
Dual-energy computed tomography is non-invasive and can help to make a correct diagnosis in atypical gout and gouty tophi such as without hyperuricemia.
Dr. Tadashi Kimura, Department of Orthopaedic Surgery, The Jikei University School of Medicine, Minato, Tokyo, Japan. E-mail: tadashi-kimura@jikei.ac.jp
Abstract
Introduction: Gouty tophi are relatively simple to diagnose because they almost always occur in patients with persistent hyperuricemia. Treatment typically consists mainly of oral medication, and surgical intervention is necessary for only a small number of patients.
Case Presentation: We present a case of 66-year-old Japanese man presented with a painful gouty tophus diagnosed by dual-energy computed tomography in the right foot without hyperuricemia that had gradually increased in size over the past 20 years. The tophus was removed and the patient’s plantar pain disappeared after surgery and there was no recurrence.
Conclusion: We obtained a favorable outcome through surgical intervention for a gouty tophus of the foot diagnosed by dual-energy computed tomography in a patient without hyperuricemia. Our experience suggests that proactive surgical removal of gouty tophi should be considered for symptomatic cases and to prevent further joint destruction.
Keywords: Dual-energy computed tomography, foot, gouty tophus.
Acute gout attacks are triggered by an inflammatory response caused by excessive pooling of uric acid and local deposition of monosodium urate crystals in a person with hyperuricemia. Attacks first manifest as acute intermittent gout, or acute attacks that resolve spontaneously and then recur repeatedly. Over the long term, persistent hyperuricemia causes acute attacks to become increasingly more frequent and severe, ultimately resulting in chronic arthritis and formation of palpable gouty tophi. Many patients with hyperuricemia are successfully treated with oral medication and lifestyle modification alone, and few develop gouty tophi. Even fewer require surgical intervention [1]. Here, we report a case of gouty tophus in the foot of a patient without hyperuricemia, which we diagnosed by dual-energy computed tomography (DECT) and treated surgically.
A 66-year-old Japanese man presented with a painful plantar mass in the right foot that had gradually increased in size over the past 20 years. The mass was at the level of the plantar metatarsophalangeal (MTP) joints on the right fourth metatarsal head and had a maximum diameter of approximately 30 mm (Fig. 1a). There was no redness or heat. Hematological investigations were normal and included a uric acid level of 6.5 mg/dl (normal range, 3.0–7.0 mg/dl). Magnetic resonance imaging revealed a soft tissue mass extending from just below the fourth MTP joint. T1-weighted (Fig. 1b), T2-weighted (Fig. 1c), and short tau inversion recovery (Fig. 1d) images showed heterogeneous low signal inside the septum and bone erosion around the second, third, and fourth MTP joints.