
Studies conducted on the effectiveness of TENS nailing for the treatment of femoral shaft fracture among children is sparse in this part of the country which prompts a need for this current study.
Dr. Srinivasa Reddy Suggu, Department of Orthopaedic Surgery, Vinayaka Missions Kirupananda Variyar Medical College and Hospital, Salem, Tamil Nadu, India. E-mail: srinivasareddy.suggu40@gmail.com
Introduction: The objective of the study was to evaluate the effectiveness of elastic stable intramedullary nailing titanium elastic nailing system (TENS) in the treatment of femoral shaft fractures among children (5–15 years) with particular importance to functional outcome and complications.
Methods: A hospital-based prospective study was conducted among 30 children with fracture shaft of femur who underwent elastic stable intramedullary nailing (TENS) in the department of Orthopaedics in Vinayaka Mission’s Kirupananda Variyar Medical College and Hospital, Salem. The study was conducted for a period of 2 years from January 2020 to December 2021. Postoperatively, the patients were followed up for clinical and radiological outcome and complications after internal fixation by Titanium elastic nailing at 6 weeks, 12 weeks, 6 months, and 1 year following surgery. Flynn criteria were used to assess the functional outcome during follow-up. To analyze the Data Statistical Package for the Social Sciences Version 21 is used. Categorical variables such as gender, side of fracture, and mode of injury are expressed as frequency and percentages. Continuous variables such as age and duration of surgery are expressed as mean (SD) or median (IQR). Statistical analysis was done using Chi-square test for categorical variables and independent samples t-test was used to determine the association for continuous variables with functional and radiological outcomes. To be considered as statistically significant, the P-value should be <0.05.
Results: With regard to outcome based on Flynn criteria, excellent outcome was observed among 22 (73.3%) children and satisfactory outcome was observed among 8 (26.7%) children. None of the children had poor outcome.
Conclusion: TENS is a safer and an effective procedure in terms of functional and radiological outcome among the children with fracture shaft of femur.
Keywords: Femoral shaft fractures, titanium elastic nailing system, Flynn criteria, functional outcome
One of the most important and common fractures in children is fracture of femur and they are the most incapacitating fracture in children. Approximately 1.6% of all the injuries related to bone are accounted by fracture of femur in children [1, 2]. These fractures have a bimodal distribution with respect to age with a peak at 6 and 16 years. Long bone fractures in children typically occur due to trauma, specially road traffic accidents [3, 4] and the second main cause being the abuse. Low velocity trauma leads to transverse fractures and high-speed causes comminuted or segmental fractures [5]. These fractures are more commonly seen in males with a sex ratio of 2:1 [6]. Conventionally, the treatment of these fractures is influenced by age, location of fracture, type of fracture, and the associated injuries. These fractures commonly heal rapidly along with spontaneous correction of angulation and are considered as the characteristic feature of these fractures. Hence, conservative treatment with spica cast immobilization generally results in good outcomes [7, 8]. The conservative methods of Hip Spica in femur is an acceptable standard of care for young children (<6 years), but in older children complications such as mal-union, shortening, angulation, joint stiffness, and delay in functional recovery are not uncommon [9, 10]. In addition to the above mentioned drawbacks, the conservative methods also results in longer period of hospital stay and hence imposes an economic burden [11]. Due to failure to obtain an acceptable reduction by the use of conservative methods, open fractures among the children and association with head injuries, multiple injuries, there is an increasing trend toward managing these fractures using surgical methods. In terms of operative treatment of these fractures, external fixation along with compression plating and intramedullary rigid nailing is considered as the best modalities [8, 12, 13, 14, 15, 16]. These methods also have its own complications such as infection of pin tract, loss of reduction, chances of refracture, and avascular necrosis of the femoral epiphysis [17]. Hence, the management of femoral diaphyseal shaft fracture among children in the intermediate age group has always been controversial and a point of debate. Moreover, the available literatures do not have enough evidence to support one procedure over the other. With the introduction of flexible intramedullary nailing, the surgeons have developed enthusiasm in the operative management of fractures of the lower limb of children [18]. This procedure was developed by Metaizeau and team from Nancy, France in 1982 [19]. It allows stable reduction and maintenance of reduction along with early mobilization [20]. It allows results in the early development of callus and allows restores the bone continuity very early when compared to other procedures particularly among children aged 5–14 years. This procedure is advantageous since it is relatively simple, does not violate the physics due to its load sharing internal splint and allows early mobilization with alignment. The basic principle of action of titanium elastic nailing system (TENS) is three point fixations which provide flexible, translational, axial and rotational stability. The callus formation by external bridging is fastened by the micro-motion which is provided by the elasticity of fixation. Since it is a closed procedure, it results in lesser risk of infection and relatively lesser disturbance in fracture hematoma and lessens the disturbance of periosteum [21]. Added to all of the above advantages, it is a minimally invasive procedure and it results in early removal of implant when compared to the plates. To the best of our knowledge, studies conducted on the effectives of TENS on the functional and radiological outcome along with the complications for the treatment of femoral shaft fracture among children is sparse in this part of the country. Hence, this study was conducted among the children (5–15 years) admitted with fracture shaft of femur who underwent flexible intramedullary nail with TENS in a tertiary care center Salem to determine the functional outcome and to determine the complications.
