
Acromioclavicular joint pseudo-dislocation with lateral end clavicle fracture is a rare injury and can be treated well with our described technique.
Dr. Vivek Dubey, Department of Trauma and Orthopaedics, West Hertfordshire Hospitals NHS Trust, Level 5, PMOK Building, Watford General Hospi-tal, Watford - WD18 0HB, Unites Kingdom. E-mail: vvk7878@gmail.com
Abstract
Introduction: Lateral end clavicle fractures are rare injuries in pediatric and adolescent population. Most of these injuries can be managed conservatively. However, in patients with acromioclavicular joint (ACJ) “pseudo-dislocations” associated with significant clinical deformity, some patients will benefit from operative intervention.
Case Report: Our reported case is a young adolescent with a Type IV Dameron and Rockwood distal clavicle fracture and ACJ pseudo-dislocation, who underwent surgical fixation for this injury. We propose a novel technique of fixation with a suture anchor and endo button with temporary K wire stabilization. These are rare injuries and there are no standardized techniques for reconstruction and fixation. Stabilization with a suture anchor can provide a minimally invasive method of fixation for such injuries without the traditional plating and can lead to excellent final outcomes.
Conclusion: ACJ pseudo-dislocations are rare injuries. There is limited evidence in guiding the management of such injuries. Our proposed technique of fixation with suture anchor, endo button and temporary stabilisation with K-wire can provide promising results.
Keywords: Clavicle fracture, paediatrics, suture anchors, acromioclavicular joint, trauma.
Lateral/acromial end clavicle fractures are rare injuries in the pediatric population, and only account for 10–20% of all clavicular fractures [1,2]. They have been classified by Dameron and Rockwood in a comparable manner to adult acromioclavicular joint (ACJ) injuries, based on the position of the lateral clavicle and injury to the periosteal tube [2,3]. In type III–VI injuries, the mechanism of injury is likened to a “banana-peeling” phenomenon [4]. There is epiphyseal-metaphyseal separation of the distal end of the clavicle, creating a “pseudo-dislocation” at the ACJ [5].
