
Nerve transfers effectively restore shoulder abduction and elbow flexion in upper brachial plexus injuries, though recovery of external rotation remains less predictable.
Dr. Rachit Bhatnagar, Department of Orthopaedic Surgery, Ganesh Shankar Vidyarthi Medical College, Kanpur, Uttar Pradesh, India. E-mail: princerachit@gmail.com
Abstract
Objectives: The objective of the study is to evaluate the functional outcomes of nerve transfer procedures in adults with post-traumatic irreparable upper root brachial plexus injuries (BPIs).
Material and Methods: Design: Retrospective cohort study. Setting: Single-centre study conducted at a multi-super-speciality tertiary care hospital. Patient Selection Criteria: Adult patients aged 18–42 years with post-traumatic upper root BPIs (C5–C7) who underwent nerve transfer surgery within 10 months of injury were included. Patients with prior brachial plexus surgery, associated central nervous system injury, or incomplete follow-up were excluded. Outcome Measures and Comparisons: Primary outcome measures included recovery of active shoulder abduction, external rotation, and elbow flexion, assessed using the British Medical Research Council grading system. Outcomes were evaluated at the final follow-up and compared with pre-operative functional status.
Results: A total of 26 patients were included, with a mean follow-up duration of 24 months. Statistically significant recovery was observed in shoulder abduction in 88.5% of patients (P < 0.001) and elbow flexion in 84.6% of patients (P < 0.001). Recovery of external rotation was achieved in 30.77% of patients and did not reach statistical significance (P = 0.076). No intraoperative or post-operative complications were reported.
Conclusion: Nerve transfer procedures resulted in significant functional improvement in adults with upper root BPIs. Shoulder abduction and elbow flexion demonstrated reliable recovery following nerve transfer surgery. Restoration of external rotation remained inconsistent and represents an area for further investigation.
Keywords: Brachial plexus injuries, nerve transfer, shoulder abduction, elbow flexion, external rotation.
Brachial plexus injuries (BPIs) are debilitating and painful conditions that result in a loss of function and quality of life. These injuries occur when the network of nerves supplying the shoulder, arm, forearm, and hand is damaged [1]. The brachial plexus consists of the anterior rami of the spinal nerves C5 to T1 and is responsible for motor and sensory functions in the upper limb [2]. BPIs can have various causes, including trauma, obstetric injury, or iatrogenic factors. Traumatic BPIs are commonly caused by motor vehicle accidents, falls, sports injuries, and gunshot wounds [3]. Obstetric BPIs (such as Erb’s and Klumpke’s palsies) typically result from excessive pulling on the baby’s shoulders during delivery, particularly in complicated births [4]. The severity of a BPI is classified according to the anatomical injury scale, with degrees ranging from mild to severe, depending on the extent of nerve damage. Mild injuries may cause temporary weakness or numbness, while severe injuries can result in complete paralysis and loss of sensation [5]. The functional impact of a BPI can be significant, hindering an individual’s ability to perform activities of daily living, work, or engage in social activities. Treatment for BPIs depends on various factors, including the severity of the injury, the type of damage, the time elapsed since the injury, and any other underlying conditions. Nerves that are only stretched may recover without intervention. However, surgery is often the most effective option for more serious nerve injuries [6]. Nerve transfers have emerged as a promising technique for reconstructing damaged nerves in BPIs. This method involves transferring expendable donor nerves and suturing them to the affected parts of the plexus [7].
Study design and setting:
This retrospective cohort study was conducted at a multi-super-speciality tertiary care hospital in northern India between June 2022 and May 2024. Institutional Ethics Committee approval was obtained before initiation of the study (IEC reference number: RHL-IEC-160152).
Study population:
The medical records of 26 adult patients who underwent nerve transfer (neurotisation) procedures for post-traumatic irreparable BPIs were reviewed. The mean age of the study population was 29.35 years (range: 18–42 years).
Inclusion criteria:
Patients were included if they had:
- Post-traumatic irreversible injuries involving the upper roots of the brachial plexus (C5, C6, and/or C7 in various combinations)
- Undergone surgical intervention within 10 months of injury
- Completed a minimum postoperative follow-up of 12 months.
