
Intra-articular injection of Growth Factor Concentrate (GFC) is a safe and effective disease-modifying therapy for Kellgren–Lawrence Grade II and III knee osteoarthritis, providing sustained pain relief, functional improvement, and structural preservation compared to normal saline.
Dr Amit Saraf, Department of Orthopaedics, Teerthanker Mahaveer Medical College and Research Centre, Moradabad, Uttar Pradesh, India. E-mail: amitsaraf_75@yahoo.com
Abstract
Introduction: Knee osteoarthritis (KOA) is a leading global cause of pain and functional impairment, with a high prevalence in India driven by ageing and obesity. Traditional treatments often provide only symptomatic relief without addressing underlying structural degeneration. This study evaluates the efficacy of intra-articular growth factor concentrate (GFC) as a regenerative and disease-modifying therapy for moderate KOA.
Materials and Methods: In this randomized controlled trial, 72 patients with Kellgren-Lawrence (KL) Grade II or III KOA were randomized into two groups. Group A (n = 36) received two ultrasound-guided intra-articular injections of autologous GFC spaced four weeks apart, while Group B (n = 36) received normal saline. Clinical outcomes were assessed using the Visual Analogue Scale (VAS) and the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC). Structural and biochemical changes were monitored via magnetic resonance imaging (MRI) (Whole-Organ Magnetic Resonance Imaging Score) and serum Coll2-1NO2 levels at baseline, 6 months, and 9 months.
Results: A total of 66 patients completed the 9-month follow-up. Group A demonstrated a significant reduction in mean VAS scores (6.48–2.79; P < 0.0001) and WOMAC scores (62.58–47.40; P < 0.0001), indicating superior pain relief and functional improvement compared to Group B, which showed mild worsening. Biochemically, Group A showed a significant decrease in serum Coll2-1 levels (P = 0.03), suggesting reduced cartilage breakdown. MRI analysis revealed increased WORM scores in Group A (130.03–136.91; P = 0.03), indicating cartilage preservation and potential regeneration, whereas Group B scores decreased (P = 0.027).
Conclusion: Intra-articular GFC injection is a safe and effective intervention for KL Grade II and III KOA. It provides sustained symptomatic relief and demonstrates potential disease-modifying effects through cartilage preservation and reduced degradation biomarkers. GFC represents a viable biological therapy to bridge the gap between conservative management and invasive surgical procedures.
Keywords: Knee osteoarthritis, growth factor concentrate, regenerative medicine, cartilage regeneration, growth factor concentrate, visual analog scale, WOMAC.
Knee osteoarthritis (KOA) is a chronic, progressive degenerative disorder and a leading global cause of pain, disability, and functional impairment. Characterised by the breakdown of hyaline cartilage, subchondral bone remodelling, and synovial inflammation, KOA is now recognised as a complex disease involving the entire joint organ. [1-4] In 2023, approximately 528 million people worldwide were living with osteoarthritis (OA), representing a 113% increase since 1990. In India, the prevalence is particularly high, ranging from 22% to 39%, driven by ageing populations, obesity, and culturally specific physical postures. [5] Current management strategies include non-pharmacological interventions, analgesics, and intra-articular injections of corticosteroids or hyaluronic acid (HA). However, these treatments primarily provide symptomatic relief and fail to address the underlying structural degeneration. While total knee replacement (TKR) is definitive for advanced stages, its high costs and surgical risks have spurred interest in biological and regenerative therapies for early-to-moderate KOA. [6-8] Growth factor concentrate (GFC), derived from autologous platelets, has emerged as a promising regenerative approach. [9] GFC contains biologically active molecules such as platelet-derived growth factor (PDGF), transforming growth factor-beta (TGF-β), and insulin-like growth factor-1 (IGF-1) that modulate inflammation and promote cartilage repair and extracellular matrix synthesis. [9,10] Despite encouraging preliminary data, there is a lack of high-quality evidence regarding the long-term efficacy and disease-modifying potential of GFC, particularly in Kellgren-Lawrence (KL) Grade II and III patients. [11-13] This study aims to evaluate the effect of intra-articular GFC injections on pain reduction, functional outcomes, and disease progression in patients with moderate KOA, utilising clinical scores (Visual Analogue Scale [VAS] and Western Ontario and McMaster Universities Osteoarthritis Index [WOMAC]), biochemical markers (serum Coll2-1NO₂), and advanced imaging (Whole-Organ Magnetic Resonance Imaging Score [WORMS]-based magnetic resonance imaging [MRI]). [14]
Study design and setting:
This study is a single-centre, hospital-based randomised controlled trial. The research was conducted in the Department of Orthopaedics at Teerthanker Mahaveer Medical College and Research Centre following approval from the College Research Committee and the Institutional Ethics Committee (TMU/IEC/2024-25/PG/122) (Date of Approval – June 07, 2024).