Study design
A hospital-based prospective study was conducted among the children with fracture shaft of femur who underwent elastic stable intramedullary nailing (TENS) in the department of Orthopaedics in Vinayaka Mission’s Kirupananda Variyar Medical College and Hospital, Salem. Study duration The study was conducted for a period of 2 years from January 2020 to December 2021.
Study population
All children with fracture shaft of femur who underwent elastic stable intramedullary nailing (TENS) in the department of Orthopaedics in Vinayaka Mission’s Kirupananda Variyar Medical College and Hospital, Salem, were included in the study.
Inclusion criteria
Children aged 5–15 years with diaphyseal (shaft) femur fracture.
Exclusion criteria
The following criteri a were excluded from the study:
• Patients (with)
• Fracture of distal 1/3rd of femoral shaft
• Not willing for surgery
• Comminuted fractures
• Segmental fractures.
Sample size and sampling.
Sample size
A total of 30 children with fracture shaft of femur were selected purposively until the sample size was reached.
Study procedure
After obtaining permission from the institute ethics committee and informed consent from the parents of the children, a pre-defined pro forma was used to obtain the socio-demographic and clinical characteristics of the children. Then, the clinical examination was performed for all the participants. Fracture anatomy was assessed with X-rays and computed tomography scans whenever needed. Routine investigations and assessment were performed before the surgery and all the patients were subjected to elastic stable intramedullary nailing. Following surgery, plain X-ray femur (antero-posterior and lateral view) including hip joint and knee joint was taken and the knee was splinted using a Thomas splint.
Follow-up
Postoperatively, the patients were followed up for clinical and radiological outcome of internal fixation by Titanium elastic nailing at 6 weeks, 12 weeks, 6 months and 1 year following surgery. The patients were also followed up for the complications at 6 weeks, 12 weeks, 6 months, and 1 year following surgery.
Study variables
Independent variables
• Age in years
• Gender
• Complaints
• Mode of injury
• Side of injury
• Type of fracture
• Location of fracture
• Weight bearing in weeks.
Outcome variables
• Functional and radiological outcome
• Perioperative complications.
Statistic analysis
Data were analyzed using Statistical Package for the Social Sciences V21 for Windows. Categorical variables such as gender, side of fracture, and mode of injury are expressed as frequency and percentages. Continuous variables such as age and duration of surgery are expressed as mean (SD) or median (IQR). Statistical analysis was done using Chi-square test for categorical variables and Independent samples t-test was used to determine the association for continuous variables with functional and radiological outcomes. To be considered as statistically significant, the P-value should be <0.05.