“Irreparable” roots were defined as spinal nerve roots deemed unsuitable for direct repair or grafting due to avulsion or severe fibrosis, rendering them unfit for use as donor nerves.
Clinical evaluation and outcome measures:
Postoperative functional assessment focused on three primary outcomes: Active shoulder abduction, active elbow flexion, and useful external rotation. Shoulder external rotation was assessed with the arm adducted alongside the trunk and initially placed in full internal rotation [8]. Shoulder abduction was evaluated against gravity. Elbow flexion was considered functional when active complete flexion was achieved with wrist extension, in conjunction with approximately 90° of shoulder girdle abduction and depression [9]. Upper extremity motor recovery was graded using the British Medical Research Council (BMRC) grading system [10]. For statistical analysis, one-sample t-tests were applied to determine whether the observed mean recovery proportions were significantly different from a reference value of 0.5. Sensory recovery, pain scores, patient-reported outcome measures, quality-of-life assessments, hand function, and return-to-work status were not routinely documented and therefore were not included in the present analysis.
Nerve transfers:
Nerve transfers, also known as neurotization, involve repairing a distal denervated nerve using a proximal donor nerve to provide neurons and axons for re-innervation of the distal targets [11]. This approach sacrifices the function of a less critical donor muscle to restore functionality in the recipient nerve and muscle. The underlying anatomical and physiological principles are relatively simple. Since the primary goal is motor recovery, selecting a donor nerve with a sufficient number of motor fibers is essential. In addition, the loss of function in the donor muscle must not result in a significant functional deficit. The neuromuscular element being reinnervated should provide a functional benefit that far outweighs the loss incurred from sacrificing the donor nerve [12]. The distribution of patients in different groups of brachial plexus nerve transfer is as mentioned in Table 1.
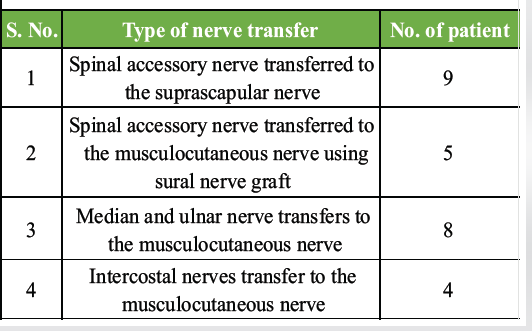
Table 1: Frequency of various nerve transfers
Surgical technique:
Spinal accessory nerve (SAN) transfer to suprascapular nerve:
The suprascapular and SANs were exposed through an oblique incision extending from the point where the brachial plexus crosses the clavicle to the anterior border of the trapezius muscle. Following skin and subcutaneous dissection, the clavicular head of the sternocleidomastoid muscle was retracted to provide access to the posterior triangle. The SAN was identified coursing on the deep surface of the trapezius and carefully dissected distally to gain adequate length for transfer. The suprascapular nerve was identified at its origin from the upper trunk of the brachial plexus, proximal to its passage through the suprascapular notch. Care was taken to preserve adjacent vascular structures and to ensure sufficient mobilization of both nerves. Once adequate length was achieved, the SAN was divided distally, and a direct, tension-free end-to-end coaptation was performed with the suprascapular nerve under an operating microscope using 8-0 or 9-0 nylon sutures supplemented with fibrin glue. This transfer re-innervates the supraspinatus and infraspinatus muscles, thereby restoring active shoulder abduction and external rotation. Hemostasis was secured, the wound was closed in layers, and the limb was immobilized postoperatively in a shoulder arm pouch for 2–3 weeks before initiating physiotherapy. In our study, 9 patients had the SAN transferred to the suprascapular nerve during brachial plexus reconstruction to restore shoulder function (Fig. 1a, b, c) [13]. This procedure was completed without the use of nerve grafts in all cases.
