
[box type=”bio”] Learning Point of the Article: [/box]
Digital Ischemia following arterial cannulation is still an unsolved mystery, Key for successful outcome lies in knowledge of risk factors immediate recognition and prompt treatment.
Case Report | Volume 10 | Issue 2 | JOCR March – April 2020 | Page 40-45 | Vishal Kumar, Amit Kumar Salaria, Prasoon Kumar, Ekta Dogra, Gaganpreet Singh, Sameer Aggarwal. DOI: 10.13107/jocr.2020.v10.i02.1688
Authors: Vishal Kumar[1], Amit Kumar Salaria[1], Prasoon Kumar[1], Ekta Dogra[2], Gaganpreet Singh[3], Sameer Aggarwal[1]
[1]Department of Orthopaedic Surgery, Post Graduate Institute of Medical Education and Research, Chandigarh, India,
[2]Department of Community Medicine, Post Graduate Institute of Medical Education and Research, Chandigarh, India,
[3]Department of Orthopaedic Surgery, All India Institute of Medical Sciences, Bathinda, India.
Address of Correspondence:
Dr. Amit Kumar Salaria,
Department of Orthopaedic Surgery, Post Graduate Institute of Medical Education and Research, Chandigarh, India.
E-mail: meetamit20salaria@gmail.com
Abstract
Introduction: Iatrogenic digital ischemia following inadvertent intra-arterial injections is well documented. Most of the culprit drugs are used for sedation or in general anesthesia. Proper understanding of the causative factors and pathophysiology is of utmost importance for adequate treatment. There have been conflicting evidences in the numerous studies and theories proposed regarding pathophysiology. We scoped the available literature to find out the cause of digital ischemia in one of the patients presented to us but could not find a convincing answer. Due to incomplete understanding of the pathophysiology, there is no specific treatment protocol. Most important is vigilance regarding risk factors, knowledge of typical medications, immediate recognition of the situation, assessment of the disease progression, anticoagulation, symptomatic treatment, and specific therapy (which varies from case to case) are mainstay of treatment. Further research is warranted to understand the etiopathogenesis so that proper treatment protocol could be established.
