
We can learn from the article that multiple synovial osteochondromatosis results in degeneration of the hip, even surgical intervention has been implemented.
Dr. Yi min Zhang,
Department of Joint Surgery, Weifang People’s Hospital, Weifang, China.
E-mail: ymzh69@hotmail.com
Abstract
Introduction: Primary synovial osteochondromatosis of the hip is a benign disorder, which is not frequently seen clinically. The characteristic of this disease is proliferation of synovium and formation of loose bodies inside the joint. It is known that only the loose bodies derived from synovium were called synovial osteochondromatosis. Although it can take place in any joint, the knee is most commonly affected, involvement of the hip joint is relatively rare. We report a young man who has multiple synovial osteochondromatosis in his left hip.
Case Presentation: A 21‑year‑old young man, who had progressive pain and functional impairment of his left hip, came to our hospital. He complained that 2 years ago, he began to feel painful of his left hip joint when walking and squatting. Physical examination found that the motion range of the hip was obviously limited, with internal rotation, abduction in particular. The Harris hip score was just 38 points. X‑ray shew multiple osteochondromatosis with mild degenerative osteoarthritis existing inside the hip joint. Magnetic resonance imaging shew that the synovial osteochondromatosis intersperse inside the hip joint. During the operation, posterolateral incision of the hip was chosen with dislocation of the femoral head for total exposure of the hip joint to debride extensive loose bodies and proliferative synovial tissue. Pulse irrigation was applied to flush out the residuals. More than 872 of osteochondromatosis were removed out of the hip joint (some small ones were sucked during the operation). The size of the loose bodies ranged from 3 cm × 3 cm × 2.5 cm to 0.2 cm × 0.2 cm × 0.15 cm. Post‑operation radiography shew most pathological tissues were taken out. After the operation, the patient rehabilitated fast. The pain relieved and he could bear weight and walked 3 days postoperatively. 1 and 3 months postoperatively, the patient came to us for visit, and he said that he just had a relatively satisfactory function of his affected hip. He could walk, slowly run, and squat freely. But sometimes he could feel a bit painful on his left hip joint after long walking and fatigue. And sometimes he could feel and hear mild crepitus on the left hip joint. 12 months later, the patient came again and complained that the pain of his operated hip became a bit more serious than before since about 20 days ago. The range (internal rotation, abduction in particular) of this hip joint could not live up to normal, compared with the uninvolved hip in physical examination. X‑ray shew osteoarthritis had become a bit severer. The patient accepted the suggestion of prospective total hip replacement.
Conclusion: Multiple synovial osteochondromatosis is not a very uncommon condition. However, there may be unusual presentations. It can take place in any joint, the knee is most commonly affected, however, involvement of the hip joint is relatively rare as was seen in our patient.
Keywords: Primary synovial osteochondromatosis, hip joint, surgery.
Primary synovial osteochondromatosis of the hip is a benign disorder, which is not frequently seen clinically. The characteristic of this disease is proliferation of synovium and formation of loose bodies inside the joint. It is known that only the loose bodies derived from synovium were called synovial osteochondromatosis. Although it can take place in any joint, the knee is most commonly affected, involvement of the hip joint is relatively rare [1,2,3]. We report a young man who has multiple synovial osteochondromatosis in his left hip.
A 21‑year‑old young man, who had progressive pain and functional impairment of his left hip, came to our hospital. He complained that 2 years ago, he began to feel painful of his left hip joint when walking and squatting. And crepitation also occurred inside the affected hip joint. Sometimes he could feel swelling after aggravating activities. During the 2 years, the stated symptoms became more and more severe. Physical examination found that the motion range of the hip was obviously limited, with internal rotation, abduction in particular. The Harris Hip Score [4]was just 38 points. X‑ray shew multiple osteochondromatosis with mild degenerative osteoarthritis existing inside the hip joint (Fig. 1). The patient underwent magnetic resonance imaging (MRI) to confirm the clinical diagnosis and aid surgical planning. MRI shew that the synovial osteochondromatosis intersperse inside the hip joint (Fig. 2). Then, operation was decided on this young patient under epidural anesthesia. During the operation, posterolateral incision of the hip was chosen with dislocation of the femoral head for total exposure of the hip joint to debride extensive loose bodies and proliferative synovial tissue. Pulse irrigation was applied to flush out the residuals. More than 872 of osteochondromatosis were removed out of the hip joint (some small ones were sucked during the operation). The size of the loose bodies ranged from 3 cm × 3 × 2.5 cm to 0.2 cm × 0.2 cm × 0.15 cm (Fig. 3). Post‑operation radiography shew most pathological tissues were taken out (Fig. 4). After the operation, the patient rehabilitated fast. The pain relieved and he could bear weight and walked 3 days postoperatively. 10 days later, he was dismissed from the hospital.

About 1 and 3 months postoperatively, the patient came to us for visit, and he said that he just had a relatively satisfactory function of his affected hip. He could walk, slowly run, and squat freely. But sometimes he could feel a bit painful on his left hip joint after long walking and fatigue. And sometimes he could feel and hear mild crepitus on the left hip joint.

About 12 months later, the patient came again and complained that the pain of his operated hip became a bit more serious than before since about 20 days ago. The range (internal rotation, abduction in particular) of this hip joint could not live up to normal, compared with the uninvolved hip in physical examination. X‑ray shew osteoarthritis had become a bit severer (Fig. 5). The patient accepted the suggestion of prospective total hip replacement.
