
Magnetic resonance imaging Modic type I changes strongly correlate with histopathological inflammation in lumbar degenerative disc disease and may serve as a useful non-invasive marker of active disease.
Dr. Ravisha Gautam, Department of Orthopaedics, International University of Science and Medicine, Bishkek, Kyrgyzstan. E-mail: ravishagautam007@gmail.com
Abstract
Introduction: Lumbar degenerative disc disease (DDD) is a condition that is a major cause of individuals having persistent lower back pain and functional deficits. Modic endplate alterations detected using magnetic resonance imaging (MRI) have evolved into key diagnostic features for evaluating vertebral and disc pathologies. Researchers have yet to carry out adequate studies to ascertain the relationship between histopathological inflammatory activity and these imaging outcomes.
Materials and Methods: This hospital-based cross-sectional analytical study included 50 patients with lumbar DDD undergoing surgical intervention. Pre-operative MRI was used to classify Modic endplate changes into Types I, II, and III categories. Vertebral endplate and disc tissue samples were collected intraoperatively for histopathological assessment of inflammatory activity. The authors analysed their data with the help of the Statistical Package for the Social Sciences 26.0. The researchers conducted Chi-square testing to identify the relationship between Modic types and inflammation, with P < 0.05 as the threshold for testing the relationship between the two.
Results: Modic Type II changes appeared in 44% of the 50 patients, whereas Type I changes showed up in 40%, and Type III changes appeared in 16% of the cases. In 42% of cases, doctors observed moderate inflammation, whereas 30% showed severe inflammation. The study found that Modic Type I changes developed a strong link to severe inflammatory activity because 50% of Type I cases showed severe inflammation. The study showed that Type II changes mainly caused mild-to-moderate inflammation. The study found a statistically significant correlation between Modic changes and histopathological inflammation (P = 0.002). The study found that higher inflammation grades resulted in increased pain severity.
Conclusion: The research demonstrates that MRI Modic endplate changes, which include Type I changes, show a strong link to histopathological inflammatory activity that occurs in lumbar DDD. The study results show that MRI functions as an effective non-invasive method to evaluate internal inflammation, which helps medical professionals make treatment decisions.
Keywords: Endplate inflammation, histopathology, lumbar degenerative disc disease, Modic changes, magnetic resonance imaging.
Lumbar degenerative disc disease (DDD) is the main reason why individuals all over the globe experience chronic low back pain, which in turn causes impairments. Because the illness has a negative effect on both developed and developing countries in terms of medical expenditures and quality of life, it drives up healthcare prices. Intervertebral disc and vertebral body degeneration, as well as the age-related decline in disc hydration and proteoglycan content, annular fissure development, and biomechanical instability, all play a role in the onset of DDD [1]. In recent years, there has been a surge in interest in studying alterations in vertebral endplates as a possible sign of the degenerative processes that underlie DDD [2]. According to Modic et al., there are three distinct ways to categorise the alterations they first identified based on the magnetic resonance imaging (MRI) signal’s characteristics. When persons undergo Modic Type I modifications, the highest correlation between active inflammatory processes and pain sensations is established [3,4]. Since the intervertebral disc does not get blood flow, the vertebral endplate functions as the principal mechanism that nourishes the disc while preserving its structural integrity. Reportedly, endplate degeneration or injury leads to functional loss, which in turn causes more disc damage and sets off inflammatory processes (report 5). The development of vascular granulation tissue, increased cytokine production, and the arrival of inflammatory cells all contribute to an ongoing state of inflammation within the vertebral bone marrow, as shown by histopathological evidence, leading to Modic Type I changes [5,6]. Degeneration occurs via fatty marrow replacement due to Modic Type II alterations, according to the research, as this condition exhibits less active inflammation that occurs between two distinct stages of degeneration [7]. Researchers have made some progress, but they still do not know how the Modic alterations seen by MRI correlate with the histological signs of inflammation in patients. Because of its better soft-tissue contrast, MRI has become the gold standard for assessing spinal degenerative diseases, allowing for the early identification of biochemical and structural abnormalities. Since MRI findings cannot be directly compared with histological data, the medical community relies on them as independent evidence. We now know that inflammation is a key driver of pain and the course of DDD illness; so, the medical community must fill this information vacuum by determining the accuracy with which imaging data depict biological changes, particularly inflammation. Better diagnosis accuracy, more therapy choices