Participant selection:
Adult patients (>18 years) presenting to the orthopaedic outpatient department were screened. Inclusion was based on the American College of Rheumatology 2019 criteria and a diagnosis of KL Grade II or III OA through standing radiographs. Key exclusion criteria included the following:
- Inflammatory or secondary OA and active knee infections
- Bleeding disorders, uncontrolled diabetes, or known malignancy
- MRI contraindications or ligamentous instability
- History of previous intra-articular steroid injections.
Randomisation and intervention:
A total of 72 participants (36 per group, accounting for a 20% loss to follow-up) were randomised using computer-generated software.
- Group A (Case): Received two intra-articular injections of GFC spaced 4 weeks apart
- Group B (Control): Received two intra-articular injections of normal saline (NS) on the same schedule.
Methodology:
After obtaining approval from the College Research Committee (CRC) and the Institutional Ethics Committee (IEC), patients will be recruited from the outpatient department (OPD) based on radiological confirmation of knee osteoarthritis classified by ACR criteria with Kellgren–Lawrence grades II and III on standing anteroposterior and lateral knee radiographs. All participants will be screened according to predefined inclusion and exclusion criteria, and eligible subjects will be randomised into two groups. Randomisation will be performed using a computer-generated random sequence, and patients will be allocated into Group A (GFC) and Group B (normal saline control). The baseline assessment will include recording of the Visual Analogue Scale (VAS), the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), serum Coll2-1NO₂ levels, radiographic evaluation, and MRI assessment using the WORMS scoring system prior to the first intra-articular injection. Patients will then receive the first ultrasound-guided intra-articular injection according to group allocation (GFC or normal saline). At 1-month follow-up, VAS and WOMAC scores will be reassessed, and a second ultrasound-guided intra-articular injection will be administered. At 6 months, VAS and WOMAC scores will again be recorded to evaluate clinical improvement. At 9 months, the final assessment will include VAS, WOMAC, serum Coll2-1NO₂ levels, radiographs, and MRI evaluation using WORMS scoring to determine the overall effect of the intervention.
Preparation and administration:
GFC was prepared by collecting 8 mL of autologous blood in a specialised vacutainer, followed by 30 min of activation and centrifugation at 3400 rpm for 10 min to separate the yellowish GFC layer. Both GFC and NS were administered via ultrasound-guided injection into the suprapatellar pouch using a 22-G needle under sterile conditions.
Outcome measures:
Clinical and structural assessments were performed at baseline, 6 months, and 9 months.
- Clinical Scores: VAS for pain and WOMAC for function
- Biochemical Analysis: Serum Coll2-1NO2 levels to monitor cartilage degradation
- Imaging: X-rays and MRI scored using the WORMS to evaluate structural changes.
Statistical analysis:
Data analysis was conducted using the Statistical Package for the Social Sciences version 20. Categorical variables were assessed via Pearson’s chi-square test, while continuous variables were compared using the Z-test. Significance was set at P < 0.05.