Primary synovial osteochondromatosis of the hip joint, a rare benign condition characterized by multiple intra‑articular osteochondral loose bodies and synovial hyperplasia may result in mechanical symptoms and degenerative osteoarthritis. Synovectomy and loose bodies removal through open operation [1,5,6] or arthroscopy [7,8] is a reliable procedure that can effectively relieve symptoms. Pre‑operative MRI can evaluate the configuration of intra‑articular bodies, the presence of effusion, synovial proliferation and hypertrophy, the condition of cartilage, and extra‑articular of the disease [9,10]. On the basis of the location and extent of the osteochondromatosis by MRI, the operative approach can be determined to implement enough debridement. Sometimes, the decision that the femoral head should be dislocated or remain in place during operation could be made in advance through preoperative MRI. It has been reported that arthroscopic technique is suitable for such disease. But for this patient who has multiple synovial osteochondromatosis, open surgery remain more effective value than arthroscopy. To our knowledge, the quality of hip synovial osteochondromatosis in our case has never been reported by other authors previously. Unfortunately, symptoms of osteoarthritis occurred 1 year after surgery, the reason of which might include: (1) The destroy of articular cartilage by protopathy; (2) dislocation of femoral head during operation; (3) recurrence from residual pathological synovium. All the above factors can accelerate the process of osteoarthritis.
Multiple synovial osteochondromatosis is not a very uncommon condition. However, there may be unusual presentations. It can take place in any joint, the knee is most commonly affected, however, involvement of the hip joint is relatively rare as was seen in our patient.
It is reported that the location of multiple synovial osteochondromatosis lies in the knee joint, but we first find that hip joint could be also the site of multiple synovial osteochondromatosis. Further observation and study are needed.
References
- 1. Mussey RD Jr, Henderson MS. Osteochondromatosis. J Bone Joint Surg Am 1949;31A(3):619‑627. [Google Scholar] [PubMed]
- 2. Maurice H, Crone M, Watt I. Synovial chondromatosis. J Bone Joint Surg Br 1988;70(5):807‑811. [Google Scholar] [PubMed]
- 3. Shpitzer T, Ganel A, Engelberg S. Surgery for synovial chondromatosis 26 cases followed up for 6 years. Acta Orthop Scand 1990;61(6):567‑569. [Google Scholar] [PubMed]
- 4. Harris WH. Traumatic arthritis of the hip after dislocation and acetabular fractures: Treatment by mold arthroplasty. An end‑result study using a new method of result evaluation. J Bone Joint Surg Am 1969;51(5):737‑755. [Google Scholar] [PubMed]
- 5. Gilbert SR, Lachiewicz PF. Primary synovial osteochondromatosis of the hip: Report of two cases with long‑term follow‑up after synovectomy and a review of the literature. Am J Orthop (Belle Mead NJ) 1997;26(8):555‑560. [Google Scholar] [PubMed]
- 6. Gille J, Krueger S, Aberle J, Boehm S, Ince A, Loehr JF. Synovial chondromatosis of the hip: A case report and clinicopathologic study. Acta Orthop Belg 2004;70(2):182‑188. [Google Scholar] [PubMed]
- 7. Chen CY, Chen AC, Chang YH, Fu TS Synovial chondromatosis of the hip: Management with arthroscope‑assisted synovectomy and removal of loose bodies: Report of two cases. Chang Gung Med J 2003;26(3):208‑214. [Google Scholar] [PubMed]
- 8. Krebs VE. The role of hip arthroscopy in the treatment of synovial disorders and loose bodies. Clin Orthop Relat Res 2003;(406):48‑59. [Google Scholar] [PubMed]
- 9. Kim SH, Hong SJ, Park JS, Cho JM, Kim EY, Ahn JM, et al. Idiopathic synovial osteochondromatosis of the hip: radiographic and MR appearances in 15 patients. Korean J Radiol 2002;3(4):254‑259. [Google Scholar] [PubMed]
- 10. Robinson P, White LM, Kandel R, Bell RS, Wunder JS. Primary synovial osteochondromatosis of the hip: Extracapsular patterns of spread. Skeletal Radiol 2004;33(4):210‑215. [Google Scholar] [PubMed]
Related Articles in Journal of Orthopaedic Case Reports
 December 10, 2023 Effects of the Percutaneous Carbon Dioxide Therapy on Post-surgical and Post-traumatic Hematoma, Edema and Pain
December 10, 2023 Effects of the Percutaneous Carbon Dioxide Therapy on Post-surgical and Post-traumatic Hematoma, Edema and Pain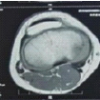 June 1, 2026 Cortical Lytic Lesion of the Proximal Tibia in an 8-Year-Old Child: A Pediatric Diagnostic Conundrum
June 1, 2026 Cortical Lytic Lesion of the Proximal Tibia in an 8-Year-Old Child: A Pediatric Diagnostic Conundrum July 1, 2026 Bizarre Parosteal Osteochondromatous Proliferation: A Case Series and Literature Review
July 1, 2026 Bizarre Parosteal Osteochondromatous Proliferation: A Case Series and Literature Review December 10, 2023 How we do it? Trimalleolar Fractures: Posterolateral Approach for Fixing the Syndesmotic Ligament, Posterior Malleolus, and Fibula
December 10, 2023 How we do it? Trimalleolar Fractures: Posterolateral Approach for Fixing the Syndesmotic Ligament, Posterior Malleolus, and Fibula