for doctors, and better patient evaluation with sophisticated prognosis methods may be achieved by establishing a link between MRI modal alterations and histological inflammatory activity [7]. The inflammatory theory indicates that a connection is established when low-grade bacterial infection with Propionibacterium acnes affects Type I Modic changes, which subsequently results in the formation of Modic changes [8]. The medical industry is conducting research on the most effective antibacterial and anti-inflammatory treatments to use on specific groups of patients. Further research is needed to confirm the relationships among these outcomes, which is important in order to grasp their clinical meaning [9]. Histopathological evaluation remains the gold standard for assessing inflammatory activity. Correlating MRI findings with histopathology may improve understanding of disease progression and guide treatment strategies. The most accurate approach for studying inflammatory infiltrates, neovascularisation, cytokine activity, and all other cellular and molecular signs of inflammation is histopathological investigation [10]. The researchers conducted their study to investigate how MRI-identified Modic changes affect the relationship between imaging patterns and clinical symptoms. The researchers will study lumbar degenerative disc degeneration patients to find out if histological inflammatory activity corresponds with MRI Modic end-plate changes. We need to understand this relationship because it will help us develop better diagnostics and treatments for DDD and create specific evidence-based management methods. The researchers demonstrate how radiological imaging relates to disease processes to achieve better patient outcomes.
Study design:
This hospital-based cross-sectional analytical study was conducted in the Departments of Orthopaedics, Radiology, and Pathology of a tertiary care teaching hospital over a period of 18 months (January 2024–June 2025) to evaluate the relationship between MRI Modic endplate changes and histopathological inflammatory activity in patients with lumbar DDD. The study protocol was approved by the Institutional Ethics Committee, and written informed consent was obtained from all participants before enrolment in the study.
Participants:
Inclusion criteria:
- Patients aged between 18 and 70 years
- Patients diagnosed with lumbar DDD based on clinical and radiological findings
- Patients undergoing lumbar spine surgery (discectomy/laminectomy/spinal fusion)
- Patients with pre-operative MRI showing Modic endplate changes
- Patients who provided written informed consent.
Exclusion criteria:
- Patients with spinal infections (e.g., tuberculosis, pyogenic spondylodiscitis)
- Patients with spinal tumors or metastatic lesions
- Patients with previous lumbar spine surgery
- Patients with inflammatory spinal disorders (e.g., ankylosing spondylitis)
- Patients on long-term immunosuppressive therapy
- Patients are unwilling to participate in the study.
Study sampling:
A purposive sample was used to select people who were eligible to take part in the research. The orthopaedic outpatient clinic assessed patients who showed symptoms of lumbar degenerative disc disease. The researchers evaluated all surgical candidates who took part in the trial until they had the required sample size. This strategy allowed researchers to include all patients with pertinent medical history and tissue samples to be analysed by histopathology.
Study sample size:
A total of 50 patients were included in the study. As this was an exploratory cross-sectional study involving surgically treated patients with available histopathological specimens, the sample size was determined based on the expected case volume during the study period, feasibility considerations, and sample sizes reported in previous studies evaluating Modic changes and inflammatory activity. No formal a priori sample size calculation was performed.
Study parameters:
The study utilised three types of Modic endplate changes (Type I, Type II, and Type III) MRI results as its primary variables, together with histopathological data, which showed inflammatory cell infiltration, vascular proliferation, oedema, and fibrosis, and the presence of viable granulation tissue. The researchers used clinical data that contained information about symptom duration and pain intensity and treatment outcomes, together with demographic data that comprised age and sex. The researchers implemented a systematic method to gather and analyze the studied parameters.
Study procedure:
All eligible patients underwent clinical assessment together with lumbar spine MRI, which followed standard medical procedures. Experienced radiologists conducted their review of MRI findings in order to determine the Modic changes classification. Patients received surgical treatment after doctors assessed their medical requirements. The surgical team collected vertebral endplate tissue samples together with adjacent disc tissue specimens, which they obtained through sterile methods. The samples were immediately treated with formalin and sent to the pathology department for examination. Histopathological examination used haematoxylin and eosin staining together with special stains, which were applied when required. A pathologist who did not know the MRI results assessed both the presence and the severity of inflammatory changes.