Keywords: Digital ischemia, etiopathogenesis, gangrene, polytrauma, intra-arterial.
Introduction
The case of iatrogenic digital ischemia following intra-arterial (IA) injections has been well documented [1, 2, 3, 4]. Most of these documented drugs are used for sedation or general anesthesia. Ischemia could lead to skin necrosis progressing to severe gangrene, requiring subsequent amputations resulting in permanent disabilities. Even when no tissue loss occurs, patients can experience a deficit in fine motor skills, hot-cold hypersensitiveness, and paresthesias. In spite of the various risk factors and drugs which are thought to be important causes of digital ischemia, there could be clinical scenarios in which digital ischemia has occurred without any known reason.
Case Report
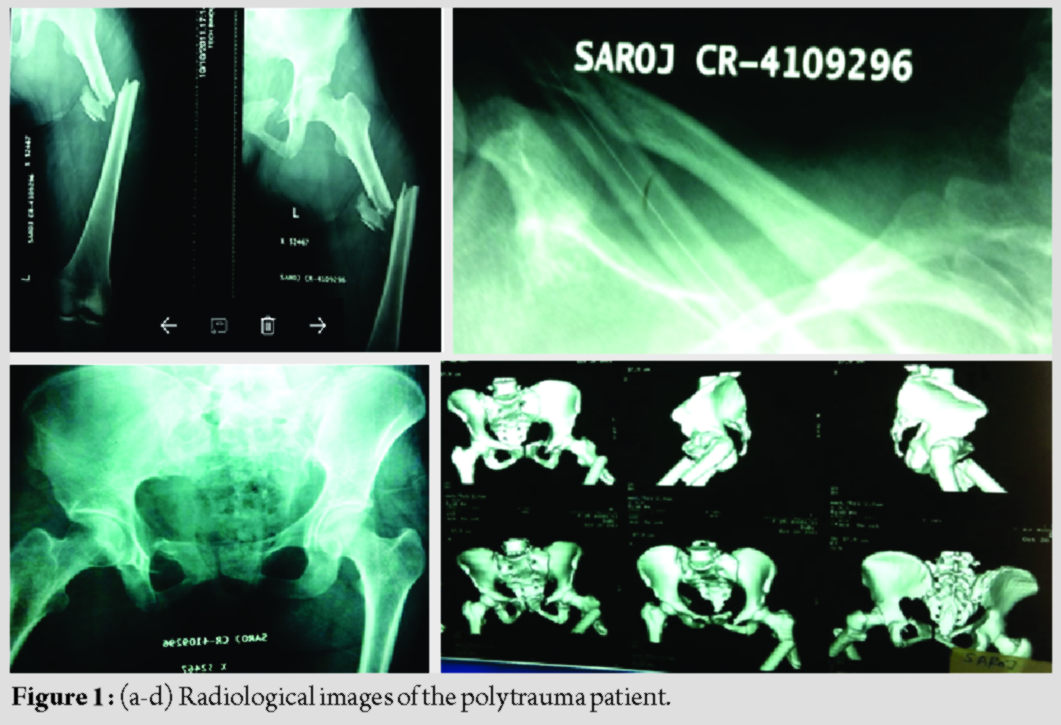
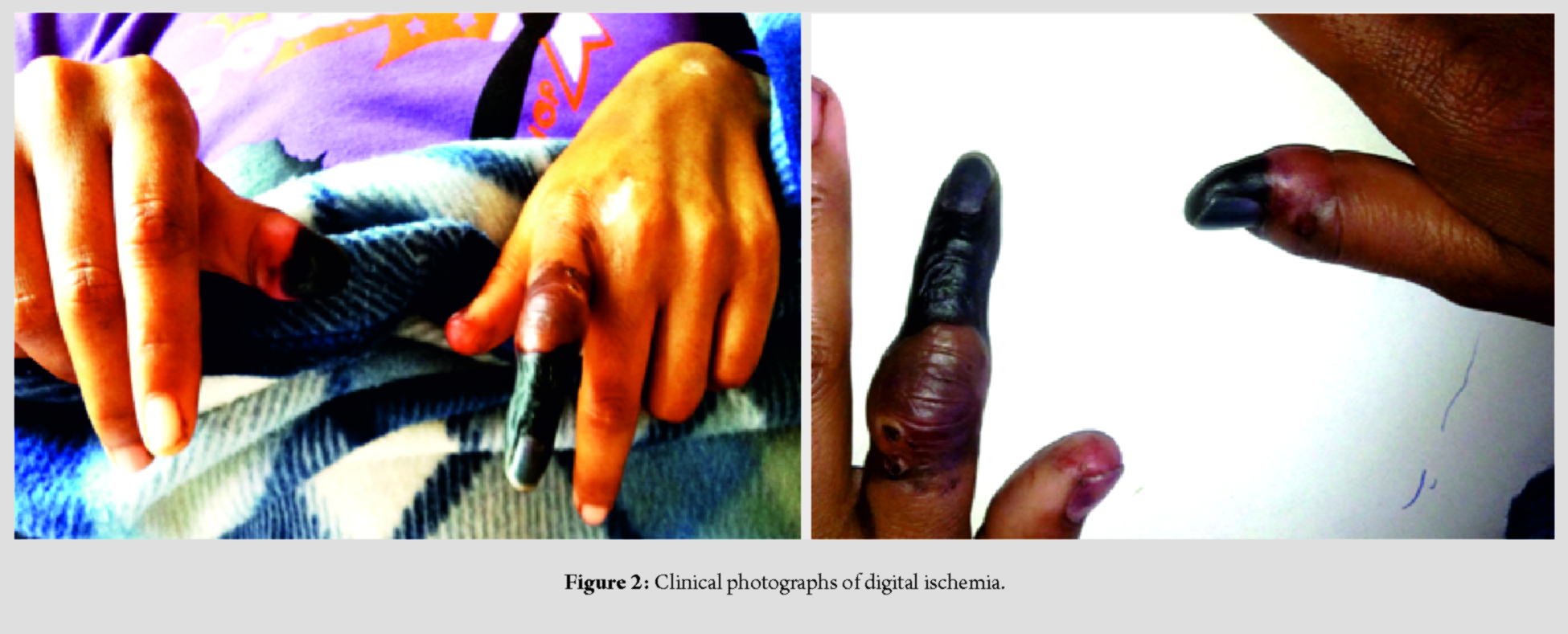
A 45-year-old female patient with polytrauma was referred to our institution with fractures of shaft femur, right clavicle, and pelvis with concomitant abdominal and chest injuries. After initial resuscitation and stabilization, the patient was operated for fracture shaft of femur and the other injuries were managed conservatively (Fig. 1 a, b, c, d, ). Postoperatively, mechanical ventilation was required, and the patient was shifted to the intensive care unit. The brachial artery was cannulated for IA monitoring of blood pressure on the left arm. Subsequently, 3 days after the cannulation, bluish discoloration of the distal end of the index finger was observed. Initially, an accidental drug injection through the arterial line resulting in ischemia was suspected. Since the patient was comatose, brachial artery cannulation on the right side was done for further monitoring. Remarkably, signs of ischemia were now noted on the right thumb 48 h after the cannulation (Fig. 2 a & b). It was confirmed that no drug was given through the cannula on this side. The coagulation profile came out to be normal. Cardiac evaluation turned out to be normal, with the absence of any source of emboli in the cardiac valves or chambers. In spite of giving heparin, papaverine, and oral anticoagulants, the digits could not be saved. Subsequently, the amputation of the digits was done.