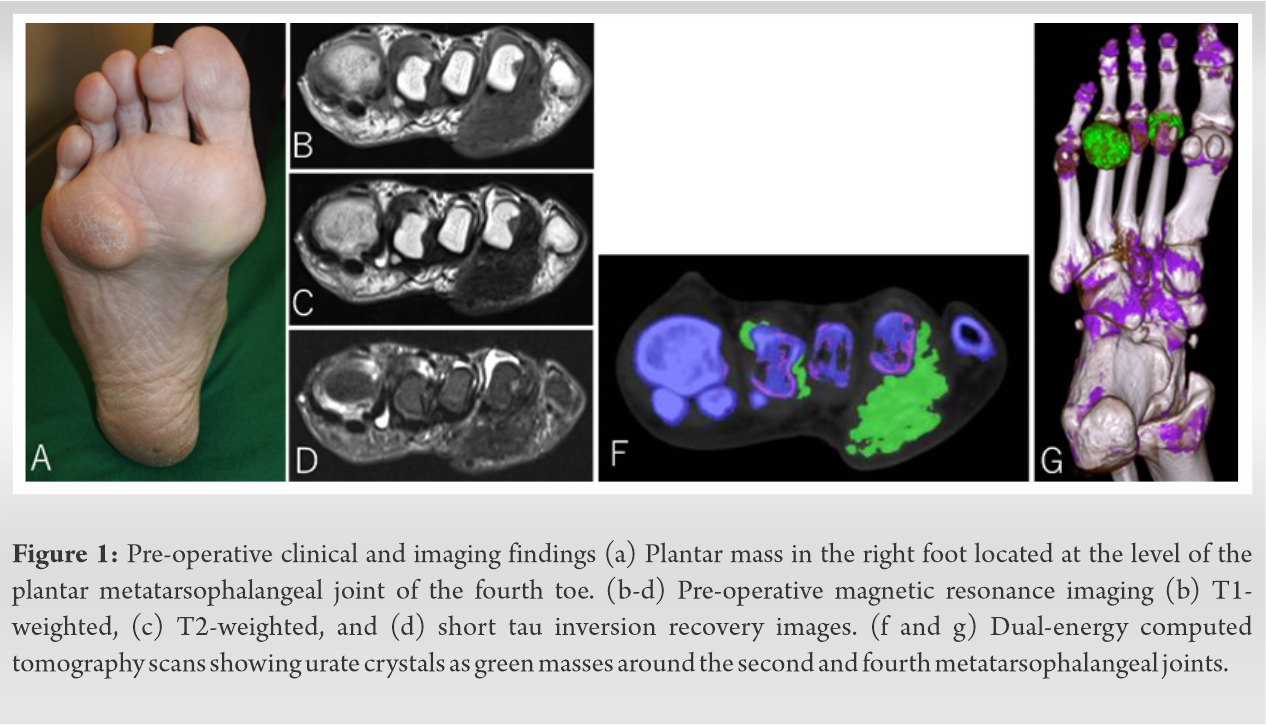 The differential diagnoses were amyloidosis, gouty tophus, and fibromatosis. We then performed DECT, which enables differentiation of urate crystals from calcium-containing mineralization. The patient was scanned with a SOMATOM Drive CT system (Siemens Healthineers, Forchheim, Germany) in DE mode. Two-material decomposition analysis was performed using a commercial workstation (Syngo; Siemens Healthineers). A monosodium urate image was created. Urate crystals were clearly visualized by DECT as green masses around the second, third, and fourth MTP joints (Fig. 1f and g). Therefore, the mass was diagnosed as gouty tophus. Due to weight-bearing pain around the fourth MTP joint, we performed resection of the mass. The mass was located directly under the skin and entrapped in the flexor tendon of the fourth toe (Fig. 2a). The mass was removed and found to contain chalk-like deposits (Fig. 2b). The histopathological findings were consistent with gout. The patient’s plantar pain disappeared after surgery and there was no recurrence. Post-operative DECT showed that most of the gouty tophus around the fourth MTP joint was removed (Fig. 2c and d).
The differential diagnoses were amyloidosis, gouty tophus, and fibromatosis. We then performed DECT, which enables differentiation of urate crystals from calcium-containing mineralization. The patient was scanned with a SOMATOM Drive CT system (Siemens Healthineers, Forchheim, Germany) in DE mode. Two-material decomposition analysis was performed using a commercial workstation (Syngo; Siemens Healthineers). A monosodium urate image was created. Urate crystals were clearly visualized by DECT as green masses around the second, third, and fourth MTP joints (Fig. 1f and g). Therefore, the mass was diagnosed as gouty tophus. Due to weight-bearing pain around the fourth MTP joint, we performed resection of the mass. The mass was located directly under the skin and entrapped in the flexor tendon of the fourth toe (Fig. 2a). The mass was removed and found to contain chalk-like deposits (Fig. 2b). The histopathological findings were consistent with gout. The patient’s plantar pain disappeared after surgery and there was no recurrence. Post-operative DECT showed that most of the gouty tophus around the fourth MTP joint was removed (Fig. 2c and d).
Gout is a type of crystal-induced arthritis and is usually diagnosed based on peripheral joint swelling and redness [2]. However, there are unusual presentations (e.g., an atypical site, polyarticular involvement, or an indolent course) that can make the diagnosis challenging [3]. Gouty tophi are reported to be common in patients with a serum urate level of >8.5 mg/dl for more than >10 years [4]. However, our patient had never been diagnosed with hyperuricemia or an attack of gout.
