
Pain in the ankle is rarely due to malignancies. Malignancies such as chondrosarcoma behave very differently in the hand and foot bones. The differential diagnosis of chronic pain should always include malignancy.
Dr. Rishikesh Tupe, Department of Orthopedics, Byramjee Jeejeebhoy Government Medical College and Sassoon General Hospital, Pune, Maharashtra, India. E-mail: rishi8contact@gmail.com
Abstract
Introduction: Chondrosarcoma of the talus is one of the rare causes of ankle pain. Often this pain is neglected by the patients. Hence, the presentation is late. A rare occurrence, lack of clinical familiarity, and resemblance to enchondroma make the diagnosis of chondrosarcoma difficult.
Case Report: We present a case of chondrosarcoma of talus in a 42-year-old female, which is an uncommon site of occurrence. In the presence of non-classical radiologic and histologic findings, the patient was treated with below-knee amputation. At present, the patient is disease-free and walking with a prosthesis.
Conclusion: Talus is an infrequent site for chondrosarcoma. When affected, it presents as vague ankle pain. A patient can be underdiagnosed as there are no clear radiological and histological guidelines to differentiate between benign and low-grade cartilaginous tumors such as enchondroma and low-grade chondrosarcoma. Histologically proven benign lesions must be followed for a long time in suspicion of malignancy. The treatment of chondrosarcoma of the talus can vary from local wide excision to below-knee amputation, depending on the grade of malignancy.
Keywords: Chondrosarcoma, cartilaginous tumor, talus, enchondroma, below-knee amputation.
Chondrosarcoma is a malignant tumor of bone that produces a cartilaginous matrix. It is commonly seen in long tubular bones of the lower limb and upper limb as well as in the pelvis [1]. In the lower limb, the femur is the most common site, whereas the proximal humerus is most commonly involved in the upper limb [1]. The foot is an infrequent site for the occurrence of chondrosarcoma, with an incidence of around 1.5% to 2.97% of all cases of chondrosarcoma [2,3,4]. Involvement of metatarsals, calcaneum, and proximal phalanx are relatively common as compared to talus [4]. No more than eight cases of chondrosarcoma of the talus have b een reported in the medical literature [5,6,7]. In one of the largest studies by Murari et al. [8] with 255 cases of primary bone tumors of the foot, no case of chondrosarcoma of the talus was reported. On review of the Scottish Bone Tumor Registry between 1954 and 2010, only two cases of talar chondrosarcoma were discovered [9]. Frequently, chondrosarcoma around the ankle joint presents as a painful or painless swelling. At times, ankle pain may be the only presenting complaint. Many patients present late and often these tumors are misdiagnosed as soft tissue injuries. A high index of suspicion for the tumor is required in the absence of trauma or persistent symptoms [9]. Radiology and histology may not always confidently differentiate between enchondroma and low-grade chondrosarcoma. Not only diagnosing these tumors can be a challenge but also choosing optimal treatment could be tricky. Clinical judgment, the experience of the surgeon, and multidisciplinary teamwork play a crucial role in managing such tumors.
Overall, low-grade chondrosarcoma needs extensive research to build clear guidelines for its diagnosis and management. Few immunohistochemical markers such as S100 protein and CD 99 are useful to detect chondrosarcoma, but they are positive only in mesenchymal variety and not very specific for other types of chondrosarcoma [7]. Thus, it also provides a research opportunity to refine the molecular diagnosis of chondrosarcoma.