Study data collection:
The research team used a pre-existing form to collect study data. The researchers meticulously documented patient demographic information along with their medical background and MRI findings, surgical results, and tissue analysis results. The histopathological data delivered both qualitative and semi-quantitative assessments of inflammatory conditions, whereas the MRI data demonstrated the specific type and severity of Modic changes. The research team maintained the complete accuracy of all database entries they created.
Data analysis:
The researchers used the Statistical Package for the Social Sciences (SPSS) 26.0 to conduct their data analysis. The study used mean values and standard deviations to present continuous data while using frequency counts and percentage distributions to present categorical data. The researchers used Fisher’s exact test and the Chi-square test to examine the relationship between MRI modalities and histological inflammatory status. The researchers considered results to be statistically significant when the P-value fell below the 0.05 threshold. The researchers established the level of correlation between variables where it was considered necessary.
A total of 50 patients with lumbar DDD undergoing surgical intervention were included in the study. The majority of patients were aged 41–50 years (30%), and males constituted 64% of the study population. Most patients had symptoms for more than 12 months (40%). The L4–L5 level was the most commonly affected disc level (48%), followed by L5–S1 (40%) (Table 1).
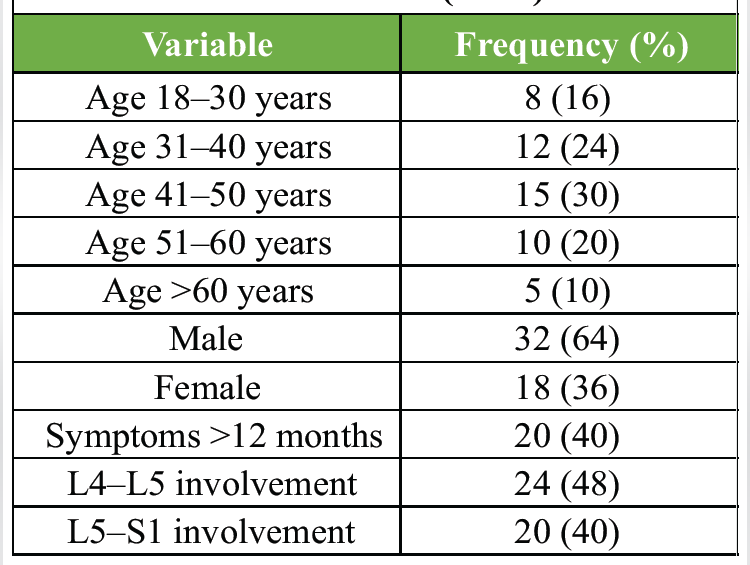
Table 1: Baseline demographic and clinical characteristics (n=50)
MRI evaluation demonstrated Modic Type II changes in 44% of patients, followed by Type I changes in 40% and Type III changes in 16%. Histopathological examination revealed moderate inflammatory activity in 42% of cases, severe inflammation in 30%, and mild inflammation in 28%. A significant association was observed between Modic type and inflammatory activity (χ2 test, P = 0.002). Severe inflammation was most frequently observed in patients with Modic Type I changes, whereas Modic Type II changes were predominantly associated with mild-to-moderate inflammatory activity (Table 2 and Fig. 1).