Demographic and baseline characteristics:
A total of 66 patients completed the study, divided equally into Group A (GFC, n = 33) and Group B (NS, n = 33). The mean age was 55.54 ± 12.00 years in Group A and 52.00 ± 10.68 years in Group B, with no statistically significant difference between the groups (P = 0.21). Gender distribution showed a significant difference (P = 0.002), with females constituting 75.76% of Group A compared to 39.39% in Group B. The groups were well-matched regarding comorbidities (P = 0.15), with hypertension being the most common medical condition in Group A (36.36%), and Group B patients frequently presenting with no comorbidities (48.48%).
Radiographic and clinical parameters:
- KL Grade: Distribution was comparable between groups (P = 0.51). In Group A, 51.52% had Grade III OA, while 48.48% of Group B had Grade II
- Side Involvement: Group A primarily exhibited Right-sided involvement (51.52%), whereas Group B showed a high prevalence of Bilateral involvement (66.67%) (P < 0.0001)
- Baseline Labs: Haemoglobin and random blood sugar were similar across groups. While Total Leukocyte Count was higher in Group A (P = 0.0009), it did not impact baseline clinical status.
Primary clinical outcomes: VAS and WOM AC scores:
Pain and functional scores diverged significantly over the 9-month period:
- VAS: Group A reported a significant and sustained reduction in pain, with mean scores decreasing from 6.48 ± 1.00 at baseline to 2.79 ± 1.10 at 9 months (P < 0.0001). Conversely, Group B scores increased from 5.54 ± 1.25 to 6.03 ± 1.07, indicating a mild worsening of pain (Table 1 and Fig. 1)
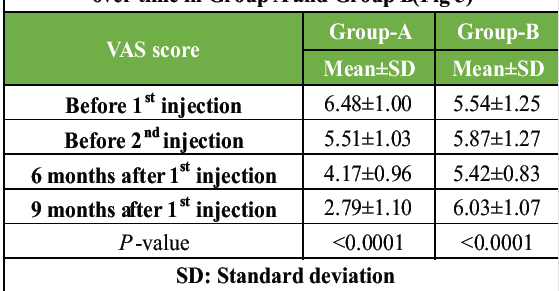
Table 1: Changes in Visual Analogue Scale (VAS) scores over time in Group A and Group B (Fig 5)

Figure 1: Step 1 of preparation of GFC
- WOMAC Score: Functional outcomes in Group A improved significantly, with mean scores falling from 62.58 ± 10.88 to 47.40 ± 11.09 (P < 0.0001). In Group B, functional impairment increased, with scores rising from 51.48 ± 10.56 to 59.99 ± 7.61 (P = 0.0001) (Table 2 and Fig. 2).