A 42-year-old housewife came to the orthopedic outpatient department with complaints of insidious onset dull pain and mild generalized ankle swelling in the right ankle for 2 years. On examination, there were no skin changes over the swelling and ankle range of motion was complete without any pain. She was given treatment in the-form of analgesics which failed to relieve her symptoms. She was referred for further evaluation to our center. Radiographic examination showed a lytic lesion in the talus with a narrow transition zone and irregular calcifications at the center (Figs. 1a and b).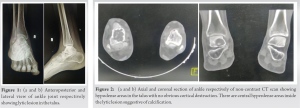 A computed tomography scan without contrast (NCCT) was performed which revealed a 4.2 × 3 × 2.3 cm [AP × ML × SI] hypodense lesion involving almost the entire talus with hyperdense calcific foci noted within it. No obvious cortical destruction was noted (Fig. 2a and b). A magnetic resonance imaging (MRI) of the patient was suggestive of neoplastic etiology possibly enchondroma or low-grade chondrosarcoma (Fig. 3-5). The patient was advised biopsy to rule out malignancy. Biopsy was taken under an image intensifier by J-needle (Fig. 6). On histopathological examination, chondrocytes did not show nuclear atypia hypercellularity or pleomorphism suggestive of a benign pathology such as enchondroma (Fig. 7). A tentative diagnosis of the benign chondroid tumor was made, and the patient was followed up on an outpatient basis. Two months later, the patient was complaining increase in the intensity of ankle pain. In suspicion of malignancy, the patient was referred to an oncologist. A repeat biopsy was performed which showed a moderately cellular tumor arranged in lobules of an extracellular hyaline cartilaginous matrix with focal myxoid degeneration and atypical chondrocytes embedded in it (Fig. 8). Findings were suggestive of grade 2 conventional chondrosarcoma. Metastatic work up for patient was done. Chest radiograph was normal.
A computed tomography scan without contrast (NCCT) was performed which revealed a 4.2 × 3 × 2.3 cm [AP × ML × SI] hypodense lesion involving almost the entire talus with hyperdense calcific foci noted within it. No obvious cortical destruction was noted (Fig. 2a and b). A magnetic resonance imaging (MRI) of the patient was suggestive of neoplastic etiology possibly enchondroma or low-grade chondrosarcoma (Fig. 3-5). The patient was advised biopsy to rule out malignancy. Biopsy was taken under an image intensifier by J-needle (Fig. 6). On histopathological examination, chondrocytes did not show nuclear atypia hypercellularity or pleomorphism suggestive of a benign pathology such as enchondroma (Fig. 7). A tentative diagnosis of the benign chondroid tumor was made, and the patient was followed up on an outpatient basis. Two months later, the patient was complaining increase in the intensity of ankle pain. In suspicion of malignancy, the patient was referred to an oncologist. A repeat biopsy was performed which showed a moderately cellular tumor arranged in lobules of an extracellular hyaline cartilaginous matrix with focal myxoid degeneration and atypical chondrocytes embedded in it (Fig. 8). Findings were suggestive of grade 2 conventional chondrosarcoma. Metastatic work up for patient was done. Chest radiograph was normal.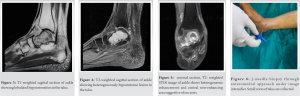 Furthermore, FDG-PET scan revealed a lytic low-grade metabolically active lesion with the chondroid type of calcification in the talus. There was no metabolically active disease elsewhere in the body. The presumptive diagnosis of chondrosarcoma of the talus was made and the patient was explained about the disease and its progression. All possible treatment options were explained to her. The patient opted for below-knee amputation due to the high possibility of recurrence of the tumor. The amputation stump was sent for histopathology which confirmed grade 2 conventional chondrosarcoma. The post-operative course was uneventful. She is walking with below knee prosthesis without support. A 1-year follow-up examination and radiological imaging revealed no evidence of metastasis.
Furthermore, FDG-PET scan revealed a lytic low-grade metabolically active lesion with the chondroid type of calcification in the talus. There was no metabolically active disease elsewhere in the body. The presumptive diagnosis of chondrosarcoma of the talus was made and the patient was explained about the disease and its progression. All possible treatment options were explained to her. The patient opted for below-knee amputation due to the high possibility of recurrence of the tumor. The amputation stump was sent for histopathology which confirmed grade 2 conventional chondrosarcoma. The post-operative course was uneventful. She is walking with below knee prosthesis without support. A 1-year follow-up examination and radiological imaging revealed no evidence of metastasis.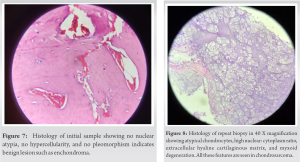
