
Chronic osteomyelitis of calcaneum is troublesome for surgeons. Simultaneous debridement and local delivery of large dosage of antibiotics through calcium sulphate pellets is a promising single stage treatment modality.
Dr. Mukund Madhav Ojha, Department of Orthopaedic Surgery, All India Institute of Medical Sciences, Raipur, Chhattisgarh, India. E-mail: mukund1203@gmail.com
Background: Calcaneal osteomyelitis is a complicated entity and much more challenging to treat. We present a case of calcaneal osteomyelitis treated with debridement, curettage and filling bone defect with antibiotic mixed calcium sulphate pellets.
Case Report: A female patient presented with pain, swelling and purulent discharge from the left heel. Culture studies and magnetic resonance imaging findings were suggestive of osteomyelitis of the calcaneum. The patient was planned for definitive treatment, and remission was achieved with systemic antibiotics, debridement, curettage, and filling dead space with antibiotic mixed calcium sulphate pellets.
Conclusion: Calcaneal osteomyelitis is very resistant to treatment and results in poor functional outcome. Management of calcaneal osteomyelitis with single-stage strategy using antibiotic mixed calcium sulphate effectively eradicates the disease to attain overall good functional outcome for the patient.
Keywords: Calcaneum, osteomyelitis, debridement, calcium sulphate.
Amongst all the bone infections, calcaneal osteomyelitis accounts for 3–10% [1]. They are very notorious and difficult to eradicate, and with a chronic condition, operative steps are necessary to get away with them [1]. Calcaneal osteomyelitis usually sets in after trauma, post-surgery, or as a complication of the diabetic foot and through hematogenous spread when in children [2]. Overall, Staphylococcus aureus remains the most familiar causative bacteria in all age group [2]. The usual course of management consist of early definitive diagnosis by culture, imaging studies, and blood parameters and treatment in the form of tailored systemic antibiotic coverage, off-loading total contact casting, wound irrigation, debridement, curettage, partial or total calcaneal resection with or without soft tissue coverage, and as per the severity of the disease, may even land up into proximal limb amputation [3]. Nevertheless, whatsoever the treatment is, the main aim is to provide an excellent functional limb as early as possible. We are reporting a case of calcaneal osteomyelitis in a young female treated with wound debridement, curettage and commercially available bone graft substitute (calcium sulphate), which was used as the carrier for local antibiotic dissemination and for dead space management.
A 12-year-old female patient presented to us with the complaint of pain, swelling and purulent discharge from her left heel. She had a history of similar episodes in the near past, for which she underwent incision and drainage elsewhere. She had a swollen red heel with a linear scar on its lateral aspect with pus discharge from the site on examination. Her blood parameters like WBC, ESR and CRP were elevated. A radiograph of the region revealed calcaneal bone destruction and surrounding osteopenia (Fig. 1).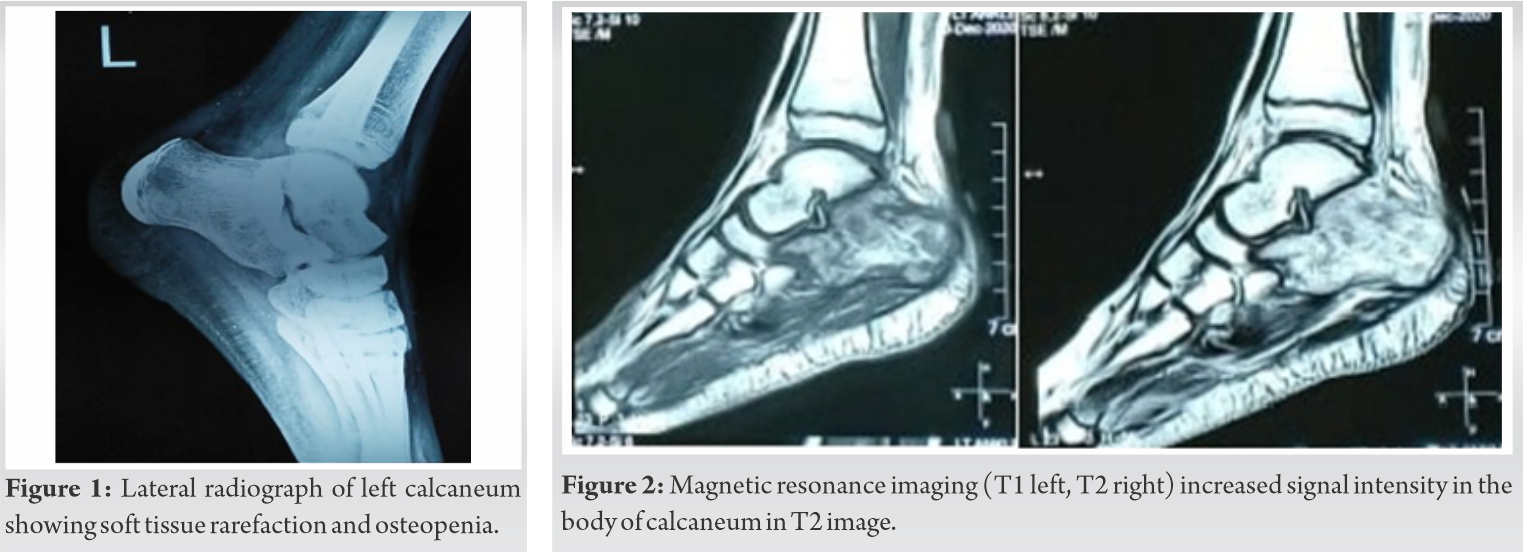 Sinogram tracks the sinus, which was arising from the body of the calcaneum. Magnetic resonance imaging was suggestive of osteomyelitis of the body of calcaneum (Fig. 2). A culture study of the swab, taken from a deeper aspect of the wound, showed the growth of methicillin-resistant S. aureus bacteria. After diagnosing chronic osteomyelitis of calcaneum was confirmed, the patient was planned for a single-stage operative procedure under systemic antibiotic coverage.