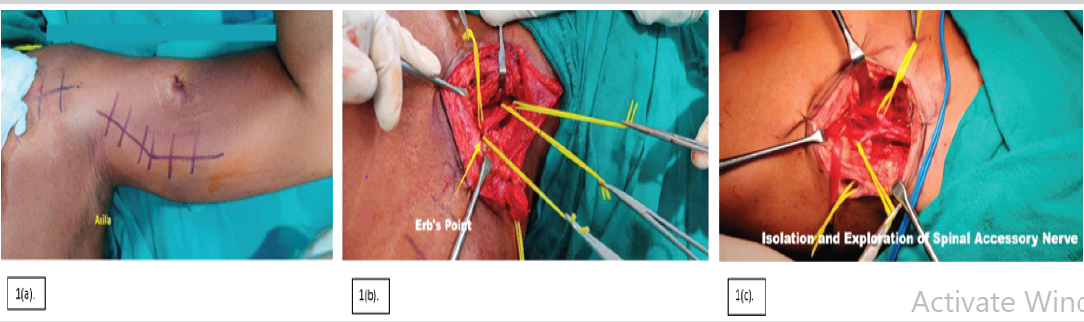
Figure 1: (a) Incision mark at the arm (for exploration of nerves) and shoulder (for exploration of Erb’s point). (b) Exploration of Erb’s point. (c). Isolation and tagging of spinal accessory nerve.
SAN transfer to musculocutaneous nerve (MCN) using sural nerve graft:
With the patient in the supine position, a supraclavicular incision was made to expose the SAN in the posterior triangle. The SAN was dissected proximally for adequate length. Through a separate anteromedial arm incision, the MCN and its motor branch to the biceps were identified. The sural nerve was harvested through longitudinal leg incisions, reversed, and tunnelled subcutaneously from the neck to the arm. Under microscopic magnification, the SAN was coapted to the proximal end of the graft, and the distal graft was coapted to the biceps branch of the MCN using 8-0/9-0 nylon sutures and fibrin glue. The arm was immobilised postoperatively in 90° elbow flexion, followed by progressive physiotherapy. In 05 patients with global BPI, the SAN was transferred to the MCN with the aid of an interposed sural nerve graft to restore elbow flexion (Figs. 2a and b; 3a and b) [14].
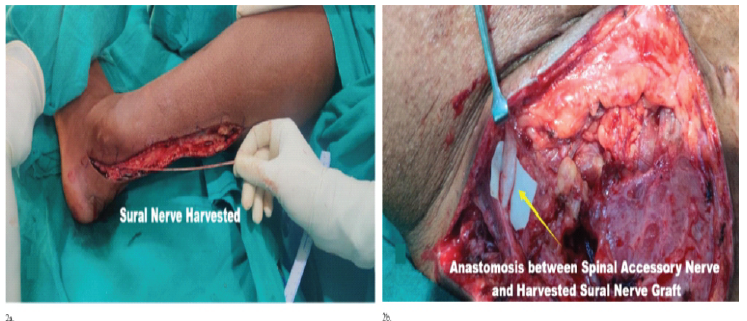
Figure 2: (a) Harvesting sural nerve graft figure. (b) Anastomosis between spinal accessory nerve and harvested sural nerve graft.
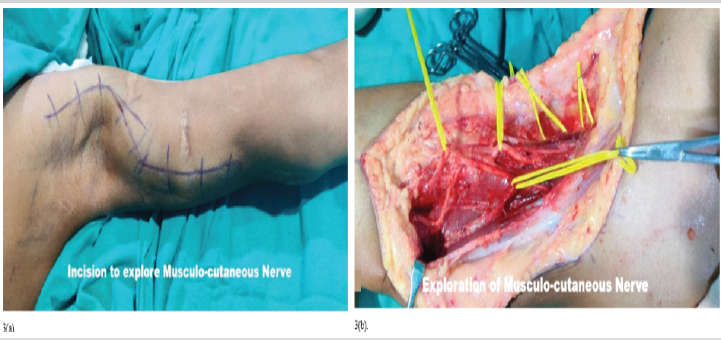
Figure 3: (a) Incision to explore musculocutaneous nerve. (b) Exploration of musculocutaneous nerve.