Chondrosarcoma commonly presents in the 4th and 5th decades with male predilection (2:1) [1]. The most common symptom is pain, occurring in almost 95% of the cases. Pain is insidious in onset, progressive over the time, and worst at the night and has been present for months to years before presentation [1]. In some patients, pain is associated with soft-tissue swelling. Few patients report pathological fractures as an initial presentation when chondrosarcoma involves typically a long bone. A sudden increase in pain indicates aggressiveness or conversion to malignancy. As ankle pain is rarely caused by malignancy, these tumors are neglected and commonly treated as soft-tissue injuries. Young et al. [9] reported that 14 patients with talar tumors were initially misdiagnosed with an ankle sprain (9), ganglion (2), and rheumatological or soft-tissue injury (3). Chondrosarcoma is 3rd most common tumor of the bone [1]. The axial skeleton is commonly involved in chondrosarcoma. Murari et al. [8] reported chondrosarcoma as the most common tumor of the foot with metatarsal being most commonly involved bone [8]. Talus was a very rare site of occurrence for malignant tumors [4,8,9]. If present in the talus, cartilaginous tumors are typically well recognized on radiographs. However, differentiation between benign (enchondroma) and malignant (low-grade chondrosarcoma) is very difficult and is a radiologic and histologic challenge [10]. As the treatment for benign lesions requires only follow-up and malignant need surgical intervention, these tumors must be addressed cautiously. Not just tumor heterogenicity but also the sampling errors make the histological identification of low-grade chondrosarcoma more complicated [10]. Few studies described “Secondary chondrosarcoma” as a rare entity that arises in benign lesions such as enchondromas, osteochondroma, synovial chondromatosis, fibrous dysplasia, and radiation therapy [11], which again increases the diagnostic difficulties. Levent buluc [5] presented a case of chondrosarcoma of talus that arouse from a pre-existing enchondroma and has emphasized regular follow-up of benign cartilaginous tumor of bone for early detection of secondary chondrosarcoma. In our case, we have faced similar problems. Computer tomography (CT) and MRI findings were not very classic to label it as a malignant tumor. The initial biopsy sample did not show any histological findings of malignancy, but the repeat biopsy had features of low-grade chondrosarcoma. This may raise suspicion of the development of secondary chondrosarcoma in pre-existing enchondroma. In our case, for this diagnosis 2 months were a very acute duration for the development of such a condition. Hence, sampling error thought to be contributing factor to secondary chondrosarcoma. But still, the possibility of secondary chondrosarcoma cannot be fully ruled out. Typical radiologic features of chondrosarcoma are present in long bones. Hence, differentiating benign and low-grade chondrosarcoma is relatively easier in long bones than in foot and hand bones [1]. Typical radiology of chondrosarcoma shows lobulated, lytic, and sclerotic lesions. The characteristic appearance of the “Ring and arc pattern” of calcification is seen [12]. These tumors grow in lobular architecture and cause endosteal scalloping that may result in cortical penetration and soft-tissue extension. Tumor size of more than 4 cm in its maximum diameter, broad cortical scalloping, destruction of the cortex, characteristic ring and arc calcification, and soft-tissue extension point toward chondrosarcoma are the findings which will help in deciding the diagnosis of chondrosarcoma [5]. Brien et al. showed that there is a positive correlation between tumor size and malignant propensity [13]. Depth of endosteal scalloping is the single most important feature distinguishing enchondroma and chondrosarcoma of long bones. However, this feature is not typically seen in long tubular bones of hands and feet, as enchondroma can also cause endosteal scalloping in these bones. Cortical penetration and extension to soft tissue is a relatively reliable feature in small bones