Sinogram tracks the sinus, which was arising from the body of the calcaneum. Magnetic resonance imaging was suggestive of osteomyelitis of the body of calcaneum (Fig. 2). A culture study of the swab, taken from a deeper aspect of the wound, showed the growth of methicillin-resistant S. aureus bacteria. After diagnosing chronic osteomyelitis of calcaneum was confirmed, the patient was planned for a single-stage operative procedure under systemic antibiotic coverage.
The calcaneum was approached laterally with an L shaped incision. Thorough debridement was done; the infected bone was curetted out and sent for culture examination (Fig. 3).  We use 10cc of calcium sulphate (STIMULAN®, Biocomposites) [4] as bone defect filler, and for local antibiotic delivery, stimulan® paste was mixed with 1g of vancomycin moulded into multiple pellets through a sterile cast. The bone defect was filled with these pellets (Fig. 4), and the wound was primarily closed, and the limb was supported by below-knee posterior POP (Plaster of Paris) slab. Postoperatively, on day 2, the wound was okay, and there was no discharge, and the radiograph showed the excellent placement of stimulan® (Fig. 5).
We use 10cc of calcium sulphate (STIMULAN®, Biocomposites) [4] as bone defect filler, and for local antibiotic delivery, stimulan® paste was mixed with 1g of vancomycin moulded into multiple pellets through a sterile cast. The bone defect was filled with these pellets (Fig. 4), and the wound was primarily closed, and the limb was supported by below-knee posterior POP (Plaster of Paris) slab. Postoperatively, on day 2, the wound was okay, and there was no discharge, and the radiograph showed the excellent placement of stimulan® (Fig. 5).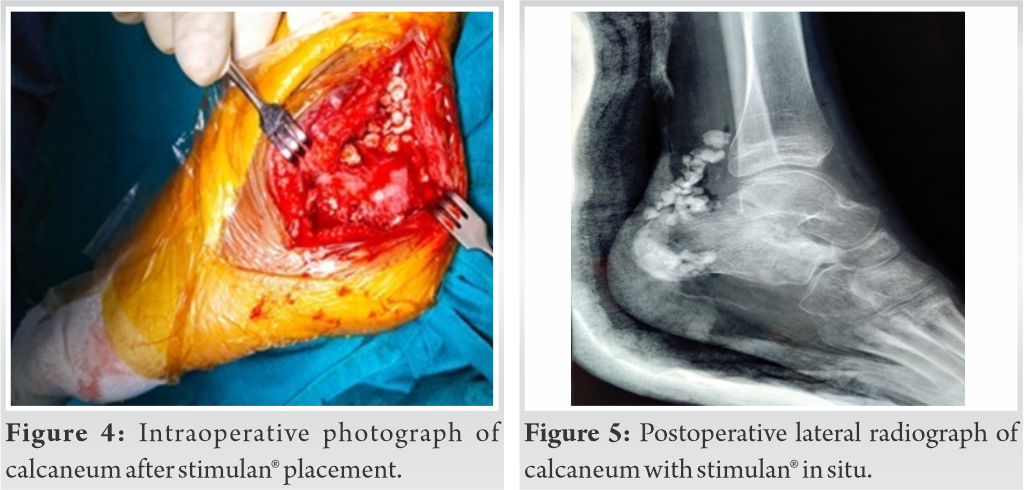 Intravenous antibiotics were continued for 1 week postoperatively. The patient was discharged with slab support and on oral antibiotics and calcium supplements. Post-operatively, after 2 weeks, the wound was healthy, and all sutures were removed.