Due to the excellent remodelling potential in skeletally immature patients, it is widely accepted that non- or minimally displaced fractures can be managed conservatively [1,2]. However, there is no clear guidance on the surgical management of more displaced fractures, such as these ACJ “pseudo dislocations.” Literature is limited to a number of case series and reports.
However, consensus appears to be that in paediatric patients nearing skeletal maturity, when significant clinical deformity is present, reduction and fixation of the fracture are recommended [1,2,6]. There is reduced remodelling potential in this population.
We present a case of a young adolescent with an ACJ pseudo dislocation, and propose a novel method of surgical fixation for such injuries.
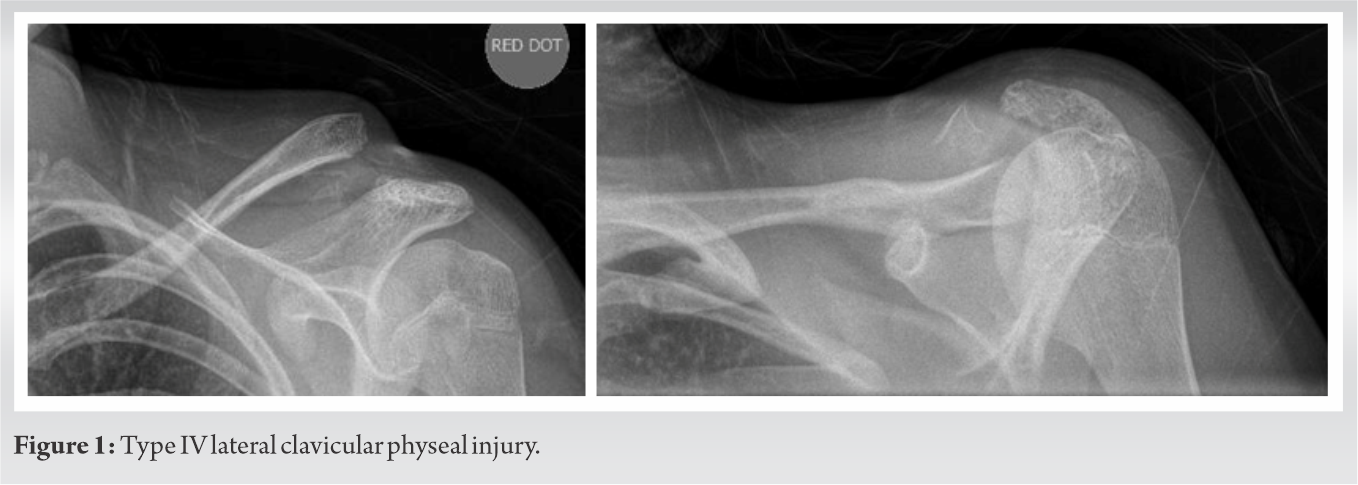
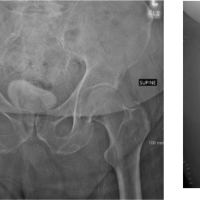
A 14-year-old girl presented to our emergency department following a direct fall onto her left shoulder sustained riding a pushbike. This was an isolated, closed and neurovascularly intact injury. The skin was not threatened. The child presented with swelling and pain around the left shoulder. There was a clear deformity of the clavicle and palpable posterior displacement of the medial fragment. The patient suffered from asthma and no other significant medical co-morbidities and did not take any regular medications. This was her non-dominant hand. Radiographs and a CT scan demonstrated a Dameron and Rockwood Type IV [3] lateral clavicular physeal injury with posterosuperior translation of the metaphyseal fragment (Fig. 1, 2). 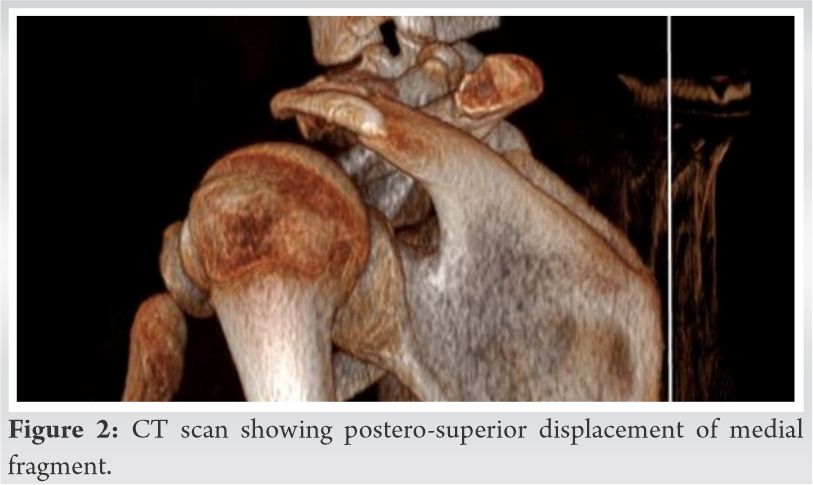
 This is associated with an ACJ pseudo subluxation. After clinical review of the patient and a discussion with the parents about risks and benefits of surgery, the decision was made to proceed with surgical management with informed consent from the child’s parents. These factors which guided us towards specific management were grade of injury, degree of posterior displacement of the proximal fracture fragment and patient’s age. A 14-years-old girl has a lack of superior periosteal cover and limited remodelling potential and hence, she was a candidate for surgical intervention.