Because our patient did not have hyperuricemia, we were not confident that the mass we observed on magnetic resonance imaging was a gouty tophus. That is why we used DECT. This imaging modality obtains two exposures at different energy levels, which allows material decomposition and acquisition of virtual monochromatic images [5]. The discriminated materials can be color-coded and overlaid onto CT images to aid diagnosis and localization of a lesion. DECT can reveal gout by displaying monosodium urate deposition regardless of site and phase of disease. Therefore, DECT is a suitable method for making a diagnosis with confidence and without aspiration or biopsy. It was added in the 2015 Gout Classification Criteria published by the American College of Rheumatology-European League against Rheumatism [6]. DECT also enables visualization of the therapeutic effect of both surgical and conservative treatment [7]. Although few institutions are capable of DECT at this time, it will likely become more widespread in the future.
Treatment for gouty tophi typically consists of pharmacotherapy with antihyperuricemic agents, and surgery is rarely performed nowadays. However, surgical intervention is necessary in certain circumstances, for example, when a fistula has formed, the tophus is very painful, or the tophus is in a tendon or bone [1]. Our patient’s QOL had been negatively affected by pain, and improved significantly after surgery. Based on this experience, we believe that proactive surgical removal of gouty tophi should be considered for symptomatic cases and to prevent further joint destruction.
We obtained a favorable outcome through surgical intervention for a gouty tophus of the foot diagnosed by DECT in a patient without hyperuricemia.
DECT is non-invasive and can help to make a correct diagnosis in atypical gout and gouty tophi such as without hyperuricemia. Clinicians should consider performing DECT before invasive examination if a patient is suspected to have gouty tophi or another gout-related problem. Clinicians should also consider surgical treatment when pain or other symptoms are affecting the patient’s QOL.
References
- 1.Chhana A, Dalbeth N. The gouty tophus: A review. Curr Rheumatol Rep 2015;17:19. [Google Scholar | PubMed]
- 2.Hainer BL, Matheson E, Wilkes RT. Diagnosis, treatment, and prevention of gout. Am Fam Physician 2014;90:831-6. [Google Scholar | PubMed]
- 3.Ning TC, Keenan RT. Unusual clinical presentations of gout. Curr Opin Rheumatol 2010;22:181-7. [Google Scholar | PubMed]
- 4.Gutman AB. The past four decades of progress in the knowledge of gout, with an assessment of the present status. Arthritis Rheum 1973;16:431-45. [Google Scholar | PubMed]
- 5.Fukuda T, Fukuda K. The role of dual-energy computed tomography in musculoskeletal imaging. PET Clin 2018;13:567-78. [Google Scholar | PubMed]
- 6.Neogi T, Jansen TL, Dalbeth N, Fransen J, Schumacher HR, Berendsen D, et al. 2015 Gout classification criteria: An American college of rheumatology/European league against rheumatism collaborative initiative. Arthritis Rheumatol 2015;67:2557-68. [Google Scholar | PubMed]
- 7.Maeda K, Chino H, Tokashiki T, Udaka J, Okutsu Y, Yukawa M, et al. A case of carpal tunnel syndrome caused by giant gouty tophi: The usefulness of DECT for the diagnosis, preoperative planning and postoperative evaluation of atypical cases. Mod Rheumatol Case Rep 2019;3:165-71. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 January 10, 2020 Complete Extra-articular Ankylosis of Hip and Stiff Elbow in a Case of Extensive Myositis Ossificans: A Rare Presentation
January 10, 2020 Complete Extra-articular Ankylosis of Hip and Stiff Elbow in a Case of Extensive Myositis Ossificans: A Rare Presentation December 10, 2022 Digital Arterial Occlusion at the Metacarpophalangeal Joint with Hypothenar Hammer Syndrome-like Symptoms: A Case Report
December 10, 2022 Digital Arterial Occlusion at the Metacarpophalangeal Joint with Hypothenar Hammer Syndrome-like Symptoms: A Case Report November 1, 2025 Irreducible Dislocation of the Great Toe Interphalangeal Joint Secondary to an Incarcerated Sesamoid: A Retrospective Case Series of Six Patients
November 1, 2025 Irreducible Dislocation of the Great Toe Interphalangeal Joint Secondary to an Incarcerated Sesamoid: A Retrospective Case Series of Six Patients October 10, 2023 Recurrent Abdominal Aggressive Fibromatosis with Incapacitating Hip Contracture – A Case Report
October 10, 2023 Recurrent Abdominal Aggressive Fibromatosis with Incapacitating Hip Contracture – A Case Report