Ethical approval
The ethical approval was sought from the Institutional Ethics Committee. Informed consent was obtained from the informants of the children before data collection. Data were analyzed in aggregate and access to the collected data was limited only to me, my guide and co-guide. Confidentiality is maintained.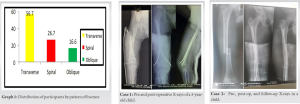

A total of 30 children aged 5–15 years with fracture shaft of femur were included in the study. All the children underwent elastic stable intramedullary nailing (TENS) and followed up at regular intervals till 1 year of surgery. The mean age of the children was 9.7 (2.5) years. The median age of the study participants was 10.0 (8.0–12.0) years with a minimum of 5 years and a maximum of 15 years. Majority (66.7%) of the children with fracture shaft of femur were males with a M:F of 2:1. Distribution of participants by mode of injury majority of the fractures (63.3%) were due to road traffic accidents and the remaining 11 children had fracture due to accidental fall. The mean age of the patients with fractures due to RTA was higher when compared to the mean age of the patients with fractures due to accidental fall, but it was not found to be statistically significant (P = 0.089). Distribution of participants by side of injury shows that the injury was more common on the right side, with majority (63.3%) children having injury on the right side. Distribution of participants by pattern of fracture shows that majority of patients (56.7%) had transverse pattern of fracture followed by spiral and oblique pattern which was present in 26.7% and 16.6% children, respectively. Distribution of participants by time between injury and surgery and duration of surgery shows that the median duration between the fracture and the surgery was 3.5 (2.0-5.25) days. The mean duration of surgery was 60.1 (18.8) min. The mean duration of hospital stay was 11.6 (4.2) days. The median duration of hospital stay was 10.5 (8.0–14.25) days with a minimum of 6 days and a maximum of 22 days. Distribution of participants according to time for union of fracture, the median duration of union was 12 (range: 10-20) weeks that more than 4/5th (83.4%) patients had their fracture united between 10 and 13 weeks of follow-up after surgery. Only one patient had the union at 18 weeks and it could be due the wound infection in that patient. The median duration of full weight bearing was achieved in 11 (range: 8–20) weeks. Limb length discrepancy (LLD) among the study participants shows that more than 3/4th (76.7%) children did not have any limb length discrepancy. Limb shortening and limb lengthening were noticed among three and four children, respectively, during the follow-up. Mal-alignment among the study participants shows that mal-alignment was noticed among five children operated with TENS for fracture shaft of femur. Angulation of <10° was present in two children and angulation of more than 10° was present among three children. Post-operative complications among the study participants shows that wound infection and pain was noticed among three and two children, respectively. Functional outcome according to Flynn criteria scoring shows that excellent outcome was observed among 22 (73.3%) children and satisfactory outcome was observed among 8 (26.7%) children. None of the children had poor outcome. This table shows that excellent outcome was observed among 22 (73.3%) children and satisfactory outcome was observed among 8 (26.7%) children. None of the children had poor outcome.
Fracture shaft of femur is one of the common pediatric orthopedic injuries in day to day practice. The femoral shaft fractures are treated by surgical methods among the adults; however, conservative treatment is mainly adopted among the children, mainly due to the better acceptance by the parents and children. However, it has a disadvantage of longer period of union and prolonged immobilization due to casting. For the treatment of lower extremity long bone fractures in this pediatric age group an ideal implant for should be load sharing, and should allow early mobilization, should not disrupt the blood supply of epiphyseal growth plates, it maintains limb length and alignment till the fracture heals which will be marked by bridging callus. Recently, after the introduction of flexible intra medullary nailing, the management of pediatric femoral shaft fractures, the procedure had gained popularity both in terms of acceptance and reduction in the loss of school days. Hence, it became imperative to determine the functional and radiological outcomes of fracture shaft of femur treated with TENS along with the complications among the children aged 5–15 years in a tertiary care Centre. Our study showed that the majority (66.7%) of the children with fracture shaft of femur were males with a M:F of 2:1 and the mean age of the children was 9.7 (2.5) years. A study by Sandhu et al. [22] had shown that males were 60.33% which is also comparable to Heybeli et al. [23] and Gamal et al. [24] where the males were 57.14% and 72.7%, respectively. This could be explained by the fact that the boys tend to involve in outdoor activities when compared to girls and more chance of road traffic accidents. These results are supported by various other studies conducted elsewhere [25, 26, 27, 28]. With regard to age, literatures have shown that the fracture has a bimodal distribution with the peak at age of two and at 17 years, which might be due to various factors. Various other studies have shown the similar results [29, 30]. Majority of the fractures (63.3%) were due to road traffic accidents and the remaining 11 children had fracture due to accidental fall. Our results are consistent with studies conducted by Heybeli et al. [31], Sandhu et al., Khurram and Humayun [32] and various other studies conducted across various countries [33, 34]. Our study also reported that there was no association for mode of injury with gender and age of the