Double Oberlin nerve transfer:
The Double Oberlin procedure is performed with the patient in the supine position, the affected arm abducted to 90° on an arm board or hand table, and the limb prepared in a sterile fashion to the axilla. Intraoperative electromyography is used for donor fascicle identification, with electrodes placed in the median and ulnar innervated muscles. A longitudinal incision, 8–10 cm in length, is made along the biceps-triceps groove, guided by the brachial artery pulse. The median nerve (MN) is identified adjacent to the brachial artery, while the ulnar nerve (UN) lies medial and posterior. The MCN is exposed between the biceps and brachialis muscles, with its branches to the biceps and brachialis carefully preserved. Under microsurgical magnification, internal neurolysis of MN and UN is performed to isolate appropriate donor fascicles. A lateral fascicle of the MN, preferentially innervating wrist flexors or pronator teres, is coapted to the brachialis branch of the MCN. A fascicle from the UN, with minimal intrinsic hand contribution, is transferred to the biceps branch. Tension-free coaptation is achieved using 8-0 or 9-0 nylon sutures and fibrin glue without nerve grafts. Postoperatively, the elbow is immobilised at 90° flexion for 2–3 weeks, followed by progressive physiotherapy to restore motion and strengthen reinnervation. Median and UN transfers to MCN are performed in 8 patients (Fig. 4a, b, c)

Figure 4: (a) Incision to explore musculocutaneous nerve and median nerve. (b) Transfer of ulnar nerve fascicle to biceps branch of musculocutaneous nerve. (c) Exploration of median nerve.
Intercostal nerve transfer to the MCN transfer:
Intercostal nerve transfer to the MCN was performed with the patient in the supine position. A curvilinear incision was made along the inframammary region to expose the third to fifth intercostal spaces. The intercostal nerves were identified beneath the costal cartilages, dissected proximally to their origins, and mobilized distally with preservation of intercostal vessels. Small muscular branches were divided to obtain sufficient length. Through a separate incision along the anteromedial arm, the MCN was exposed between the biceps and brachialis muscles and traced proximally to its motor branches. The selected intercostal nerves were tunnelled subcutaneously to the axilla and coapted end-to-end with the motor branches of the MCN under the operating microscope. Microsurgical neurorrhaphy was performed using 8-0 or 9-0 nylon sutures supplemented with fibrin glue, ensuring tension-free repair. Haemostasis was achieved and incisions were closed in layers. Postoperatively, the arm was immobilised for 2 weeks, followed by gradual physiotherapy to restore elbow flexion. Intercostal nerve transfers to the MCN were performed in 04 patients to restore active elbow flexion (Fig. 5a and b) [15]. Although all patients underwent structured post-operative physiotherapy, individual compliance, rehabilitation intensity, and attendance varied and were not independently quantified or analysed.
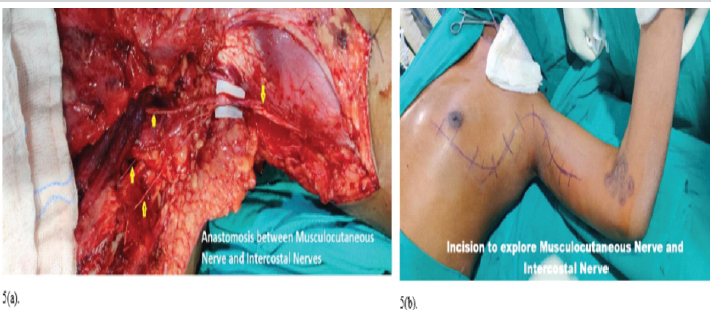
Figure 5: (a) Anastomosis between musculocutaneous nerve and intercostal nerves. (b) Incision to explore musculocutaneous nerve and intercostal nerve.