of hands and feet [2,14]. High grades of chondrosarcoma (grade 3) show a more aggressive pattern of bone lysis and are called “Moth-eaten” appearance [1] on a radiograph. A CT scan is helpful in the detection of cortical permeation and curvilinear pattern of matrix mineralization. Although the matrix mineralization and endosteal scalloping are best depicted on CT scan, these features are not promising to differentiate between enchondroma and low-grade chondrosarcoma [15]. MRI provides the extent of marrow and soft-tissue involvement. Demonstration of soft- tissue extension with mass formation excludes the diagnosis of enchondroma [1]. MRI- STIR (Short T1 Inversion Recovery) images are very useful to detect increased marrow or soft-tissue signals. Histopathology is the gold standard for the detection of many tumors. However, intermediate tumors such as low-grade chondrosarcoma are very difficult to identify on histology especially, in small bones of hands and feet. Typical histology of chondrosarcoma shows atypical chondrocytes, hypercellularity, nuclear hyperchromasia, pleomorphism, and high nuclear: Cytoplasm ratio, increased mitosis, myxoid degeneration, and peripheral spindling. Typical histology of enchondroma shows nodules of cartilage separated by marrow fat that this pattern is called “benign islands of cartilage” pattern. Second, enchondroma typically shows an “encasement pattern” that is the partial or complete encasement of the tumor by plates of lamellar bone [13]. However, However, at some location such as foot this histologic criteria is not well defined and greater cellularity and atypia is allowed for enchondroma and cannot be differentiated from low-grade chondrosarcoma Despite its greater cellularity and atypia, enchondroma of the foot bone is not considered malignant. This characteristic makes the distinction between enchondroma and low-grade chondrosarcoma difficult. [16,17]. Few lesions will demonstrate a mixture of low-grade chondrosarcoma and enchondroma. Biopsy from the benign part may lead to sampling error; hence, differentiation of low-grade chondrosarcoma from enchondroma becomes challenging [13]. Stoker DJ, in his article on needle biopsy of musculoskeletal lesions, mentioned that a single biopsy is advisable as the rate of local recurrence and metastasis increases when more than one biopsy is performed [18]. To improve the accuracy of biopsy and reduce sampling error, mapped MR imaging-guided tissue biopsy is recommended [10]. The incidence of malignant transformation of enchondroma in small bones of hands and feet is around 1% [13]. Low-grade chondrosarcoma is a locally aggressive tumor. Recurrence and metastasis are not uncommon in chondrosarcoma of foot bones specially calcaneus and talus. Chemotherapy and radiotherapy are generally ineffective against chondrosarcoma. Hence, aggressive treatment such as below-knee amputation is required for chondrosarcoma of these bones [19]. Young et al. [9] stated that out of 5 low-grade chondrosarcomas of calcaneum 3 were subjected to intralesional curettage with adjuvant, 1 wide local excision, and 1 below knee amputation. Out of three intralesional curettage groups, two patients underwent below knee amputation due to local recurrence. His study included two talus chondrosarcoma and both of them underwent below knee amputation. After 7 years, one patient was disease free and another died due to pulmonary metastasis. All patients with calcaneal chondrosarcoma were dead. In our case, the patient opted for a below-knee amputation. After 1 year of follow-up, the patient is not having any signs of metastasis and walking with prosthesis.
The chondrosarcoma of the talus is a rare malignant tumor. It presents as pain in the ankle and is sometimes associated with swelling. As these symptoms are very vague, most of the time these tumors are misdiagnosed as an ankle sprain and easily neglected. After radiologic diagnosis, the battle does not end. As enchondroma and low-grade chondrosarcoma share many common CT and MRI findings. The task becomes more difficult in bones of hand and feet as a histologic diagnosis also becomes a challenge. Hence, correctly stated by Brien “The importance of always keeping in mind the possibility of chondrosarcoma when taking a biopsy of an enchondroma, no matter how innocent it may appear to all concerned” [13].
Ankle pain of long duration should not be ignored. Always keep simple causes of ankle pain as your first diagnosis but always remember to keep rare causes of ankle pain in mind.
References
