
Dr. Ankit Tripathi, Department of Orthopaedics, Baba Raghav Das Medical College, Gorakhpur - 273013, Uttar Pradesh, India. E-mail: ankit.aki02@gmail.com
Dear Editor-in-Chief,
We sincerely thank the author for their thoughtful insights on our article titled “Clavicle Fracture Non-Union in a 3-Year-Old Child: A Case Report and Literature Review” published in the Journal of Orthopaedic Case Reports 2026 March;16(03):179–183. We appreciate the constructive comments and the opportunity to further discuss this uncommon clinical entity.
We agree with the author that clavicle fracture non-union in the pediatric age group is exceedingly rare, particularly in children as young as three years of age. As highlighted in our case report that most of the clavicle fractures in pediatric age group unites uneventfully owing to their rich blood supply and remarkable healing and remodelling potential. However, significant fracture displacement with lack of cortical apposition may still predispose to non-union even in very young child with clavicle fracture cases.
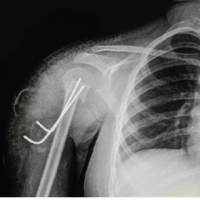
The author also rightly pointed the concerns regarding differentiation from congenital pseudoarthrosis and other associated conditions such as cleidocranial dysplasia and neurofibromatosis. In our patient, several clinical and radiological features favored a traumatic hypertrophic non-union rather than congenital pseudoarthrosis, cleidocranial dysplasia, or neurofibromatosis-related clavicular pathology. The child had a definite history of trauma followed by persistent deformity over clavicle and functional limitation at the same side with parents reporting persistent pain. Radiographs showed clavicle fracture with hypertrophic fracture ends with sclerotic margins and displacement rather than the classical appearance of congenital pseudoarthrosis which classically presents as a painless, smooth-edged pseudoarthrosis involving the middle third of the right clavicle without preceding trauma. Intraoperatively, hypertrophic fracture ends with sclerotic callus were identified along with interposing fibrous tissue, finding more favouring of traumatic non-union. Furthermore, the patient neither had any neurocutaneous manifestations, osseous dysplasia and other features Neurofibromatosis nor had clinical features suggestive of cleidocranial dysplasia such as bilateral clavicular involvement, dental abnormalities, or generalized skeletal dysplasia. The histopathological evaluation done showed no evidence of any congenital clavicular pathology. Nevertheless, we acknowledge that a more elaborate discussion regarding these differential diagnoses could have further strengthened the manuscript.
We also agree with author’s point regarding challenges in symptom interpretation in very young children and parental observations are often more reliable indicator. In our case, the parents consistently reported persistent pain in shoulder, and it was observed by parents to be more associated with overhead activities, parents also noticed visible deformity and functional limitation of the shoulder since the initial injury, which correlated with the clinical and radiological findings at presentation.
The author’s observation regarding the concise nature of the literature review is well taken. Due to the rarity of this condition and limitations of manuscript length, we focused primarily on the most relevant previously reported pediatric clavicle non-union cases. However, we agree that a more detailed comparison with previously published cases could provide additional perspective regarding age distribution, fracture characteristics, management strategies, and outcomes.
We also concur with the author’s point that the absence of standardized radiological follow-up protocols for pediatric clavicle fractures may contribute to delayed recognition of rare complications such as non-union. Our case reinforces the importance of fracture specific management and a careful clinical follow-up in markedly displaced fractures, even in very young children who are otherwise expected to heal reliably with conservative treatment.
We once again thank the author for their thoughtful observation and for contributing meaningfully to the discussion regarding this rare pediatric complication.
Sincerely,
Dr. Rajnand Kumar1, Dr. Ankit Tripathi2, Dr. Nitish Kumar1, Dr. Gyanendra Kumar1




Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2025 Successful Management of a Rare Pediatric Proximal Humerus Fracture-Dislocation Using K-Wire Fixation: A Case Report
May 1, 2025 Successful Management of a Rare Pediatric Proximal Humerus Fracture-Dislocation Using K-Wire Fixation: A Case Report May 11, 2018 Spontaneous Retroperitoneal Hematoma Presenting as Femoral Neuropathy in a Patient on Low Molecular Weight Heparin Therapy
May 11, 2018 Spontaneous Retroperitoneal Hematoma Presenting as Femoral Neuropathy in a Patient on Low Molecular Weight Heparin Therapy October 10, 2016 Modified Boyd’s Dual Onlay Bone Graft Technique for 15 Years Old Neglected Nonunion Fracture both Bone Forearm with Severe Angular Deformity: Case Report
October 10, 2016 Modified Boyd’s Dual Onlay Bone Graft Technique for 15 Years Old Neglected Nonunion Fracture both Bone Forearm with Severe Angular Deformity: Case Report December 1, 2025 Total Hip Arthroplasty for Neglected Hip Dislocation – Surgical Technique and Results
December 1, 2025 Total Hip Arthroplasty for Neglected Hip Dislocation – Surgical Technique and Results