We were unable to identify the precipitating factor(s) for ischemia in our patient, and therefore, to understand the probable causative factors and pathophysiology that could have resulted in digital gangrene in our patient, we undertook this scoping review of the literature. We searched PubMed for evaluating the causes of digital ischemia following cannulation of the peripheral arteries. Relevant articles in English published between 1960 until date was reviewed and accordingly, we enlist symptomatology, pathophysiological process, squeal, and the various management modalities that have been documented till date.
Discussion
Symptoms and risk factors
Inadvertent IA injection could lead to immediate or delayed repercussions, distal to injection site [1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11].
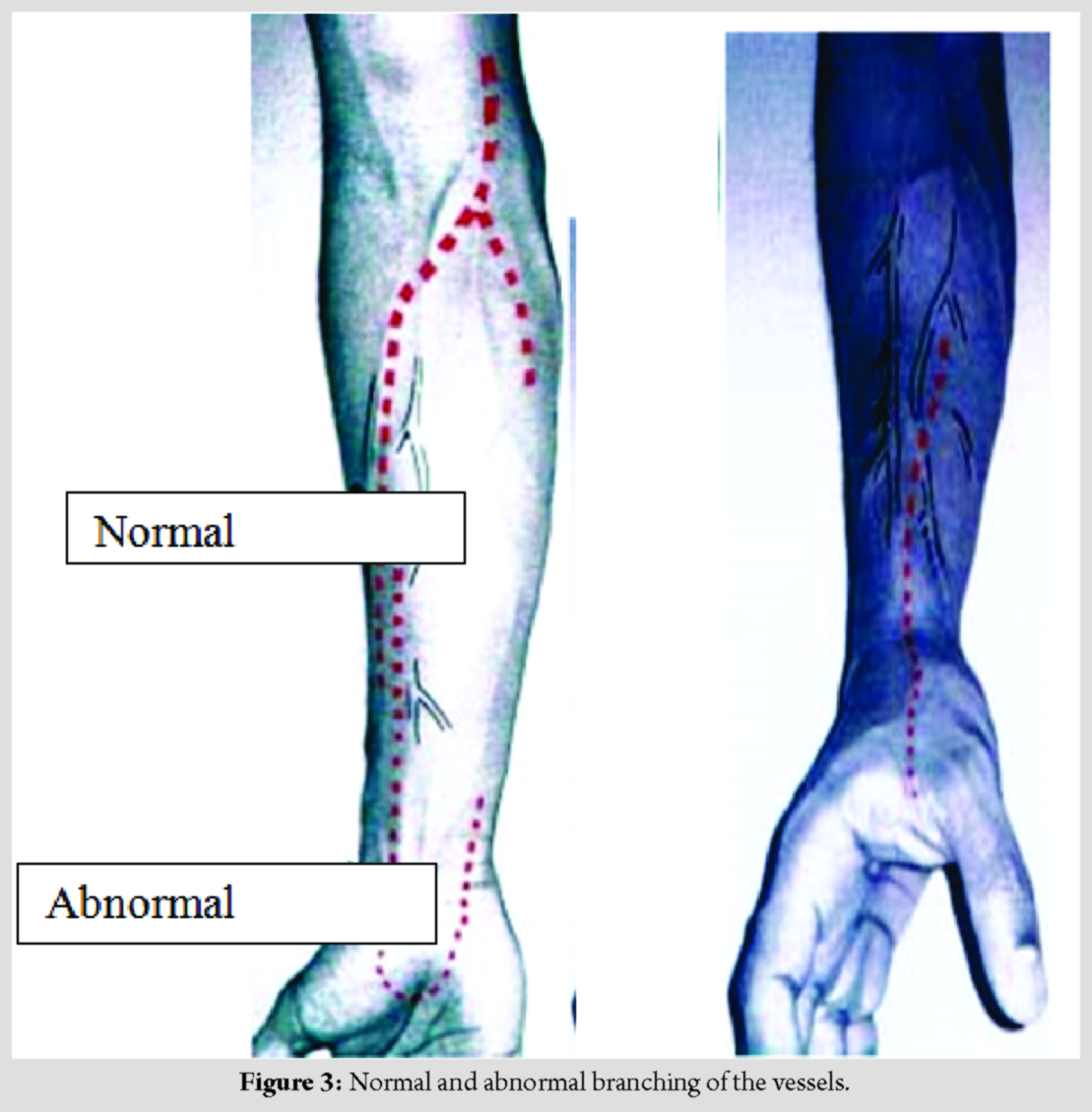
This could manifest as tingling, burning sensation, numbness, and paresthesias. Motor deficits with or without involuntary muscular contractions and flushing and mottling of the skin, are commonly reported [1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12]. Clinical features such as pain, pulseless hands, bluish or pale discoloration, paresthesias, and motor function loss, result due to chronicity with the establishment of compartment syndrome.Ultimately necrosis and gangrene occur, which could lead to permanent loss of function. Chronic pain with or without complex regional pain syndrome may be an eventuality. Since pain is often the only initial symptom, patients who cannot communicate it are at a high risk of progression; comatose patients or those on mechanical ventilation, patients with altered mental status, infants, and trauma victims with distracted by more intense pain elsewhere. Patients at high risk for inadvertent IA injection are those with obesity, those with dark skin, patients of thoracic outlet syndrome, patients with prolonged indwelling arterial catheters, or with pre-existing vascular anomalies of the forearm [1, 2, 3, 13]. Indicators of such injections