children. Majority of patients (56.7%) had transverse pattern of fracture followed by spiral and oblique pattern which was present in 26.7% and 16.6% children, respectively. Transverse fracture was the common pattern of fracture in studies conducted by Lal, Khazzam et al. [35], Yadav et al., Kumar [36], Cramer et al. [31], and Mann et al. [37]. However, a study by Venkataramana et al. had shown that spiral type of fracture was the common type of fracture in their study. The median duration between the fracture and the surgery was 3.5 (2.0–5.25) days and the mean duration of surgery was 60.1 (18.8) min. In a study by Nama [23], the average operative time was 35 min. The median duration of hospital stay was 10.5 (8.0–14.25) days in our study. According to the study by Sandhu et al., the average duration of hospital stay was 7.63 days and the average time interval between admission and surgery was 2.06 days. The average hospital stay was 6.47 days in a study by Agarwal et al. [38]. Similarly, the mean duration of hospital stay was 6.5 days in a study by Lal [39]. Saikia et al. [40] study observed a mean duration of hospital stay of 9.8 days. Our study showed that the median duration of union was 12 (range: 10–20) weeks and more than 4/5th (83.4%) patients had their fracture united between 10 and 13 weeks of follow up after surgery. Only one patient had the union at 18 weeks and it could be due the wound infection in that patient. The median duration of full weight bearing was achieved in 11 (range: 8–20) weeks. Our study results are similar to various other studies which showed the similar time for union and full weight bearing among the treated children. For instance, the average duration for union was 8.2 weeks in a study conducted by Mishra et al. A study by Agarwal et al. also had concluded that all the fractures healed in 10 weeks with an average time of union of 7.5 weeks. Bhuyan and Singh [41] in their study had stated that full weight bearing was achieved in 9 (8–12) weeks. The study also stated that radiologically, union was achieved in all the fractures with callus formation at 8–10 weeks of surgery. Similarly studies by Venkataramana et al., Hossain et al., [42] Saikia et al., Yadav et al., and Palanisamy et al. [43] had shown similar time for union and full weight bearing among their studies. More than 3/4th (76.7%) children did not have any limb length discrepancy in our study. Limb shortening and limb lengthening was noticed among three and four children, respectively, during the follow-up. Mal-alignment was noticed among five children operated with TENS for fracture shaft of femur. Angulation of <10° was present in two children and angulation of more than 10° was present among three children. Wound infection and pain were noticed among three and two children, respectively. A study by Mishra et al. had concluded that about 82.5% children achieved reduction without limb length discrepancy and limb shortening was noted among three children and lengthening was noted among four children. Mal-alignment of <5°, 5–10° and >10° was noted among 31, 8, and 1 children, respectively. Similarly a study by Agarwal et al. had shown that the complication commonly encountered was soft tissue irritation at the nail entry site seen in 2 Cases. Clinically, shortening was noticed in 3 Cases, while no patient had lengthening and 6 Cases had mal-alignment. However, a study by Siwach et al. [44] showed higher rates of complications. The study concluded that three patients had exposed implant, and 15 patients developed superficial infections among 63 children who underwent surgery for fracture shaft of femur. Bhuyan and Singh in their study among 40 children noticed limb lengthening in six children, varus mal-alignment was seen among four children and rotational mal-alignment in three children. Peri-operative difficulties encountered were failure of closed reduction in four cases and cork screwing of nails in two children. There were eight patients with LLD of 1–2 cm in a study by Kayaokay and Aktuglu [45]. A study by Nama observed only 1 Case with superficial wound infection among 30 children. These results show that the procedure was efficient in terms of complication following surgery, which is also proved by numerous other studies. With regard to outcome based on Flynn criteria, excellent outcome was observed among 22 (73.3%) children and satisfactory outcome was observed among 8 (26.7%) children. None of the children had poor outcome. Choudhari et al. study had shown that among 53 children in their study, excellent outcome was observed among 36 children. Good and poor outcome was observed among 14 and one child respectively. Siwach et al. had also concluded that forty-eight patients had excellent Flynn score, and 15 had a satisfactory score and none of the children had poor outcome according to Flynn criteria. Bhuyan and Singh study among 40 children with femoral shaft fracture had shown a comparable result where excellent result was achieved among 33 children (82.5%) and satisfactory results were observed among 7 children (17.5%). The results are similar with a study by Thapa et al. [46] where excellent outcome was observed among 49 children. Satisfactory outcome and poor outcome were observed among 6 and 1 child, respectively. Various other studies had shown similar results [47, 48, 49]. Hence, it can be safely argued that TENS is a safer and an effective procedure in terms of functional and radiological outcome among the children with fracture shaft of femur. However, the sample size was smaller in most of the studies and hence the results are to be reported with caution. Due to the less sample size, there is an issue of generalizability to a larger population. However, our study results could be generalized to the population of the similar setting. In addition to it, there was no comparator procedure in our study and hence the relative effectiveness of the procedure over the other procedures could not be ascertained.