- 1.Murphey MD, Walker EA, Wilson AJ, Kransdorf MJ, Temple HT, Gannon FH. From the archives of the AFIP: Imaging of primary chondrosarcoma: Radiologic-pathologic correlation. Radiographics 2003;23:1245-78. [Google Scholar | PubMed]
- 2.Nigrisoli M, Ferraro A, De Cristofaro R, Picci P. Chondrosarcoma of the hand and foot. Chir Organi Mov 1990;75:315-23. [Google Scholar | PubMed]
- 3.Ogose A, Unni KK, Swee RG, May GK, Rowland CM, Sim FH. Chondrosarcoma of small bones of the hands and feet. Cancer 1997;80:50-9. [Google Scholar | PubMed]
- 4.Patil S, de Silva MV, Crossan J, Reid R. Chondrosarcoma of the bones of the feet. J Foot Ankle Surg 2003;42:290-5. [Google Scholar | PubMed]
- 5.Buluç L, Arslan A, Müezzinoglu B, Yildiz DK, Sarlak AY. Chondrosarcoma of the talus: A case report. J Foot Ankle Surg 2005;44:292-6. [Google Scholar | PubMed]
- 6.Bell SW, Young PS, Mahendra A. Primary bone tumours of the talus: The Scottish Bone Tumour Registry experience. Foot Ankle Surg 2012;18:277-82. [Google Scholar | PubMed]
- 7.Zhao F, Fan S, Qin A, Jin G. Mesenchymal chondrosarcoma of the talus: A case report. Foot Ankle Int 2007;28:1095-9. [Google Scholar | PubMed]
- 8.Murari TM, Callaghan JJ, Berrey BH Jr., Sweet DE. Primary benign and malignant osseous neoplasms of the foot. Foot Ankle 1989;10:68-80. [Google Scholar | PubMed]
- 9.Young PS, Bell SW, MacDuff EM, Mahendra A. Primary osseous tumors of the hindfoot: Why the delay in diagnosis and should we be concerned? Clin Orthop Relat Res 2013;471:871-7. [Google Scholar | PubMed]
- 10.Geirnaerdt MJ, Hogendoorn PC, Bloem JL, Taminiau AH, van der Woude HJ. Cartilaginous tumors: Fast contrast-enhanced MR imaging. Radiology 2000;214:539-46. [Google Scholar | PubMed]
- 11.Ahmed AR, Tan TS, Unni KK, Collins MS, Wenger DE, Sim FH. Secondary chondrosarcoma in osteochondroma: Report of 107 patients. Clin Orthop Relat Res 2003;411:193-206. [Google Scholar | PubMed]
- 12.Ferrer-Santacreu EM, Ortiz-Cruz EJ, González-López JM, Pérez Fernández E. Enchondroma versus low-grade chondrosarcoma in appendicular skeleton: Clinical and radiological criteria. J Oncol 2012;2012:437958. [Google Scholar | PubMed]
- 13.Brien EW, Mirra JM, Kerr R. Benign and malignant cartilage tumors of bone and joint: Their anatomic and theoretical basis with an emphasis on radiology, pathology and clinical biology. I. The intramedullary cartilage tumors. Skeletal Radiol 1997;26:325-53. [Google Scholar | PubMed]
- 14.Cawte TG, Steiner GC, Beltran J, Dorfman HD. Chondrosarcoma of the short tubular bones of the hands and feet. Skeletal Radiol 1998;27:625-32. [Google Scholar | PubMed]
- 15.Aoki J, Sone S, Fujioka F, Terayama K, Ishii K, Karakida O, et al. MR of enchondroma and chondrosarcoma: Rings and arcs of Gd-DTPA enhancement. J Comput Assist Tomogr 1991;15:1011-6. [Google Scholar | PubMed]
- 16.Landry MM, Sarma DP. In-situ chondrosarcoma of the foot arising in a solitary enchondroma. J Foot Surg 1990;29:324-6. [Google Scholar | PubMed]
- 17.Bakotic B, Huvos AG. Tumors of the bones of the feet: The clinicopathologic features of 150 cases. J Foot Ankle Surg 2001;40:277-86. [Google Scholar | PubMed]
- 18.Stoker DJ, Cobb JP, Pringle JA. Needle biopsy of musculoskeletal lesions. A review of 208 procedures. J Bone Joint Surg Br 1991;73:498-500. [Google Scholar | PubMed]
- 19.Ericksson AL, Schiller A, Mankin HJ. The management of chondrosarcoma of bone. Clin Orthop 1980;153:44-66. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Medial Subtalar Joint Dislocation in an 18-Year-Old Athlete with Pes Planus: Beyond A Simple Misstep
August 1, 2026 Medial Subtalar Joint Dislocation in an 18-Year-Old Athlete with Pes Planus: Beyond A Simple Misstep August 1, 2026 Thumb Distal Phalanx Enchondroma: Expanding the Surgical Corridor Through a Modified Volar Lateral Technique – A Case Report
August 1, 2026 Thumb Distal Phalanx Enchondroma: Expanding the Surgical Corridor Through a Modified Volar Lateral Technique – A Case Report July 1, 2026 Diagnostic Dilemma in a Distal Femoral Intramedullary Lesion: Enchondroma Mimicking Low-Grade Chondrosarcoma with Discordant Biopsy Findings: A Case Report
July 1, 2026 Diagnostic Dilemma in a Distal Femoral Intramedullary Lesion: Enchondroma Mimicking Low-Grade Chondrosarcoma with Discordant Biopsy Findings: A Case Report July 1, 2026 Resolution of Proximal Humerus Enchondroma in a 53-Year-Old Female with Curettage and Bone Substitution: A Case Report
July 1, 2026 Resolution of Proximal Humerus Enchondroma in a 53-Year-Old Female with Curettage and Bone Substitution: A Case Report