The study cohort consisted of 26 patients with upper root BPIs, with a mean age of 29.35 years (standard deviation ±7.32; range 18–42 years). The age distribution indicated that the majority of patients were in their third decade of life, reflecting the high incidence of such injuries among young, active individuals. In the study cohort, 21 (80.77%) were male and 5 (19.23%) were female patients. The demographic and baseline characteristics of the study population are shown in Table 2.
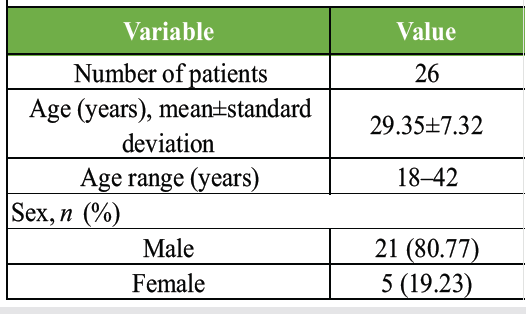
Table 2: Demographic and baseline characteristics of the study population (n=26)
Pre- and post-operative evaluations revealed no complications in any of the participants. Both intraoperative procedures and post-operative recovery were uneventful, with no evidence of infection, donor site morbidity, or neurovascular compromise. This consistency across the cohort reinforces the safety profile of the nerve transfer procedures performed. A total of 26 adult patients with irreparable post-traumatic BPIs were evaluated following nerve transfer procedures. Functional recovery was assessed across three key upper-limb outcomes: active shoulder abduction, active elbow flexion, and useful external rotation (Table 3).
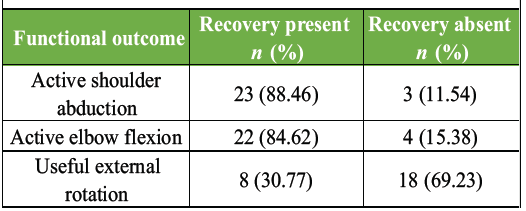
Table 3: Overall functional recovery following nerve transfer surgery (n=26)
Active shoulder abduction was restored in 23 of 26 patients (88.46%). Active elbow flexion recovery was achieved in 22 of 26 patients (84.62%). This outcome was statistically significant in one-sample t-testing (both P < 0.001), confirming the high effectiveness of nerve transfer techniques in restoring shoulder abduction and elbow flexion (Tables 4 and 5).
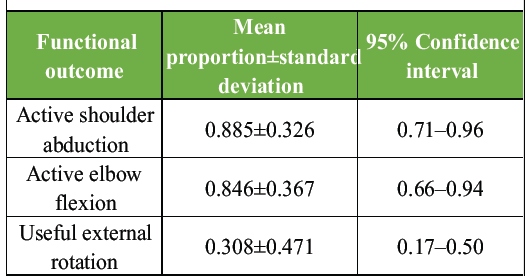
Table 4: Descriptive statistics of functional recovery
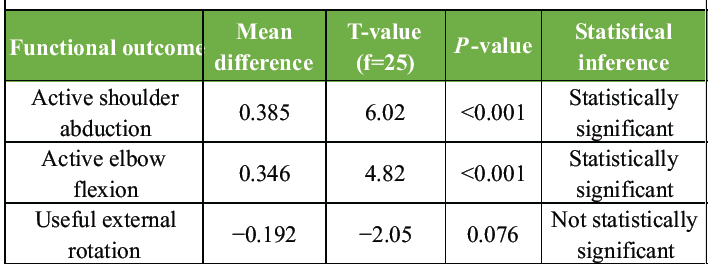
Table 5: One-sample t-test for functional recovery (test value=0.5)
In contrast, useful external rotation was restored in only 8 of 26 patients (30.77%), P = 0.076, demonstrating inconsistent recovery of external rotation following nerve transfer surgery. Importantly, no intra-operative or post-operative complications were reported in this cohort, suggesting that the procedures were not only effective but also safe within the observed population.
