008;43:1057-66. [Google Scholar] [PubMed]
- 29. Lehman RA, Kuklo TR, Freedman BA, Cowart JR, Mense MG, Riew KD. The effect of alendronate sodium on spinal fusion: A rabbit model. Spine J 2004;4:36-43. [Google Scholar] [PubMed]
- 30. Huang RC, Khan SN, Sandhu HS, Metzl JA, Cammisa FP, Zheng F, et al. Alendronate inhibits spine fusion in a rat model. Spine (Phila Pa 1976) 2005;30:2516-22. [Google Scholar] [PubMed]
- 31. Vaz K, Verma K, Protopsaltis T, Schwab F, Lonner B, Errico T. Bone grafting options for lumbar spine surgery: A review examining clinical efficacy and complications. SAS J 2010;4:75-86. [Google Scholar] [PubMed]
- 32. Lv B, Sun S, Wang H, Xiao L, Xu T, Ji P, et al. Clinical efficacy and rehabilitation of microscopic “Over the Top” for bilateral decompression in degenerative lumbar stenosis: A retrospective study. Biomed Res Int 2020;2020:7174354. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Radiological Outcomes of Reamed Short Proximal Femoral Nailing in Intertrochanteric Fractures in Patients Aged 50 Years and Above
August 1, 2026 Radiological Outcomes of Reamed Short Proximal Femoral Nailing in Intertrochanteric Fractures in Patients Aged 50 Years and Above July 1, 2026 Retrograde Nailing of an Unstable Distal-Third Femoral Shaft Fracture Using Pure Indirect Reduction: A Case Report in Osteoporotic Bone
July 1, 2026 Retrograde Nailing of an Unstable Distal-Third Femoral Shaft Fracture Using Pure Indirect Reduction: A Case Report in Osteoporotic Bone July 1, 2026 Association of Different Levels of Vitamin D Deficiency and Hip Fracture in Indian Population: A Cross-sectional Study
July 1, 2026 Association of Different Levels of Vitamin D Deficiency and Hip Fracture in Indian Population: A Cross-sectional Study July 1, 2026 Assessment of Osteoporotic Fracture Risk in Patients above 50 Years Using Quantitative Ultrasonography and Fracture Risk Assessment Tool: A Cross-sectional Study
July 1, 2026 Assessment of Osteoporotic Fracture Risk in Patients above 50 Years Using Quantitative Ultrasonography and Fracture Risk Assessment Tool: A Cross-sectional Study