include bright red back-flow of blood into the cannula with pulsatile blood column movement. Clinicians should be cognizant of these as well as the anatomical locations where arteries and veins are in close proximity, for example, at the elbow. In addition, the pressure reading through the IA cannula increases in the case of any fluid injection through it [1]. However, these indicators subtle and require vast experience on the part of the clinicians to comprehend them. Blood gas analysis or pressure transducers are more reliable to confirm IA injections. In the critical care setting, patients who are often intubated, sedated, and receiving mechanical ventilation, have an IA cannula access for monitoring of blood pressure. They also are recipients of multiple intravenous medications. Therefore, lies the possibility of accidental injections through the IA line rather than the IV lines. In our patient, specifically in the second limb, no IA medication was administered as proper care was taken. Jones et al. have given guidelines for adequate and safe maintenance of an arterial catheter that includes clear labeling and color-coding; no injection ports attached to the IA cannula and educating all health-care professionals involved in administering medications of the consequences of IA injections [6]. A pre-existing vascular aberration such as radial artery with origin above the intercondylar line or with a superficial palmer branch could be an important factor leading to IA injections (Fig. 3). This may be inadvertently cannulated during IV access. Antebrachialissuperficialis dorsalis artery is a branch of the radial artery due to its bifurcation in the forearm, ending as an incomplete palmar arch, on the other hand. Often, it crosses underneath a terminal branch of the cephalic vein, superficial to the radial styloid, which is a common site for IV access. The antecubital fossa and groin are other sites for potential errors. The brachial artery being in close proximity of the median basilic vein can be cannulated unintentionally. Similarly, femoral artery can be cannulated while attempting to gain femoral vein access [1, 2].