Injuries to the upper brachial plexus account for approximately 15–20% of injuries to the supraclavicular plexus [16]. These injuries generally have a favourable prognosis due to the preservation of hand function. However, in cases involving root avulsion, direct nerve repair is not possible. In such situations, nerve transfers are more effective than alternatives such as tendon or muscle transfers or shoulder arthrodesis [17]. Furthermore, in cases where extensive fibrosis affects the upper plexus, the viability of proximal root stumps may be compromised, making nerve transfer the only practical option for arm rehabilitation [18]. The primary objectives of nerve transfers in these cases are to restore elbow flexion and shoulder abduction. The intercostal nerves, medial pectoral nerve, phrenic nerve, thoracodorsal nerve, and SAN are among the donor nerves that have been effectively utilised to produce elbow flexion. Techniques including muscle-tendon transfers, nerve transfers, and arthrodesis can be used to treat shoulder abduction and stability. While shoulder arthrodesis provides stability, it often results in a restricted range of motion. Muscle and tendon transfers, which utilise muscles such as the trapezius, levator scapulae, sternocleidomastoid, or latissimus dorsi, can also be challenging for achieving optimal results. In contrast, nerve transfers have been shown to offer superior outcomes in terms of shoulder abduction and stability [19]. Emamhadi et al. [13] reported an 86% success rate in shoulder abduction using spinal accessory to suprascapular nerve transfer in patients with BPIs. In our study, the success rate for restoring active shoulder abduction was slightly higher at 88.46%. This similarity supports the reliability of SAN transfers in addressing shoulder abduction. However, differences in sample size (9 vs. 26 patients) and follow-up duration (not specified in Emamhadi et al. vs. 24 months in our study) may account for any subtle variations. Bhandari et al. [14] demonstrated an 83% success rate for restoring elbow flexion using the Oberlin nerve transfer technique. Our study observed a comparable outcome, with 84.62% of patients achieving successful elbow flexion restoration. Both studies underscore the efficacy of Oberlin transfers for this function. Chuang et al. [15] reported a 45% success rate in external rotation recovery using spinal accessory to suprascapular nerve transfers. In comparison, our study observed a lower recovery rate of 30.77% for external rotation. The discrepancy may be attributed to differences in rehabilitation protocols, variations in surgical techniques, or patient-specific factors such as injury severity and chronicity. This highlights external rotation recovery as a challenging area requiring further refinement in surgical and post-operative strategies. Midha [16] emphasised the superiority of nerve transfers over alternative approaches such as tendon transfers, particularly in cases of root avulsion or fibrosis. Our study echoes these findings, demonstrating the effectiveness of nerve transfers in achieving meaningful functional recovery in the upper extremity. Both studies affirm that nerve transfers provide better outcomes than other reconstructive techniques, reinforcing their role as the preferred treatment for upper BPIs. Ray et al. [11] reviewed various nerve transfer procedures and highlighted the success of spinal accessory and intercostal nerve transfers in restoring shoulder and elbow functions. Our study similarly demonstrated positive outcomes for shoulder abduction and elbow flexion using these nerve transfer techniques. However, the challenges in external rotation recovery align with Ray et al.’s observations about the variability in outcomes depending on donor and recipient nerve selection. Thatte et al. [7] explored the efficacy of nerve transfer techniques and discussed factors such as donor nerve selection, timing of surgery, and patient-specific variables influencing outcomes. Our study highlights similar conclusions, emphasising the need for further research to optimise donor and recipient nerve pairings and refine timing for interventions. The findings are consistent, indicating that nerve transfer techniques are most effective when tailored to the patient’s specific injury profile. The present findings should be interpreted in the context of several methodological considerations. The retrospective design may introduce selection and information bias inherent to medical record review. Furthermore, the inclusion of different nerve transfer procedures reflects real-world clinical practice but limits direct comparison of the effectiveness of individual techniques. Future prospective studies with larger cohorts and standardised treatment protocols are needed to better define procedure-specific outcomes.
Strengths of the study:
A notable strength of this study is its focus on a well-defined cohort of patients with irreparable upper root injuries, ensuring the applicability of findings to similar clinical scenarios. The use of standardised evaluation metrics, such as the BMRC grading system, enhances the reliability of the results. In addition, the study’s rigorous follow-up period of 24 months provides meaningful insights into the intermediate-term outcomes of nerve transfers.