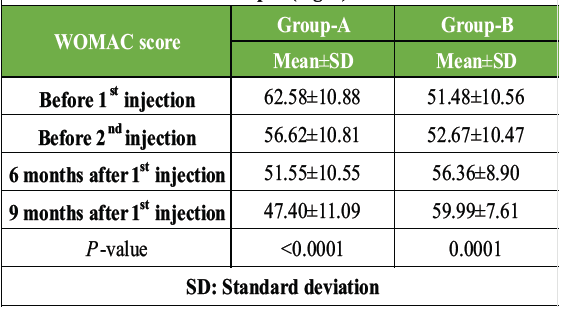
Table 2: Changes in WOMAC scores over time in Group A and Group B (Fig. 6)
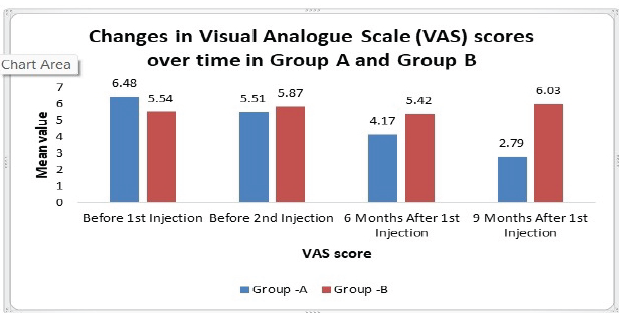
Figure 6: Changes in WOMAC score over time in Group A and Group B
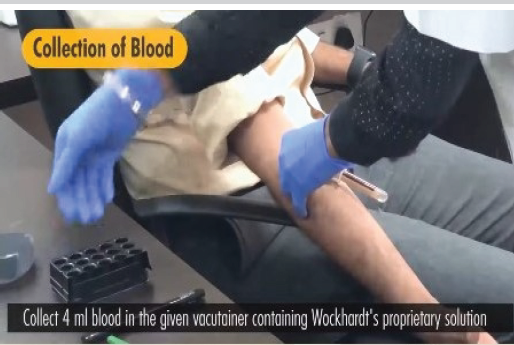
Figure 2: Step 2 of preparation of GFC
Structural and biochemical outcomes:
- Serum COLL 2-1: Group A demonstrated a significant reduction in mean collagen Type II levels from 34.40 ± 36.62 to 18.75 ± 22.22 (P = 0.03), suggesting decreased cartilage breakdown. Group B showed no such improvement (Table 3 and Fig. 3)
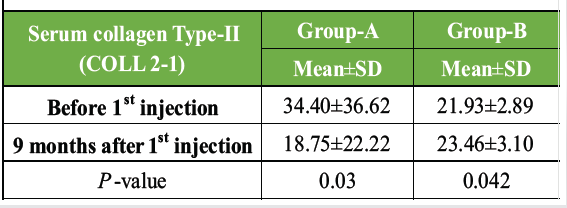
Table 3: Changes in serum collagen Type II (COLL 2-1) levels over time in Group A and B (Fig. 7)
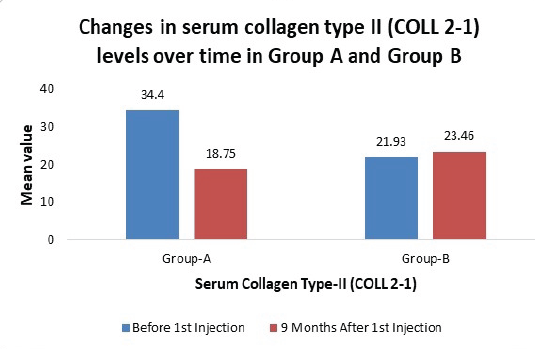
Figure 7: Changes in Serum Collagen type 2 level over time in Group A and Group B

Figure 3: Step 3 of preparation of GFC
- MRI (WORM Score): In Group A, the mean WORM score increased from 130.03 ± 12.74 to 136.91 ± 13.35 (P = 0.03), indicating preservation of cartilage thickness and potential regeneration. Group B scores decreased from 128.82 ± 10.22 to 123.63 ± 9.89 (P = 0.027), reflecting ongoing cartilage loss (Table 4 and Fig. 4)
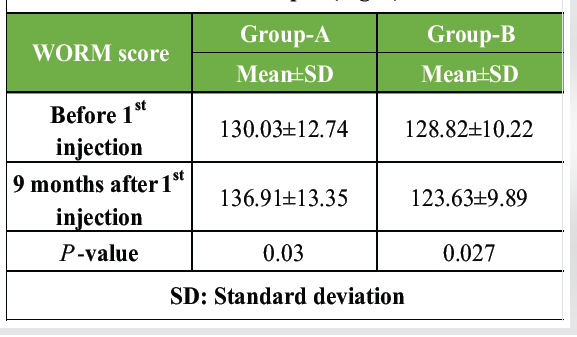
Table 4: Changes in WORM scores over time in Group A and Group B (Fig. 8)
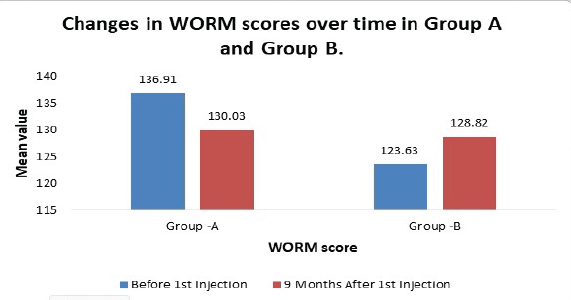
Figure 8: Changes in WORM score over time in Group A and Group B
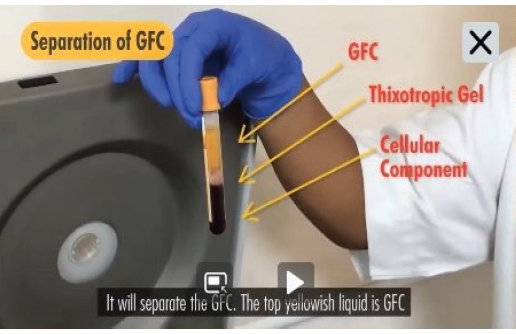
Figure 4: Step 4 of preparation of GFC
- Growth Factor Concentrations: Comparisons of growth factor levels (PDGF, vascular endothelial growth factor, fibroblast growth factor, IGF-1, TGF-β) between the groups at the time of assessment showed no statistically significant differences (P > 0.05 for all), indicating comparable baseline biochemical profiles (Fig. 5).