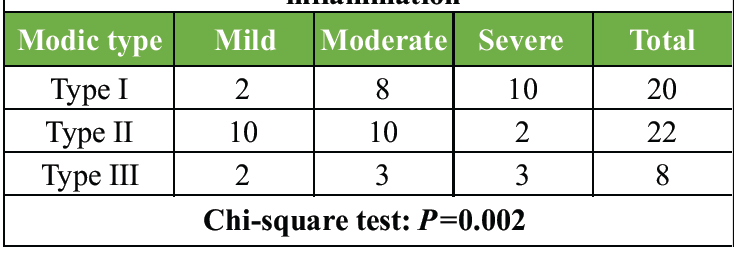
Table 2: Correlation between magnetic resonance imaging Modic changes and histopathological inflammation
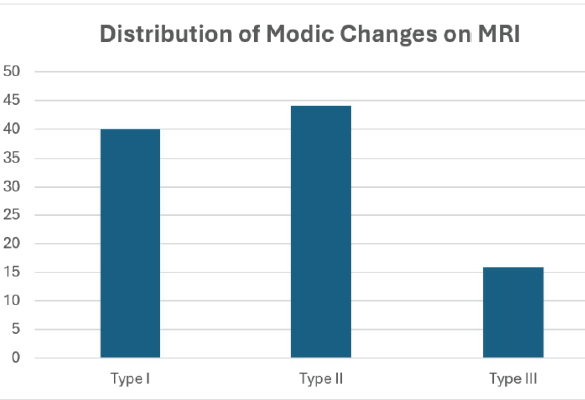
Figure 1: Distribution of magnetic resonance imaging Modic endplate changes and corresponding histopathological inflammatory activity among study participants.
Pain severity showed a positive correlation with histopathological inflammation. Severe pain (Visual Analogue Scale [VAS] 7–10) was reported by 48% of patients, whereas moderate pain was observed in 40%. Among patients with severe inflammatory activity, 86.7% reported severe pain. Increasing inflammatory grades were associated with greater pain severity, indicating a significant relationship between biological inflammation and clinical symptom burden (Table 3 and Fig. 2).
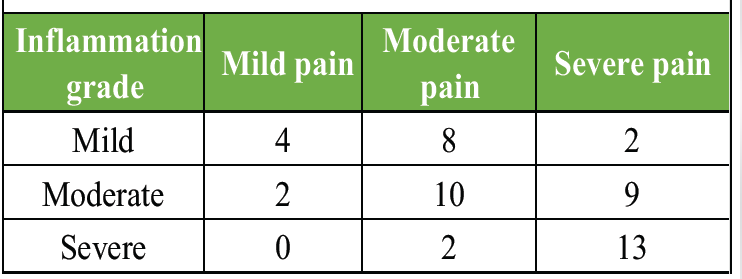
Table 3: Correlation between pain severity and histopathological inflammation
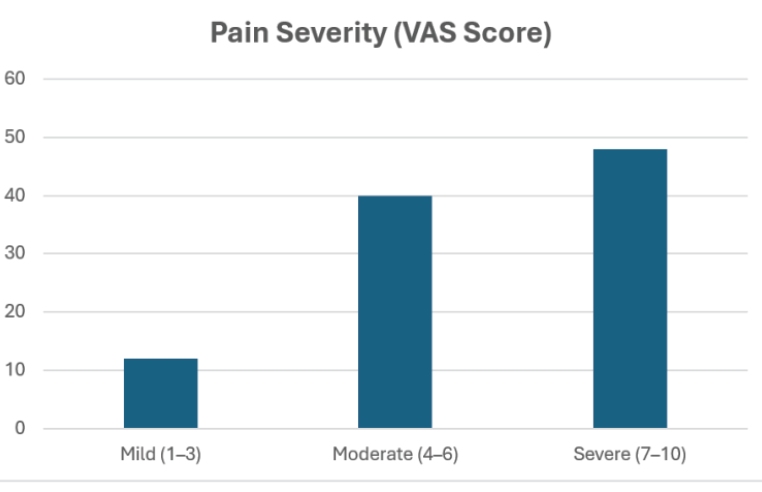
Figure 2: Relationship between pain severity (Visual Analog Scale score) and histopathological inflammatory activity in lumbar degenerative disc disease.
Overall, the findings demonstrated that Modic Type I changes were strongly associated with active inflammatory pathology and higher pain intensity, whereas Type II and Type III changes represented relatively less active stages of degeneration. These results support the role of MRI as a reliable non-invasive indicator of underlying inflammatory activity in lumbar DDD.