Limitations of study:
This study has several limitations. The relatively small sample size (n = 26), retrospective design, and single-centre setting limit the generalisability of the findings and may introduce selection and information bias. The inclusion of multiple nerve transfer techniques within the same cohort created procedural heterogeneity, making procedure-specific outcome comparisons difficult. In addition, the absence of a control group prevented direct comparison with alternative reconstructive strategies. Although the mean follow-up period was 24 months, longer follow-up is required to evaluate the durability of recovery and late complications. Functional assessment was primarily based on shoulder abduction, external rotation, and elbow flexion using the BMRC grading system; therefore, sensory recovery, hand function, pain relief, quality of life, patient-reported outcomes, and return-to-work status were not evaluated. Variability in patient compliance with rehabilitation protocols was also not independently analysed. Furthermore, only patients with upper root injuries treated within 10 months of injury were included, limiting applicability to delayed presentations and more extensive BPIs. Future prospective multicentre studies with larger cohorts are needed to validate these findings.
Future directions:
Building on these findings, future research should aim to address the limitations of this study. Multi-centre trials with larger sample sizes and standardised surgical protocols could provide more robust data. In addition, studies exploring patient-specific factors, such as age, injury chronicity, and co-morbidity, could help refine patient selection criteria and predict outcomes more accurately. The role of tailored rehabilitation programmes in optimising functional recovery also warrants further investigation. Finally, advancements in nerve transfer techniques, including the use of biological or synthetic conduits to enhance nerve regeneration, hold promise for improving outcomes, particularly for challenging functions like external rotation.
Nerve transfers offer a promising surgical approach for managing BPIs, demonstrating notable functional recovery in upper extremity movements.
The findings provide strong statistical evidence that nerve transfer procedures are highly effective in restoring shoulder abduction and elbow flexion in adults with irreparable BPIs. However, recovery of external rotation was significantly lower and did not reach statistical significance, confirming that this functional domain remains inconsistent and less reliably restored. While recovery can be inconsistent in some areas, overall outcomes are encouraging. Further research is needed to improve success rates and identify factors influencing functional outcomes. Investigating different techniques, patient-specific variables, optimal surgery timing, and tailored rehabilitation programmes could enhance recovery. Long-term efficacy and sustainability of these results are crucial to evaluate, enabling better-informed treatment decisions. Nerve transfers provide valuable hope for improved outcomes in patients with this challenging condition.
In patients with irreparable upper brachial plexus injuries, nerve transfers can reliably restore key upper limb functions, particularly elbow flexion and shoulder abduction. Timely intervention within the 1st year after injury significantly improves outcomes. Recovery of external rotation remains challenging and should be discussed during pre-operative patient counselling.
References
- 1. Mancuso CA, Lee SK, Dy CJ, Landers ZA, Model Z, Wolfe SW. Expectations and limitations due to brachial plexus injury: A qualitative study. Hand (N Y) 2015;10:741-9. [Google Scholar] [PubMed]
- 2. Bayot ML, Nassereddin A, Varacallo M. Anatomy, shoulder and upper limb, brachial plexus. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2024. [Google Scholar] [PubMed]