This is associated with an ACJ pseudo subluxation. After clinical review of the patient and a discussion with the parents about risks and benefits of surgery, the decision was made to proceed with surgical management with informed consent from the child’s parents. These factors which guided us towards specific management were grade of injury, degree of posterior displacement of the proximal fracture fragment and patient’s age. A 14-years-old girl has a lack of superior periosteal cover and limited remodelling potential and hence, she was a candidate for surgical intervention.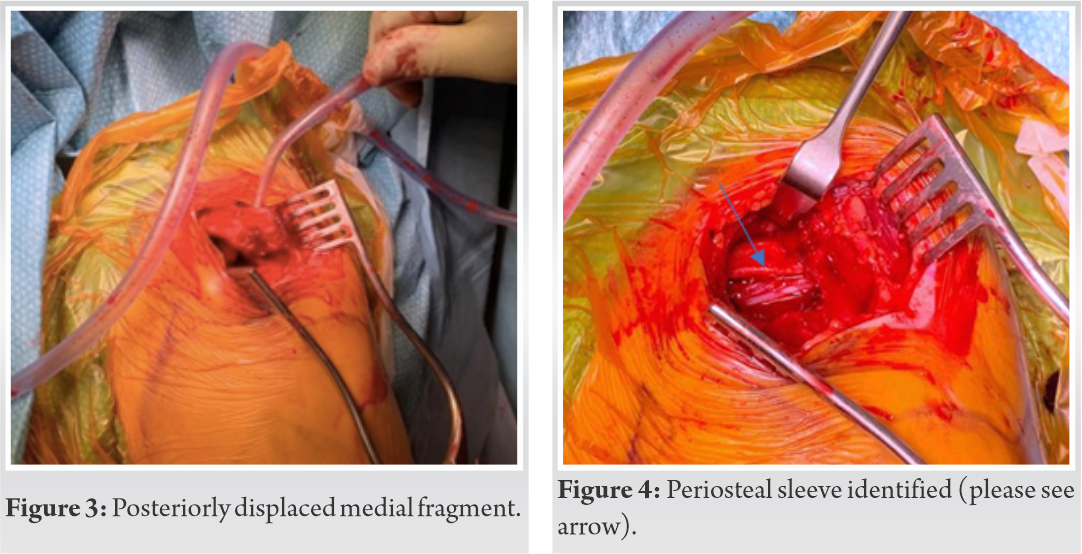
The operation was performed a day after admission. The patient was given general anaesthetic and was placed in beach chair position. Posterior displacement of the proximal fracture fragment was marked out. After prepping and draping, a skin incision over the distal end of the clavicle. Careful soft-tissue dissection was carried out to protect neurovascular structures and protect deltotrapezial fascia for later repair. The posteriorly displaced medial fragment (Fig. 3) was then identified, having buttonholed through the trapezius. As expected, there was no superior periosteal sleeve in a child of this age but, the inferior periosteal sleeve of the clavicle was still attached to the coracoclavicular (CC) joints (Fig. 4). There was also an epiphyseal fragment of the lateral end of the clavicle still in continuity with the ACJ, with the maintained alignment of ACJ.
We elected to use the Acumed (acumed) clavicle plating system for fixation. Due to the patient’s age our plan was to use the Acu-Sinch anchor alone, rather than through the plate as per normally recommended in adults. Prior to reducing the fracture, the coracoid process was exposed. The Acu-Sinch drill was used to drill the near cortex only of the coracoid. One Acu-Sinch anchor was inserted into this drill hole using the Acu-Sinch Driver, to a depth where it was almost flush, under direct visualisation. The sutures were released and the free ends were identified and protected anteriorly. The proximal fragment was then released enough to allow fracture reduction. The reduction was held with 2 × 1.6 mm K wires, directed across the ACJ (Fig. 5).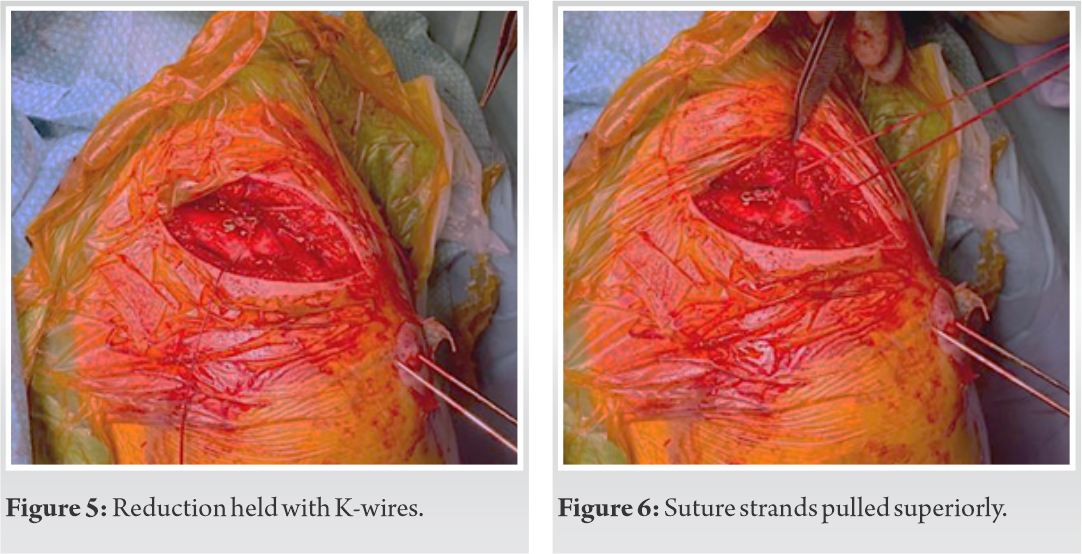 The area in the clavicle directly superior to the suture ends was identified. A 2.8 mm drill was used to drill through both cortices of the clavicle at this point, creating a tract for the suture ends to be passed through. A suture retriever was used to pull both suture strands superiorly from the anchor through the hole in the clavicle. The suture ends are designed to be passed through a suture retainer, which normally sits in the clavicle plate (Fig. 6). We, therefore, decided not to use the retainer as when used alone, it would sit prominently on the superior clavicle and risk causing a stress fracture. Instead, the sutures were tied through and over a 5mm Smith and Nephew EndobuttonTM, ensuring adequate tension and reduction of the fracture site and ACJ. The deltotrapezial fascial flaps were then closed with 2-vicryl to supplement and reinforce the fixation. The arm was placed into a polysling.