Intravenous antibiotics were continued for 1 week postoperatively. The patient was discharged with slab support and on oral antibiotics and calcium supplements. Post-operatively, after 2 weeks, the wound was healthy, and all sutures were removed.
The patient was followed up after 1 month, 3 months and 6 months. After 1-month oral antibiotics were discontinued, and she was allowed to do walker assisted partial weight-bearing. Clinically (Fig. 6) and through radiographs (Fig. 7), she showed no signs of recurrence of infection and was utterly allowed to weight bear after 3rd month follow-up. Further, follow-up visits were uneventful.
Osteomyelitis of the calcaneum is tough to cure, and any delay in the management will result in poor functional outcome [1]. Treatment of any osteomyelitis comprises debridement, sequestrectomy and dead space management [2]. Dead space management can be achieved by using bone grafts or their substitutes and flap coverage [2]. PMMA can be used as bone defect filler and for local antibiotic delivery system because of its higher mechanical durability. However, as it is non-biodegradable, it requires second surgery for its removal [5]. Biodegradable substances like calcium sulphate (STIMULAN®, Biocomposites) can be used for the same purpose but are less mechanically robust. In their study on the efficacy of stimulan® antibiotic beads in diabetic foot infection, Chon et al. concluded that usage of stimulan® beads is safe and has a higher healing rate in foot infection [6]. Another study by Papagelopoulos et al. promoted calcium sulphate pellets as an antibiotic delivery system in chronic osteomyelitis of calcaneum because they are safe, readily available and biocompatible [7]. Morley et al. stated that local delivery of antibiotics is good. It reduces systemic overload, reduces kidney and liver toxicity, and bone graft substitutes such as calcium sulphate acts as a sound carrier system for local delivery of antibiotics [8]. Although expensive due to ease in availability, good antibiotic delivery and biodegradability, which allows us to go for a single-stage procedure, we also used calcium sulphate (STIMULAN®, Biocomposites) pellets mixed with antibiotics to eradicate the sepsis from calcaneum and also to fill the bone defect in our case. Only a few case studies of calcaneal osteomyelitis treated with antibiotic mixed calcium sulphate pellets as an adjunct to debridement and curettage were reported in the past. Nevertheless, this case report has demonstrated the efficacy of stimulan® in the effective management of calcaneal osteomyelitis. However, still more case studies will be required for making it a standard modality of treatment.
Calcaneal osteomyelitis comes as an arduous task for surgeons. A meticulous multidisciplinary approach involving orthopaedic and plastic surgeons is usually indicated. Application of stimulan® as bone defect filler and for local antibiotic delivery in calcaneal osteomyelitis is safe and efficient in achieving early remission of the disease in a single-stage surgery with good functional outcome.
Chronic osteomyelitis of calcaneum is troublesome for surgeons. Simultaneous debridement and local delivery of large dosage of antibiotics through calcium sulphate pellets is a promising single stage treatment modality.
References
- 1.Sabater-Martos M, Sigmund IK, Loizou C, McNally M. Surgical treatment and outcomes of calcaneal osteomyelitis in adults: A systematic review. J Bone Jt Infect 2019;4:146-54. [Google Scholar]
- 2.Chen K, Balloch R. Management of calcaneal osteomyelitis. Clin Podiatr Med Surg 2010;27:417-29. [Google Scholar]
- 3.McCann MJ, Wells A. Calcaneal osteomyelitis: Current treatment concepts. Int J Low Extrem Wounds 2020;19:230-5. [Google Scholar]
- 4.Biocomposites. STIMULAN® Biocomposites; 2020. Avaliable from: https://www.biocomposites.com/our-products/stimulan [Google Scholar]
- 5.Kim Y, Inori F, Yamanaka K, Murakami S, Narita E, Yamamura K, et al. A case of osteomyelitis after calcaneal fracture treated by antibiotic-containing calcium phosphate cements. Case Rep Orthop 2018;2018:9321830. [Google Scholar]
- 6.Wai Chon HT, Hamish M, Kirupananthan P, Gmati A, Abdalla H, Hicks R. Stimulan® Antibiotic impregnated beads for the treatment of diabetic foot infection. Arab J Intervent Radiol 2020;4:73-8. [Google Scholar]
- 7.Papagelopoulos PJ, Mavrogenis AF, Tsiodras S, Vlastou C, Giamarellou H, Soucacos PN. Calcium sulphate delivery system with tobramycin for the treatment of chronic calcaneal osteomyelitis. J Int Med Res 2006;34:704-12. [Google Scholar]
- 8.Morley R, Lopez F, Webb F. Calcium sulphate as a drug delivery system in a deep diabetic foot infection. Foot (Edinb) 2016;27:36-40. [Google Scholar]