Pathophysiology
The understanding of the underlying pathophysiological cascade leading to the sequel of IA injections is clouded. Several theories have been postulated. The common point of all these is an end result of ischemia and necrosis, distal to the site of injection.
Norepinephrine-mediated vasoconstriction theory
Burn and Hobbs hypothesized the role of norepinephrine as a vasoconstrictor leading to ischemia [1]. However, evidence suggests that this is a transient phase, followed by the resumption of normal arterial flow with or without vasodilation [2]. Therefore, its role in the initial stage seems more feasible.
Thrombosis theory
It is reported that red blood cells hemolysis subsequent to an IA injection of drugs such as thiopental, with the release of adenosine diphosphate initiating platelet aggregation that initiates thrombosis [3]. In addition to the role of the medication per se, the catheter itself is responsible for thrombus formation [4]. Prolonged duration of more than 48 h; larger diameter, tapered design, and non-Teflon material of the catheter are identified as causative factors [4].
Crystal theory
Many medications are soluble at alkaline pH higher than the pH of arterial blood and form crystals rapidly after injection [5, 6]. Similar crystallization occurs when drugs such as thiopental and methohexital are mixed into whole blood. The crystals obstruct distal flow and lead to damage to the endothelium because of their chemical properties. However, other studies have provided contrary evidence to the importance of alkaline pH in the pathogenesis [1, 2].
Endothelial inflammation theory
This theory was initially put up by Cohen et al. in 1948 and later on substantiated by other studies [2, 8, 9, 10, 11]. It is based on the role of inflammatory changes in the inner layers of arterial walls causing chemical endarteritis. Further progression of interstitial edema, thrombosis, and damage to the myocytes occurs.
Direct cytotoxicity theory
Cytotoxicity leads to denuding of the vascular endothelium and alters its function of production of vasodilators such as endothelium-derived relaxing factor, which causes vasoconstriction leading to ischemia [12]. Researchers profess that therapeutic strategies that use endothelium-dependent vasodilation to enhance flow in involved arteries would be below par to the modalities that are independent of the integrity of arterial endothelium [12].
Venous constriction theory
Ellertson et al. described that venospasm constricting the arterial wall, and thrombus formation lead to obstruction of blood flow, with eventual stasis culminating in ischemic necrosis [14].
Lipid solubility theory
Knill and Evans reported that different medications that result in ischemia after IA injection are lipid-soluble [15, 16].
High osmolarity theory
Evans et al. suggested that the osmolarity of a solution may be a causative factor for the severe necrosis that occurs after IA injection [16]. The multiplicity of explanations and theories as well as conflicting evidences for the sequelae of IA injections suggests that there still remains a cloud over the conclusive understanding of the pathogenesis. Nevertheless, tentative theories can be established with the available evidence in the literature. Different mechanisms could play individually or in combination with the administration of specific drugs. Some drugs can crystallize, whereas others may be directly toxic to the endothelium. Thrombus formation seems to be the common pathway of all the proposed theories. Understanding the pathogenesis is of paramount importance in procuring therapeutic agents, especially since large prospective human studies are not feasible. In our patient, the risk factors were polytrauma, which itself is a hypercoagulable state and prolonged cannulation. This could have resulted in thrombus formation and subsequent distal flow blockage, leading to ischemic insult.