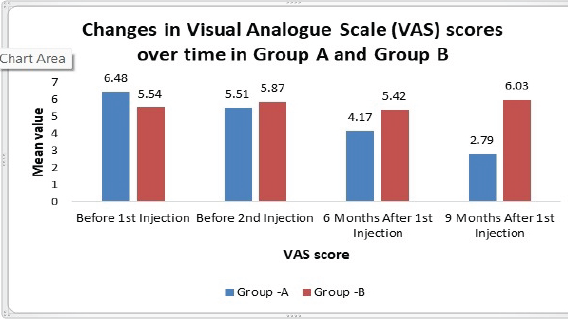
Figure 5: Changes in VAS score over time in Group A and Group B
The clinical management of KOA is evolving from purely symptomatic relief toward regenerative strategies that aim to alter the disease’s natural history. This study evaluated the therapeutic efficacy of intra-articular GFC in patients with KL Grade II and III KOA. Our findings demonstrate that GFC provides superior outcomes in pain reduction, functional improvement, and structural preservation compared to NS.
Comparative analysis of clinical outcomes:
Pain and function:
The most striking result was the divergent paths of the two groups regarding pain and physical function. Group A (GFC) experienced a sustained and statistically significant reduction in VAS scores, dropping from 6.48 to 2.79 over 9 months. In contrast, Group B (NS) showed a slight increase in pain levels. This improvement in GFC-treated patients was mirrored in WOMAC scores, which showed progressive enhancement in mobility and stiffness. These results align with previous studies, such as those by Ozcan et al. (2024) and Saraf et al. (2023), which reported that growth factor-derived therapies offer superior symptomatic relief compared to traditional viscosupplementation or placebos.
- Comparison with Saraf et al. (2023): Our findings align with Saraf et al., who reported meaningful improvements in pain and function following three monthly GFC injections that persisted for 12 months
- Comparison with Ozcan et al. (2024): Our study supports the conclusion that growth factor-based therapies (like CGF or GFC) provide superior functional improvement compared to traditional HA or standard platelet-rich plasma (PRP).
- Comparison with Hong et al. (2021): Our longitudinal data mirrors their meta-analysis findings, which demonstrated that PRP-derived treatments outperform both placebo and HA in long-term functional recovery.
Biochemical markers (Serum COLL 2-1):
A key challenge in OA management is altering the disease’s natural progression. In this study, the GFC group showed a significant reduction in serum COLL 2-1 levels. As COLL 2-1 is a biomarker for cartilage degradation, this reduction suggests that GFC may exert a chondroprotective effect. This biochemical trend validates the observations by Saraf et al. (2023), who also noted that GFC therapy significantly reduced Coll2-1 levels, suggesting a protective effect on cartilage integrity.