The authors investigated the correlation between MRI Modic endplate alterations and histopathological inflammatory activity in lumbar DDD. It was discovered that the Modic Type I alterations were strongly linked with increased inflammatory activity and that the intensity of inflammation directly influenced the intensity of pain. Based on the existing data, vertebral endplate pathology is one of the primary factors that contribute to the development and expression of DDD symptoms. Although contributing to the body of knowledge, the findings of the study shed some light on the relationship between endplate changes, Modic changes, and degenerative changes. The relationship between degeneration and inflammation appears to be bidirectional. Degenerative changes in the vertebral endplate and intervertebral disc may initiate inflammatory responses through structural disruption, cytokine release, and vascular ingrowth, while persistent inflammation may further accelerate disc degeneration and endplate damage. In the present study, Modic Type I changes were associated with higher inflammatory activity, supporting the concept that active degeneration and inflammation coexist during the early phases of disease progression. Although symptom duration was recorded, no formal statistical analysis was performed to evaluate the association between disease duration and Modic type. Future studies with larger sample sizes should investigate whether longer disease duration is associated with progression from Modic Type I to Type II or Type III changes [11]. Moderate-to-severe histopathological inflammation cases showed a higher likelihood of developing Modic Type I alterations according to the research findings. Pathophysiology currently demonstrates that Modic Type I changes represent an active stage of inflammation, which creates vascular granulation tissue combined with bone marrow oedema. Feng et al. demonstrated through their research that structural endplate damage triggers Modic changes by establishing a strong connection between vertebral endplate abnormalities and Modic changes, which they measured with an odds ratio of 4.29 and a P < 0.001. The findings revealed that 27.8% of endplates showed endplate defects, which caused a decrease in disc height and an increase in bulging and a decrease in disc signal intensity, all of which indicated disc degeneration. The research shows that structural degradation and what researchers consider Modic Type I changes both strongly correlate with the presence of inflammatory activity [12]. The research states that Type II Modic changes are signs of active fatty degeneration, and Type I changes are 40 times slower. These percentages are consistent with the trends observed in spinal degeneration. The findings showed that Type II changes were more prevalent than Type I changes, but Type II changes resulted in less severe inflammation. Results are in line with earlier research that has associated the alterations in the Modic Type I (M1), Modic Type II (M2), and bone endplate lesions with the different levels of pain experienced throughout the trial. Weakening the M1 and disc signals relieved the pain of 49 patients with persistent low back pain who had ongoing M1 lesions along with reduced disc height and increasing endplate lesions. This study demonstrates the mechanism of Modic changes as clinical predictors of ongoing pathological conditions, as 36% of the patients still experienced pain during the 1-year follow-up. In line with other research, this study established that increased inflammation correlates with increased pain and that Modic Type I is a predictor of chronic disease [13]. The present study, with a P = 0.002, showed that MRI results are a true reflection of latent biological processes, as they have created a statistically significant correlation between the changes in the Modic and histological inflammation. This discovery is credible due to the findings of Lv et al., who studied 75 patients to determine the correlation between endplate defects and Modic changes, disc degeneration, and facet joint disease. Their study found a strong relationship between the grade of endplate abnormalities and disc degeneration, Modic Type II changes, and clinical outcomes such as the VAS and the Oswestry disability index (ODI). The conclusion of the present study that the incidence rate of endplate defects was 48% was consistent with the finding of the previous study that endplate defects were more severe at L4-L5 levels. The two studies have shown consistent results that indicate that this area experiences greater mechanical stress, which exposes it to inflammatory and degenerative diseases [14]. The researchers of this study found a relationship between the level of pain and inflammation in their studies. The research demonstrated that severe inflammation brought about excruciating pain because the symptoms stemmed from inflammatory activities in the bone marrow and spinal endplates. Lv et al. [14] demonstrated