The area in the clavicle directly superior to the suture ends was identified. A 2.8 mm drill was used to drill through both cortices of the clavicle at this point, creating a tract for the suture ends to be passed through. A suture retriever was used to pull both suture strands superiorly from the anchor through the hole in the clavicle. The suture ends are designed to be passed through a suture retainer, which normally sits in the clavicle plate (Fig. 6). We, therefore, decided not to use the retainer as when used alone, it would sit prominently on the superior clavicle and risk causing a stress fracture. Instead, the sutures were tied through and over a 5mm Smith and Nephew EndobuttonTM, ensuring adequate tension and reduction of the fracture site and ACJ. The deltotrapezial fascial flaps were then closed with 2-vicryl to supplement and reinforce the fixation. The arm was placed into a polysling.
At 2 weeks, plain radiographs showed a well reduced fracture and anatomical ACJ alignment (Fig. 7). In the first 6 weeks following surgery, the patient was allowed only to mobilise the elbow and wrist. At 6 weeks, the K wires were removed and the patient started rehabilitation, allowing full range of movement as able. At 3 months follow-up, she had a pain free full range of movement, with radiographs showing a well reduced ACJ (Fig. 8). At 5 months, the patient reported no functional limitations and had returned to sporting activities.
In skeletally immature patients, bone is more prone to injury than ligamentous structures [7]. In paediatric acromioclavicular injuries, lateral physeal disruption occurs instead of CC ligament rupture. The CC ligaments remain attached to the periosteal sleeve while the clavicle displaces, creating a “banana-peeling” phenomenon [4]. These are rare injuries as demonstrated by Kubiak and Slongo [8]. They performed a retrospective review of all paediatric clavicle fractures (939 patients) presenting over 20 years to a paediatric teaching hospital. Only 15 patients required operative intervention over this time (1.6%), and only five of these were for lateral clavicle fractures (0.5%) [8]. In our case, given the patient’s age the physis had partially closed, creating a partial intra-articular fracture rather than true lateral physeal separation, an even rarer phenomenon.
There is ongoing controversy surrounding the management of these uncommon injuries as there is little existing literature. Due to the remodelling potential of children, distal clavicle fractures are often managed conservatively with successful outcomes [2,5]. However, there is some consensus in the literature that there are cases in which operative management of these injuries should be considered, particularly Dameron and Rockwood type IV–VI distal clavicle fractures [4,6,9,10]. In patients nearing skeletal maturity, there is limited remodelling potential and these fractures if not managed surgically, can lead to residual deformity of malunion, as reported previously in the literature. Various methods of fixation have been used in the literature including open tension band repair using absorbable sutures [9], temporary Kirschner wire fixation and suture repair of periosteum with [6] or without cerclage fixation around the coracoid process [5,6,8,9,11,12], and coracoid transposition [4]. Reported complications of surgery include K wire migration requiring early removal/revision fixation [5], discomfort, scar dissatisfaction and skin/soft tissue irritation by K wire [8]. However, all patients in these studies treated operatively healed fully and did not have long term clinical deformities or functional deficit.