Structural preservation and regeneration (WORMS):
While many studies focus purely on subjective scores, our use of specialised MRI sequences (WORMS) provided objective evidence of structural impact. Structural outcomes measured through MRI (WORM scores) further support this biological rationale. While the saline group showed a decrease in scores (indicating continued cartilage loss), the GFC group showed an increase. This suggests not only the preservation of existing cartilage thickness but also hints at potential cartilage regeneration and a decrease in synovial thickening.
- Contrast with Natural Progression: In contrast, the control group (NS) experienced a significant decrease in WORM scores, reflecting the natural degenerative course of KOA
- Mechanism Support: These findings are biologically supported by the work of Riewruja et al. (2022), who stated that high levels of growth factors like PDGF and TGF-\beta (both present in our GFC profile) enhance chondrocyte proliferation by activating genes such as COL2A1 and ACAN. The therapeutic success of GFC is likely attributed to the high concentration of biologically active molecules such as PDGF, TGF-β, and IGF-1. These factors are known to stimulate cellular proliferation, enhance Type II collagen synthesis, and inhibit the catabolic pathways responsible for cartilage breakdown.
Demographic and baseline considerations:
The gender distribution in our study (75.76% female in Group A) reflects global and national epidemiological trends where women account for approximately 60% of the disease burden and are more frequently affected after age 50. Despite a significant difference in baseline leukocyte counts (P = 0.0009), this did not influence the clinical status or the eventual therapeutic superiority of GFC. This suggests that the biological enrichment of growth factors (PDGF, IGF-1, and TGF-\beta) is the primary driver of the clinical benefits, rather than baseline systemic laboratory variations.
Key takeaway:
The significant reduction in pain and the biochemical/radiological evidence of cartilage preservation suggest that GFC acts as a disease-modifying agent rather than just a palliative treatment.
Limitations
While the results are promising, several limitations should be acknowledged:
- Short Follow-up Duration: An 18-month total study period with a 9-month comprehensive follow-up provides insight into mid-term efficacy, but longer-term studies (2–5 years) are needed to determine the longevity of the regenerative effects and thoroughly characterize the long-term safety profile of repeated intra-articular GFC administrations
- Gender Imbalance: Group A had a significantly higher proportion of female participants (75.76%) compared to Group B (39.39%), introducing selection bias that may limit the external generalizability of these comparative outcomes across balanced cohorts
- Bilateral Involvement: A significant portion of Group B had bilateral knee involvement (66.67%) compared to Group A (9.09%), potentially affecting baseline functional (WOMAC) scores and perceived pain levels
- Sample Size and Design: While sufficient for statistical significance in this trial, the single-center nature and relatively small final sample size (n= 66) restrict its external validity and statistical power to detect smaller localized treatment effects or uncover rare adverse occurrences
- Lack of Active Comparator and Blinding: The implementation of a NS control instead of active standard treatments (like PRP, HA, or steroids) limits direct conclusions regarding relative therapeutic superiority. Furthermore, the open-label design introduces a risk of performance and subjective evaluation biases
- Restricted Disease Spectrum: Eligibility was confined solely to KL Grade II and III OA; hence, the data cannot be extrapolated to early Grade I or late-stage Grade IV joint disease
- Unquantified Dose-Response and Restricted Biomarkers: Individual growth factor concentrations within each autologous injection were not quantified or statistically correlated with treatment clinical success, obscuring potential dose-response profiles. In addition, metabolic biochemical assessment was limited exclusively to serum Coll2-1NO2, lacking a comprehensive panel of overlapping inflammatory and catabolic joint markers.</mark>
- Imaging Restrictions: Joint structural profiling was confined to semi-quantitative WORMS-based MRI scoring. Advanced quantitative imaging methodologies, such as T2 mapping, dGEMRIC, or cartilage volume analysis, were not implemented
- Confounding Lifestyle Factors and Cost-Effectiveness: Dynamic lifestyle confounders – including body mass index, physical activity levels, occupational parameters, post-injection physiotherapy compliance, and dietary variables—were neither standardized nor statistically controlled. Finally, no economic or cost-effectiveness feasibility analysis was conducted to support real-world clinical translation.