Treatment
Management of these cases potentially encompasses symptomatic relief to the patient, relief from the arterial spasm, re-percussion to the distal extremity, correction of the injury sequelae, and ischemic features such as necrosis, and gangrene, followed by rehabilitation. We propose the following protocol for the management of a patient with inadvertent IA injection:
Step 1: Continuation of the IA access
We should curb the instinct of removal of the IA catheter when signs of ischemia show up or a suspicion of an inadvertent injection arises. Retaining the catheter has several advantages; aids in determining intravascular pressure or drawing blood for gas analysis, allows immediate local delivery of multiple medications directly to the injured site, and facilitates contrast injection for angiography, directly into the involved vasculature. The initial step should be a slow infusion of the isotonic solution to keep it patent [17].
Step 2: Identify the progress of the disease
Certain clinical indicators correlate with the progress of the disease (Fig. 1b). Assessing the progress can aid in assessing prognosis and stop the patient from developing any unrealistic expectations of improvement. Features such as cyanosis, cool extremity, delayed capillary refill, and sensory deficit can help in determining the progression of the damage [18].
Step 3: Anticoagulants
Heparin is the initial therapeutic intervention in the treatment of IA injections. Since thrombus formation is the common phenomenon in all described pathogenic proposals, heparin must be an early consideration for the treatment. There is no defined protocol available, however similar to the treatment of pulmonary embolism, an initial heparin dosage of 60 IU/kg, followed by adjustment to an international normalized ratio of 2–3, is recommended, with oral anticoagulants [4, 13, 19].
Step 4: Symptomatic relief and rehabilitation
Analgesia, limb elevation, and initiation of passive movement are the mainstay for gradual recovery within realistic estimates. These aid in decreasing edema and reducing compartmental pressures [20, 21, 22].
Step 5: Antibiotics
Empirical antibiotic coverage against Gram-positive organisms and anaerobes can be considered, but the literature is divided about the routine use of antibiotics in such cases [17, 23].
Step 6: Perform specific interventions
A review of literature yields multiple specific interventional agents, however, with no proven guaranteed therapeutic records. These range from noninvasive to procedures requiring skillful efforts with close monitoring;
Local anesthetic agents include procaine and lidocaine, prevent reflex vasospasm [24]. Extremity sympatholysis: Stellate ganglion blocks could also prevent reflex and prolonged vasospasm [22, 25]. Arterial vasodilators: Calcium channel blockers, reserpine, tolazoline, and nicardipine have shown variable efficacy [26, 27, 28]. Thromboxane inhibitors: Thromboxane is an inflammatory mediator implicated in the vasospasm from IA drug injections. Topical Aloe vera and methimazole (specific thromboxane inhibitors) have been evaluated in animal studies. However, aspirin, methylprednisolone, and methimazole all of which limit thromboxane levels, have not shown any statistically significant decrease in tissue necrosis compared with controls [29]. Iloprost (prostacyclin analog) has been successfully used atherosclerotic disease, thromboangiitis obliterans, Raynaud syndrome, and ischemic leg ulcers, as a vasodilator and platelet inhibitor. It has reported efficiency in the management of IA injections [30, 31, 32]. IA Papaverine: Papaverine is an opium alkaloid that facilitates vascular smooth muscle relaxation [33]. However, the inefficacy of IA papaverine has been reported by Jones et al. in cases of IA injections [6]. Other modalities such as selective IA injection of thrombolytics such as urokinase, tissue plasminogen activator, and hyperbaric oxygen have been found to be useful in selective cases [34, 35, 36, 37]. Corticosteroids, as a part of therapeutic regimes for the sequelae of IA injections, have been evaluated – both with and without success [38, 39]. The vast majority of available treatment options are based on anecdotal evidence. Nonetheless, basic treatment options can be derived and put into practice Ultimately, when no medication curbs the ischemic cascade, and gangrene ensues, surgical intervention in the form of amputation becomes a necessity.
Conclusion
In literature, no management guidelines exist for IA injection sequelae. Furthermore, the knowledge of incidence rates, natural history, and pathophysiologic factors resulting in these complications are clouded. For prevention, knowledge of risk factors and typical medications that are generally the culprit should be acquired and propagated among the clinicians and nursing staff. Due vigilance should be maintained, especially in high-risk patients. From a treatment point of view, immediate diagnosis, evaluation of disease progress, control of pain, early, and apt anticoagulation, followed by rehabilitation, are all crucial. In short, we can say that digital ischemia following arterial cannulation in still an unsolved mystery in terms of etiopathogenesis and proper treatment protocol still needs to be established.