The authors propose a novel technique of fixation with suture anchors in adolescents following either a displaced distal clavicle fracture or an ACJ injury. This technique involves suture anchor insertion into the coracoid and stabilisation of the clavicle with sutures tied over an EndobuttonTM. Given the age of our patient and associated superior periosteal sleeve deficiency, a suture repair of tissues or isolated K wire fixation would not have been sufficient to maintain integrity and stability of the ACJ long-term; we, therefore, supplemented the repair with CC suture stabilisation. A suture anchor was used in the coracoid as opposed to cerclage fixation to avoid the risk of neurovascular injury, and there is no need for metalwork removal under anaesthetic in the future.
There is a paucity of evidence to guide decision making in paediatric distal clavicle fractures as they are rare injuries. There is a role for operative management in patients with distal clavicle fractures and associated ACJ pseudo-dislocations. We would recommend using a suture anchor and temporary K wires as an effective method of fixation in adolescents, allowing K wire removal at 6 weeks and return to sporting activity by 5 months.
Our proposed technique of fixation and stabilisation of distal clavicle fracture with ACJ “pseudo-dislocations” using suture anchor and endo button can provide good functional out-come in young, adolescent patients.
References
- 1.Wilkins KE, Beaty JH. Rockwood and Wilkins’ Fractures in Children: Lippincott-Raven; 2006. [Google Scholar | PubMed]
- 2.Shah RR, Kinder J, Peelman J, Moen TC, Sarwark J. Paediatric clavicle and acromioclavicular injuries. J Pediatr Orthop 2010;30:S69-72. [Google Scholar | PubMed]
- 3.Rockwood C. Fractures of the outer clavicle in children and adults. J Bone Joint Surg Br 1982;64:642. [Google Scholar | PubMed]
- 4.Falstie-Jensen S, Mikkelsen P. Pseudodislocation of the acromioclavicular joint. J Bone Joint Surg Br 1982;64:368-9. [Google Scholar | PubMed]
- 5.Black GB, McPherson JA, Reed MH. Traumatic pseudodislocation of the acromi-oclavicular joint in children. A fifteen year review. Am J Sports Med 1991;19:644-6. [Google Scholar | PubMed]
- 6.Kotb A, Yong T, Abdelgawad A. A posteriorly displaced distal metaphyseal cla-vicular fracture (Type IV AC joint dislocation-like) in children: A case report and literature review study. Case Rep Orthop 2016;2016:4015212. [Google Scholar | PubMed]
- 7.Delgado J, Jaramillo D, Chauvin NA. Imaging the injured pediatric athlete: Upper extremity. Radiographics 2016;36:1672-87. [Google Scholar | PubMed]
- 8.Kubiak R, Slongo T. Operative treatment of clavicle fractures in children: A re-view of 21 years. J Pediatr Orthop 2002;22:736-9. [Google Scholar | PubMed]
- 9.Rashid A, Christofi T, Thomas M. Surgical treatment of physeal injuries of the lateral aspect of the clavicle: A case series. Bone Joint J 2013;95:664-7. [Google Scholar | PubMed]
- 10.Ogden JA. Distal clavicular physeal injury. Clin Orthop Relat Res 1984;188:68-73. [Google Scholar | PubMed]
- 11.Havránek P. Injuries of distal clavicular physis in children. J Pediatr Orthop 1989;9:213-5. [Google Scholar | PubMed]
- 12.Labronici PJ, da Silva RR Jr., Franco MV, Labronici GJ, Pires RE, Franco JS. Fratura da região distal da clavícula em crianças. Rev Bras Ortop 2016;51:24-8. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 March 10, 2024 Culture Negative Pasteurella multocida Confirmed Prosthetic Hip Infection using Next-generation Sequencing
March 10, 2024 Culture Negative Pasteurella multocida Confirmed Prosthetic Hip Infection using Next-generation Sequencing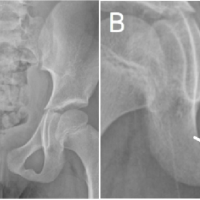 March 10, 2024 Van Neck-Odelberg Disease: A Rare Cause of Pediatric Hip Pain
March 10, 2024 Van Neck-Odelberg Disease: A Rare Cause of Pediatric Hip Pain March 10, 2018 Why do we lack a research culture? Analyzing the Indian Medical landscape – Response
March 10, 2018 Why do we lack a research culture? Analyzing the Indian Medical landscape – Response November 10, 2019 Resurgence of Conservative treatment
November 10, 2019 Resurgence of Conservative treatment