The present study demonstrates that intra-articular injection of GFC is a highly effective and safe intervention for patients with KL Grade II and III KOA. Unlike conventional treatments that offer only transient symptomatic relief, GFC targets the underlying pathophysiological mechanisms of the disease. Over a 9-month follow-up period, patients treated with GFC showed:
- Significant Pain Reduction: Mean VAS scores improved from 6.48 to 2.79, indicating superior and sustained pain relief compared to the control group
- Functional Restoration: WOMAC scores showed a consistent decline, reflecting marked improvements in physical mobility and a reduction in joint stiffness
- Disease Modification: A significant reduction in serum COLL 2-1 levels suggests a decrease in active cartilage breakdown
- Structural Preservation: MRI evaluations using WORMS indicated not only the preservation of cartilage thickness but also signs of potential cartilage regeneration and decreased synovial thickening.
Autologous GFC represents a promising regenerative and disease-modifying therapy that can significantly improve the quality of life for KOA patients while potentially delaying the need for surgical interventions like TKR. Our study reinforces the growing consensus that GFC is a safe and effective “point-of-care” biological therapy for moderate KOA. It effectively bridges the gap between conservative pharmacological management and invasive surgical interventions like TKR.
- Regenerative Potential: Intra-articular injection of GFC significantly outperforms NS in providing sustained pain relief and functional improvement for patients with KL Grade II and III KOA
- Disease Modification: Unlike purely symptomatic treatments, GFC demonstrates potential disease-modifying effects by significantly reducing cartilage degradation biomarkers such as serum COLL2-1.
- Structural Preservation: MRI evidence (WORM scores) suggests that GFC therapy may not only preserve existing joint structures but could facilitate a degree of cartilage regeneration and reduction in synovial thickening
- Safety and Feasibility: The procedure is safe, well-tolerated, and can be effectively performed under ultrasound guidance in an outpatient setting, making it a viable alternative for patients seeking to delay or avoid surgical intervention
- Target Population: GFC is particularly beneficial for patients in early-to-moderate stages of OA (KL grades II and III), where biological restoration of joint homeostasis is still achievable.
References
- 1. Altman RD. Classification of disease: Osteoarthritis. Semin Arthritis Rheum. 1991;20(6 Suppl 2):40–47. [Google Scholar] [PubMed]
- 2. Belluzzi E, El Hadi H, Granzotto M, Rossato M, Ramonda R, Macchi V, et al. The infrapatellar fat pad as a source of inflammatory mediators in knee osteoarthritis. Cells. 2019;8(8):875. [Google Scholar] [PubMed]
- 3. Houard X, Goldring MB, Berenbaum F, Sellam J, Berenbaum F, Henrotin Y, et al. The role of cartilage-bone crosstalk in osteoarthritis. Curr Opin Rheumatol. 2013;25(5):539–546. [Google Scholar] [PubMed]
- 4. Suri S, Walsh DA, Conaghan PG, Berenbaum F, Henrotin Y, McWilliams DF, et al. The role of subchondral bone and its vascularization in osteoarthritis pain. Ann N Y Acad Sci. 2012;1254:163–171. [Google Scholar] [PubMed]
- 5. Singh S, Sharma A, Kumar A, Gupta V, Jain M, Singh R, et al. Prevalence and burden of osteoarthritis in India: A systematic review and meta-analysis. Indian J Orthop. 2022;56:1234–1245. [Google Scholar] [PubMed]