Clinical Message
The patients undergoing IA cannulation should be examined multiple times and meticulously to rule out any possibility of digital limb ischemia. Knowledge of risk factors, culprit medications, and immediate diagnosis can be limb saving.
References
1. Burn JH, Hobbs R. Mechanism of arterial spasm following intra-arterial injection of thiopentone. Lancet 1959;1:1112-5.
2. Kinmonth JB, Shepherd RC. Accidental injection of thiopentone into arteries: Studies of pathology and treatment.Br Med J1959;2:914-8.
3. Brown SS, Lyons SM, Dundee JW.Intra-arterial barbiturates. A study of some factors leading to intravascular thrombosis.Br J Anaesth1968;40:13-9.
4. Arquilla B, Gupta R, Gernshiemer J, Fischer M. Acute arterial spasm in an extremity caused by inadvertent intra-arterial injection successfully treated in the emergency department. J Emerg Med 2000;19:139-43.
5. Waters DJ. Intra-arterial thiopental: A physio-chemical phenomenon. Anaesthesia 1966;21:347-56.
6. Jones NC. Inadvertent intra-arterial injection of drugs: Why does it still occur? Br J Intensive Care 1995;5:166-8.
7. Cohen SM. Accidental intra-arterial injection of drugs. Lancet 1948;255:409-17.
8. Engler HS, Freeman RA, Kanavage CB, Ogden LL, Moretz WH. Production of gangrenous extremities by intra-arterial injections. Am Surg 1964;30:602-7.
9. Maxwell TM, Olcott C 4th, Blaisdell FW. Vascular complications of drug abuse. Arch Surg 1972;105:875-82.
10. Ryan JJ, Hoopes JE, Jabaley ME. Drug injection injuries of the hands and forearms in addicts. Plast Reconstr Surg 1974;53:445-51.
11. Dodd TJ, Scott RN, Woodburn KR, Going JJ. Limb ischaemia after intra-arterial injection of temazepam gel: Histology of nine cases. J Clin Pathol 1994;47:512-4.
12. MacPherson RD, McLeod LJ, Grove AJ. Intra-arterial thiopentone is directly toxic to vascular endothelium. Br J Anaesth 1991;67:546-52.
13. Ellertson DG, Lazarus HM, Auerbach R. Patterns of acute vascular injury after intra-arterial barbiturate injection. Am J Surg 1973;126:813-7.
14. Knill RL, Evans D. Pathogenesis of gangrene following intra-arterial injection of drugs: A new hypothesis. Can Anaesth Soc J 1975;22:637-46.
15. Evans JM, Latto IP, Ng WS. Accidental intra-arterial injection of drugs: A hazard of arterial cannulation: 3 case reports. Br J Anaesth 1974;46:463-6.
16. Sujriya S, Eduardo CN, Michael BJ. Complications after unintentional intra-arterial injection of drugs: Risks, outcomes, and management strategies.Mayo Clin Proc 2005;80:783-95.
17. Treiman GS, Yellin AE, Weaver FA, Barlow WE, Treiman RL, Gaspar MR. An effective treatment protocol for intraarterial drug injection. J Vasc Surg 1990;12:456-65.
18. Hyers TM, Agnelli G, Hull RD,Morris TA, Samama M, Tapson V, et al. Antithrombotic therapy for venous thromboembolic disease. Chest 2001;119 Suppl 1:176S-93.
19. Gaspar MR, Hare RR. Gangrene due to intra-arterial injection of drugs by drug addicts. Sugery 1972;72:573-7.
20. Gould JD, Lingam S. Hazards of intra-arterial diazepam. BMJ 1977;2:298-9.
21. Goldberg I, Bahar A, Yosipovitch Z. Gangrene of the upper extremity following intra-arterial injection of drugs: A case report and review of the literature. Clin Orthop 1984;188:223-9.