a positive correlation between structural degenerative changes and clinical outcome measures, including VAS and ODI scores, indicating that both inflammatory and degenerative processes contribute significantly to symptom severity. These observations support the findings of the present study, which showed that higher grades of histopathological inflammation were associated with greater pain intensity in patients with lumbar DDD. The vertebral endplate is the main structural component that leads to disc degeneration, according to Rajasekaran et al. [15], who showed that the disc, endplate, and bone marrow collaborate as a disc-endplate-bone marrow complex. Any degeneration of any of the components, as demonstrated in the review, leads to structural cross-talk, which subsequently leads to chronic inflammation in the spinal bone marrow. This study validates earlier studies that MRI-identified inflammatory changes are in line with histological evidence of inflammation. This paper demonstrates that the unified diseased complex explains the inflammatory activity and structural deterioration, and it also explains the Modic changes and other imaging findings. To gain a more comprehensive insight into inflammatory disorders, the article by Rajasekaran et al. [16] provides a novel definition of the disc-endplate-bone-marrow complex (DEBC) that utilises MRI results and short tau inversion recovery sequence data. The seven levels of activity observed in the 8680 endplates of 1085 individuals with low back pain included acute Type A inflammation and chronic Type B inflammation, the latter being the most prevalent (51.8%). The researchers found that disc herniation with active DEBC changes was linked to a much higher risk of post-operative infection (2.4 vs. 0.47; P 0.002) and the highest odds ratio of surgical requirement (5.2). Based on the results of the study, patients with degenerative spine diseases can significantly benefit when the inflammatory activity is properly identified. The study did not employ DEBC categorisation, but it did establish a relationship between the changes in Modic Type I and the histopathological inflammation, which supports the active disease states outlined in the DEBC system. Findings from this research are consistent with those from Feng et al., showing that endplate disease is associated with disc degeneration. There is a direct correlation between endplate abnormalities and Modic alterations in the distribution of the lumbar spine, as shown by the study conducted by Feng et al. Disc signal intensity and height were both decreased as a result of these anomalies, confirming the earlier onset of degeneration due to endplate injury. The present work contributes to this knowledge by showing that histologically detectable inflammatory activity occurs with such structural alterations. Consistent with the expected progression of DDD, whose symptoms often manifest in the 40s and 50s, the majority of the participants in the current research are middle-aged, meaning they are between the ages of 41 and 50. According to the study that was used to conduct the comparison, 64% of the respondents were men, suggesting that their physical activity and working circumstances caused them to have higher levels of spinal degeneration. Because Type I changes indicate the presence of inflammation in lumbar DDD, the present study provides critical evidence that MRI Modic modifications have clinical relevance [12]. The research establishes a connection between imaging results and biological processes through histopathology and radiology outcomes. The results show that Modic changes, endplate abnormalities, and disc degeneration are linked to clinical symptoms, which now display characteristics of disc, endplate, and bone marrow disorders. The statement needs to include that MRI serves as a valuable tool to provide essential data concerning both structural changes and inflammatory processes. Nevertheless, it is important to emphasise that MRI might fail to detect all disease processes, as stated by Rajasekaran et al. [15]. MRI might need to be reclassified in the DEBC system. To gain complete insight into DDD, the research study involves imaging techniques and histopathological research. The strengths of this study include direct histopathological assessment and correlation with MRI findings. Limitations include the relatively small sample size, single-centre design, and inclusion of only surgically treated patients, which may limit generalisability.
MRI Modic endplate changes, particularly Type I changes, demonstrate a significant association with histopathological inflammatory activity in lumbar DDD. MRI may therefore serve as a valuable non-invasive tool for identifying active inflammatory disease and guiding clinical decision-making.
Modic Type I changes on MRI may indicate active inflammation in lumbar degenerative disc disease and can assist clinicians in identifying patients who may benefit from targeted treatment strategies.