- 6. Louis ML, Magalon J, Jouve E, Bornet CE, Mattei JC, Chagnaud C, et al. Single injection of platelet-rich plasma (PRP) for knee osteoarthritis: A comparative study with hyaluronic acid. Arthroscopy. 2018;34(12):3398–3410. [Google Scholar] [PubMed]
- 7. Raeissadat SA, Rayegani SM, Hassanabadi H, Fathi M, Ghorbani E, Babaee M, et al. Evaluation of platelet-rich growth factor (PRGF) in comparison with hyaluronic acid in knee osteoarthritis. J Clin Med. 2020;9(6):1200. [Google Scholar] [PubMed]
- 8. Raeissadat SA, Rayegani SM, Babaee M, Ghorbani E, Rahimi-Dehgolan S, Bahrami MH, et al. Safety and efficacy of ozone, hyaluronic acid, and platelet-rich plasma in knee osteoarthritis. Int J Rheum Dis. 2021;24(2):139–148. [Google Scholar] [PubMed]
- 9. Anitua E, Sánchez M, Orive G, Andía I, Padilla S, Mujika I, et al. New insights into and novel applications for platelet-rich plasma therapy in traumatology and sports medicine. Vaccines (Basel). 2014;2(4):617–634. [Google Scholar] [PubMed]
- 10. Riewruja K, Chokboonmongkol C, Chaiyawat P, Chotanaphuti T, Sumanont S, Soparat C, et al. Growth factor levels in platelet-rich plasma and their impact on chondrocyte proliferation. Biomedicines. 2022;10(6):1452. [Google Scholar] [PubMed]
- 11. Gupta A, Maffulli N, Malempati CS, Ramasamy A, et al. Efficacy and safety of growth factor concentrate in knee osteoarthritis: A systematic review. J Orthop. 2024;45:100–110. [Google Scholar] [PubMed]
- 12. Ozcan S, Kaya A, Yildiz C, Demir B, Aydin H, Korkmaz M, et al. Comparative efficacy of intra-articular hyaluronic acid, platelet-rich plasma, and concentrated growth factor in knee osteoarthritis: A randomized controlled trial. 2024; (journal details incomplete). [Google Scholar] [PubMed]
- 13. Saraf A, Kumar R, Singh V, Patel M, Desai K, Shah P, et al. Intra-articular growth factor concentrate (GFC) for knee osteoarthritis: A randomized controlled trial. J Clin Orthop Trauma. 2023;40:101–108. [Google Scholar] [PubMed]
- 14. Kellgren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis. 1957;16(4):494–502. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
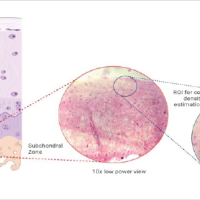 February 1, 2025 Subchondral Cellular Density Decreases with Increasing Grade of Cartilage Degeneration in Knee Osteoarthritis – An Ex vivo Histopathological Analysis
February 1, 2025 Subchondral Cellular Density Decreases with Increasing Grade of Cartilage Degeneration in Knee Osteoarthritis – An Ex vivo Histopathological Analysis August 1, 2026 The Effect of Intraarticular Platelet-Rich Plasma Injection in Knee Osteoarthritis
August 1, 2026 The Effect of Intraarticular Platelet-Rich Plasma Injection in Knee Osteoarthritis August 1, 2026 Comparative Efficacy of Intra-Articular Growth Factor Concentrate and Platelet-Rich Plasma Injections in Knee Osteoarthritis: An Evaluation of Clinical, Radiological, and Biomarker Outcomes
August 1, 2026 Comparative Efficacy of Intra-Articular Growth Factor Concentrate and Platelet-Rich Plasma Injections in Knee Osteoarthritis: An Evaluation of Clinical, Radiological, and Biomarker Outcomes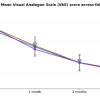 August 1, 2026 Outcome Analysis of Leukocyte-Rich Platelet-Rich Plasma, Leukocyte-Poor Platelet-Rich Plasma, and Injectable Platelet-Rich Fibrin in the Management of Chronic Plantar Fasciitis: A Prospective Comparative Study
August 1, 2026 Outcome Analysis of Leukocyte-Rich Platelet-Rich Plasma, Leukocyte-Poor Platelet-Rich Plasma, and Injectable Platelet-Rich Fibrin in the Management of Chronic Plantar Fasciitis: A Prospective Comparative Study