22. Ghouri AF, Mading W, Prabaker K. Accidental intraarterial drug injections via intravascular catheters placed on the dorsum of the hand. Anesth Analg 2002;95:487-91.
23. Cooper JC, Griffiths AB, Jones RB, Raftery AT. Accidental intra-arterial injection in drug addicts. Eur J Vasc Surg 1992;6:430-3.
24. Tin LN, Elalaoui MY, Akula E. Arterial spasm after administration of diazepam. Br J Anaesth 1994;72:139.
25. Promethazine. Available from: http://www.micromedex.com. [Last accessed on 2018 May 11].
26. Ali AT, Montgomery WD, Santamore WP, Spence PA. Preventing gastroepiploic artery spasm: Papaverine vs calcium channel blockade. J Surg Res 1997;71:41-8.
27. Boudaoud S, Jacob L, Lagneau F, Payen D, Servant JM, Eurin B. Successful treatment of vasospastic acute ischaemia with intra-arterial nicardipine. Eur J Anaesthesiol 1993;10:133-4.
28. Crawford CR, Terranova WA. The role of intraarterial vasodilators in the treatment of inadvertent intraarterial injection injuries. Ann Plast Surg 1990;25:279-82.
29. Zachary LS, Smith DJ Jr., Heggers JP, Robson MC, Boertman JA, Niu XT, et al. The role of thromboxane in experimental inadvertent intra-arterial drug injections. J Hand Surg Am 1987;12:240-5.
30. De Koning YW, Plaisier PW, Tan IL, Lotgering FK. Critical limb ischemia after accidental subcutaneous infusion of sulprostone. Eur J Obstet Gynecol Reprod Biol 1995;61:171-3.
31. Samuel I, Bishop CC, Jamieson CW. Accidental intra-arterial drug injection successfully treated with iloprost. Eur J Vasc Surg 1993;7:93-4.
32. Andreev A, Kavrakov T, Petkov D, Penkov P. Severe acute hand ischemia following an accidental intraarterial drug injection, successfully treated with thrombolysis and intraarterial iloprost infusion: Case report. Angiology 1995;46:963-7.
33. Bittner CH, Zuber M, Eisner L. Acute ischemia of the hand in a drug addict after accidental intra-arterial injection. Swiss Surg 2002;8:281-4.
34. Vangerven M, Delrue G, Brugman E, Cosaert P. A new therapeutic approach to accidental intra-arterial injection of thiopentone. Br J Anaesth 1989;62:98-100.
35. Angel MF, Amiss EC, Amiss LR, Morgan RF. Deleterious effect of urokinase used to treat experimental intra-arterial thiopental injection injuries. Ann Plast Surg 1992;28:281-3.
36. Pratikto TH, Strubel G, Biro F, Kroger K. Intra-arterial injection of dissolved flunitrazepam tablets. Vasa 2004;33:52-4.
37. Adir Y, Halpern P, Nachum Z, Bitterman H. Hyperbaric oxygen therapy for ischaemia of the hand due to intra-arterial injection of methadone and flunitrazepam. Eur J Vasc Surg 1991;5:677-9.
38. Enloe G, Sylvester M, Morris LE. Hazards of intra-arterial injection of hydroxyzine. Can Anaesth Soc J 1969;16:425-8.
39. Taweepoke P, Frame JD. Acute ischaemia of the hand following accidental radial artery infusion of depo-medrone. J Hand Surg Br 1990;15:118-20.
 |
 |
 |
 |
 |
 |
| Dr. Vishal Kumar | Dr. Amit Kumar Salaria | Dr. Prasoon Kumar | Dr. Ekta Dogra | Dr. Gaganpreet Singh | Dr. Sameer Aggarwal |
| How to Cite This Article: Kumar V, Salaria AK, Kumar P, Dogra E, Aggarwal S, Singh G. Digital Ischemia Following Brachial Artery Cannulation in a Polytrauma Patient: A Case-Based Discussion of Etiopathogenesis and Management.. Journal of Orthopaedic Case Reports 2020 Mar-Apr;10(2): 40-45. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com