- 3. Kaiser R, Waldauf P, Ullas G, Krajcová A. Epidemiology, etiology, and types of severe adult brachial plexus injuries requiring surgical repair: Systematic review and meta-analysis. Neurosurg Rev 2020;43:443-52. [Google Scholar] [PubMed]
- 4. Jeevannavar JS, Appannavar S, Kulkarni S. Obstetric brachial plexus palsy-a retrospective data analysis. Indian J Physiother Occup Ther 2020;14:25-9. [Google Scholar] [PubMed]
- 5. Ferrante MA. Brachial plexopathies: Classification, causes, and consequences. Muscle Nerve 2004;30:547-68. [Google Scholar] [PubMed]
- 6. Nagano A. Treatment of brachial plexus injury. J Orthop Sci 1998;3:71-80. [Google Scholar] [PubMed]
- 7. Thatte MR, Babhulkar S, Hiremath A. Brachial plexus injury in adults: Diagnosis and surgical treatment strategies. Ann Indian Acad Neurol 2013;16:26-33. [Google Scholar] [PubMed]
- 8. Warwick D, Srinivasan H, Solomon L. Peripheral nerve disorders. In: Solomon L, Warwick D, Nayagam S, editors. Apley’s System of Orthopaedics and Fractures. 9th ed. London: Hodder Arnold; 2010. p. 269-86. [Google Scholar] [PubMed]
- 9. Codsi M, McCarron J, Brems JJ. Clinical evaluation of the shoulder problems. Clin Orthop Relat Res 2009;467:145-76. [Google Scholar] [PubMed]
- 10. Connolly BA, Jones GD, Curtis AA, Murphy PB, Douiri A, Hopkinson NS, et al. Clinical predictive value of manual muscle strength testing during critical illness: An observational cohort study. Crit Care 2013;17:R229. [Google Scholar] [PubMed]
- 11. Ray WZ, Chang J, Hawasli AH, Wilson TJ, Yang L. Motor nerve transfers: A comprehensive review. Neurosurgery 2016;78:1-26. [Google Scholar] [PubMed]
- 12. Addas BM, Midha R. Nerve transfers for severe nerve injury. Neurosurg Clin N Am 2009;20:27-38. [Google Scholar] [PubMed]
- 13. Emamhadi M, Alijani B, Andalib S. Long-term clinical outcomes of spinal accessory nerve transfer to the suprascapular nerve in patients with brachial plexus palsy. Acta Neurochir (Wien) 2016;158:1801-6. [Google Scholar] [PubMed]
- 14. Bhandari PS, Sadhotra LP, Bhargava P, Bath AS, Mukherjee MK, Bhatti T, et al. Surgical outcomes following nerve transfers in upper brachial plexus injuries. Indian J Plast Surg 2009;42:150-60. [Google Scholar] [PubMed]
- 15. Chuang DC, Yeh MC, Wei FC. Intercostal nerve transfer of the musculocutaneous nerve in avulsed brachial plexus injuries: Evaluation of 66 patients. J Hand Surg Am 1992;17:822-8. [Google Scholar] [PubMed]
- 16. Midha R. Epidemiology of brachial plexus injuries in a multitrauma population. Neurosurgery 1997;40:1182-8; discussion 1188-9. [Google Scholar] [PubMed]
- 17. Kostas-Agnantis I, Korompilias A, Vekris M, Lykissas M, Gkiatas I, Mitsionis G, et al. Shoulder abduction and external rotation restoration with nerve transfer. Injury 2013;44:299-304. [Google Scholar] [PubMed]
- 18. Bahm J. Surgical Rationales in Functional Reconstructive Surgery of the Upper Extremity. Cham: Springer Nature; 2023. [Google Scholar] [PubMed]
- 19. Saha AK. Surgery of the paralysed and flail shoulder. Acta Orthop Scand 1967;38:3-90. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 November 1, 2024 Hydropneumothorax in an Isolated Midshaft Clavicle Fracture
November 1, 2024 Hydropneumothorax in an Isolated Midshaft Clavicle Fracture February 10, 2022 Fibrocartilaginous Dysplasia – A Report of Five Cases with Review of Literature
February 10, 2022 Fibrocartilaginous Dysplasia – A Report of Five Cases with Review of Literature June 10, 2024 Comprehensive Evaluation and Arthroscopic Management of Circumferential Labral Tears Following Traumatic First Time Shoulder Dislocation: A Case Report and Review
June 10, 2024 Comprehensive Evaluation and Arthroscopic Management of Circumferential Labral Tears Following Traumatic First Time Shoulder Dislocation: A Case Report and Review July 10, 2020 Ulnar Nerve and Ulnar Artery Injury Caused by Comminuted Distal Radius Fracture
July 10, 2020 Ulnar Nerve and Ulnar Artery Injury Caused by Comminuted Distal Radius Fracture