Majority (66.7%) of the children with fracture shaft of femur were males with a M:F of 2:1 and the mean age of the children was 9.7 (2.5) years. Majority of the fractures (63.3%) were due to road traffic accidents and 56.7% children had transverse pattern of fracture. The median duration between the fracture and the surgery was 3.5 (2.0-5.25) days and the mean duration of surgery was 60.1 (18.8) min. The median duration of hospital stay was 10.5 (8.0-14.25) days. The median duration of union was 12 (range: 10–20) weeks and more than 4/5th (83.4%) patients had their fracture united between 10 and 13 weeks of follow-up after surgery. The median duration of full weight bearing was achieved in 11 (range: 8–20) weeks. More than 3/4th (76.7%) children did not have any limb length discrepancy in our study. Limb shortening and limb lengthening were noticed among three and four children, respectively, during the follow-up. Mal-alignment was noticed among five children operated with TENS for fracture shaft of femur. Angulation of <10° was present in two children and angulation of more than 10° was present among three children. Wound infection and pain was noticed among three and two children, respectively. With regard to outcome based on Flynn criteria, excellent outcome was observed among 22 (73.3%) children and satisfactory outcome was observed among 8 (26.7%) children. None of the children had poor outcome. TENS is a safer and an effective procedure in terms of functional and radiological outcome among the children with fracture shaft of femur. Based on the results from our study, we would suggest that TENS can become the first line of management of pediatric long bone fractures, especially in older children, more than 5 years and up to 15 years. Furthermore, in cases where maintaining reduction with a closed casting is a challenge like in children who are obese, with open fracture, mentally retarded, or those with neuromuscular disorders or if there is any hindrance to further rehabilitation and nursing care, surgical management with TEN can be preferred. Further large multicentric studies comparing various other procedures for the management of the pediatric fracture shaft of femur should be done to add more strength to our study findings.
Based on the results from our study, we would suggest that TENS nailing can become the first line of management of pediatric long bone fractures, especially in older children, more than 5 years and up to 15 years. Furthermore, in cases where maintaining reduction with a closed casting is a challenge like in children who are obese, with open fracture, mentally retarded, or those with neuromuscular disorders or if there is any hindrance to further rehabilitation and nursing care, surgical management with TENS nailing can be preferred.
References
- 1.Kasser JR, Beaty JH. Femoral shaft fractures. In: Beaty JH, Kasser JR, editors. Rockwood and Wilkins fractures in children. 6th ed. New York: Lippincott Williams and Wilkins; 2006. p. 893. [Google Scholar]
- 2.Loder RT, O’Donnel PW, Finberg JR. Epidemiology and mechanism of femur fracture in children. J Pediatr Orthop 2006;26:561-6. [Google Scholar]
- 3.Luedtke LM, Flynn JM, Ganley TJ, Hosalkar HS, Pill SG, Dormans JP. The orthopedists’ perspective: Bone tumors, scoliosis, 1and trauma. Radiol Clin North Am 2001;39:803-21. [Google Scholar]
- 4.Tscherne H, Regel G, Pape HC, Pohlemann T, Krettek C. Internal fixation of multiple fractures in patients with polytrauma. Clin Orthop 1998;347:62-78. [Google Scholar]
- 5.Bar-On E, Sagiv S, Porat S. External fixation or flexible intramedullary nailing for femoral shaft fracture in children. A prospective, randomised study. J Bone Joint Surg Br 1997;79:975-8. [Google Scholar]
- 6.Koval KJ, Zuckerman JD. Handbook of fractures. 3rd ed. New York: Lippincott Willians & Wilkins; 2006. [Google Scholar]