References
- 1. Hartvigsen J, Hancock MJ, Kongsted A, Louw Q, Ferreira ML, Genevay S, et al. What low back pain is and why we need to pay attention. Lancet 2018;391:2356-67. [Google Scholar] [PubMed]
- 2. Zehra U, Cheung JP, Bow C, Lu W, Samartzis D. Multidimensional vertebral endplate defects are associated with disc degeneration, modic changes, facet joint abnormalities, and pain. J Orthop Res 2019;37:1080-9. [Google Scholar] [PubMed]
- 3. De Roos A, Kressel H, Spritzer C, Dalinka M. MR imaging of marrow changes adjacent to end plates in degenerative lumbar disk disease. AJR Am J Roentgenol 1987;149:531-4. [Google Scholar] [PubMed]
- 4. Modic MT, Steinberg PM, Ross JS, Masaryk TJ, Carter JR. Degenerative disk disease: Assessment of changes in vertebral body marrow with MR imaging. Radiology 1988;166:193-9. [Google Scholar] [PubMed]
- 5. Modic MT, Masaryk TJ, Ross JS, Carter JR. Imaging of degenerative disk disease. Radiology 1988;168:177-86. [Google Scholar] [PubMed]
- 6. Jensen TS, Karppinen J, Sorensen JS, Niinimaki J, Leboeuf-Yde ¨C. Vertebral endplate signal changes (Modic change): A systematic literature review of prevalence and association with nonspecific low back pain. Eur Spine J 2008;17:1407-22. [Google Scholar] [PubMed]
- 7. Manniche C. Vertebral endplate (modic) changes and the treatment of back pain using antibiotics. Clin Pract 2014;11:585-90. [Google Scholar] [PubMed]
- 8. Ninomiya K, Fujita N, Hosogane N, Hikata T, Watanabe K, Tsuji O, et al. Presence of modic type 1 change increases risk of postoperative pyogenic discitis following decompression surgery for lumbar canal stenosis. J Orthop Sci 2017;22:988-93. [Google Scholar] [PubMed]
- 9. Kumarasamy D, Rajasekaran S, Anand KS, Soundararajan DC, Shetty AP, Kanna RM, et al. Lumbar disc herniation and preoperative modic changes: A prospective analysis of the clinical outcomes after microdiscectomy. Global Spine J 2022;12:940-51. [Google Scholar] [PubMed]
- 10. Farshad-Amacker NA, Hughes A, Herzog RJ, Seifert B, Farshad M. The intervertebral disc, the endplates and the vertebral bone marrow as a unit in the process of degeneration. Eur Radiol 2017;27:2507-20. [Google Scholar] [PubMed]
- 11. Lyu FJ, Cui H, Pan H, Mc Cheung K, Cao X, Iatridis JC, et al. Painful intervertebral disc degeneration and inflammation: From laboratory evidence to clinical interventions. Bone Res 2021;9:7. [Google Scholar] [PubMed]
- 12. Feng Z, Liu Y, Yang G, Battié MC, Wang Y. Lumbar vertebral endplate defects on magnetic resonance images: Classification, distribution patterns, and associations with modic changes and disc degeneration. Spine (Phila Pa 1976) 2018;43:919-27. [Google Scholar] [PubMed]
- 13. Luoma K, Vehmas T, Kerttula L, Grönblad M, Rinne E. Chronic low back pain in relation to Modic changes, bony endplate lesions, and disc degeneration in a prospective MRI study. Eur Spine J 2016;25:2873-81. [Google Scholar] [PubMed]
- 14. Lv B, Yuan J, Ding H, Wan B, Jiang Q, Luo Y, et al. Relationship between endplate defects, modic change, disc degeneration, and facet joint degeneration in patients with low back pain. BioMed Res Int 2019;2019:9369853. [Google Scholar] [PubMed]
- 15. Rajasekaran S, Ramachandran K, Sri Vijay Anand KS, Kanna RM, Shetty AP. From Modic to disc endplate bone marrow complex – the natural course and clinical implication of vertebral endplate changes. Global Spine J 2025;15:196-209. [Google Scholar] [PubMed]
- 16. Rajasekaran S, Pushpa BT, Murugan C, Mengesha MG, Easwaran M, Naik AS, et al. The disc-endplate-bone-marrow complex classification: Progress in our understanding of Modic vertebral endplate changes and their clinical relevance. Spine J 2024;24:34-45. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 December 1, 2025 MRI–Histopathology Correlation of Cartilage and Bone in Early Knee Osteoarthritis
December 1, 2025 MRI–Histopathology Correlation of Cartilage and Bone in Early Knee Osteoarthritis October 1, 2025 Giant Cell Tumor of the Tendon Sheath: Case Series and Review of Literature
October 1, 2025 Giant Cell Tumor of the Tendon Sheath: Case Series and Review of Literature April 1, 2025 Soft Tissue Sarcoma Masquerading as Chronic Hematoma: A Case Report and Literature Review
April 1, 2025 Soft Tissue Sarcoma Masquerading as Chronic Hematoma: A Case Report and Literature Review August 1, 2026 Not All Red Flags Indicate Malignancy: A Case Report of a Benign Lipoma Mimicking Soft-tissue Sarcoma
August 1, 2026 Not All Red Flags Indicate Malignancy: A Case Report of a Benign Lipoma Mimicking Soft-tissue Sarcoma