- 7.Irani RN, Nicholson JT, Chung SM. Long-term results in the treatment of femoral-shaft fractures in young children by immediate spica immobilisation. J Bone Joint Surg Am 1976;58:945-51. [Google Scholar]
- 8.Henderson OL, Morrissy RT, Gerdes MH, McCarthy RE. Early casting of femoral shaft fractures in children. J Pediatr Orthop 1984;4:16-21. [Google Scholar]
- 9.Tscherne H, Regel G, Pape HC. Internal fixation of multiple fractures in patients with polytrauma. Clin Orthop 1998;347:62-78. [Google Scholar]
- 10.Jacob E, Selvam N. Titanium elastic nailing in femur: Surg Sci 2010;1:15-9. [Google Scholar]
- 11.Wood JN, Fakeye O, Mondestin V, Rubin DM, Localio R, Feudtner C. Prevalence of abuse among young children with femur fractures: A systematic review. BMC Pediatr 2014;14:169. [Google Scholar]
- 12.McCartney D, Hinton A, Heinrich SD. Operative stabilization of pediatric femur fractures. Orthop Clin North Am 1994;25:635-50. [Google Scholar]
- 13.Krettek C, Haas N, Walker J, Tscherne H. Treatment of femoral shaft fractures in children by external fixation. Injury 1991;22:263-6. [Google Scholar]
- 14.Aronson J, Tursky EA. External fixation of femur fractures in children. J Pediatr Orthop 1992;12:157-63. [Google Scholar]
- 15.Ward WT, Levy J, Kaye A. Compression plating for child and adolescent femur fractures. J Pediatr Orthop 1992;12:626-32. [Google Scholar]
- 16.Skak SV, Overgaard S, Nielsen JD, Andersen A, Nielsen ST. Internal fixation of femoral shaft fractures in children and adolescents: A ten to twenty one year follow up of 52 fractures. J Pediatr Orthop 1996;5:195-9. [Google Scholar]
- 17.Beaty JH, Austin SM, Warner WC, Canale ST, Nichols L. Interlocking intramedullary nailing of femoral-shaft fractures in adolescents: Preliminary results and complications. J Pediatr Orthop 1994;14:178-83. [Google Scholar]
- 18.Flynn JM, Skaggs D, Sponseller PD, Ganley TJ, Kay RM, Leitch KK. The operative management of pediatric fractures of the lower extremity. J Bone Joint Surg 2002;84:2288-300. [Google Scholar]
- 19.Flynn JM, Schwend RM. Management of pediatric femoral shaft fractures. J Am Acad Orthop Surg 2004;12:347-59. [Google Scholar]
- 20.Hedin H. Surgical treatment of femoral fractures in children comparison between external fixation and elastic intramedullary nails: A review. Acta Orthop Scand 2004;75:231-40. [Google Scholar]
- 21.Gwyn DT, Olney BW, Dart BR, Czuwala PJ. Rotational control of various pediatric femur fractures stabilized with titanium elastic intramedullary nails. J Pediatr Orthop 2004;24:172-7. [Google Scholar]
- 22.Sandhu KS, Kaur M, Singh H, Sandhu A. Evaluation of outcome, safety, and efficacy of diaphyseal fracture of femur and tibia in children-treated by titanium elastic nailing system (TENS). EJMCR 2021;8:4000-10. [Google Scholar]
- 23.Nama KG. Treatment of fracture shaft femur in paediatric age group with titanium elastic nail. JEMDS 2017;6:4729. [Google Scholar]
- 24.El-Adl G, Mostafa MF, Ahmed K. Titanium elastic nail fixation for paediatric femoral and tibial fractures. Acta Orthop 2009;75:512-20. [Google Scholar]
- 25.Choudhari P, Chhabra S, Kiyawat V. Evaluation of results of titanium elastic nailing system in paediatric lower extremity fractures of long bones. J Evol Med Dent Sci 2014;3:15303-9. [Google Scholar]
- 26.Venkataramana P, Mahesh S, Nagendra GS. A prospective study of surgical management of diaphyseal fractures of femur in children aged between 5 to 16 years using elastic stable intra medullary nailing. J Evol Med Dent Sci 2014;3:2268-86. [Google Scholar]
- 27.Flynn JM, Hresko T, Reynolds RA, Blasier RD, Davidson R, Kasser J. Titanium elastic nails for pediatric femur fractures: A multicenter study of early results with analysis of complications. J Pediatr Orthop 2001;21:4-8. [Google Scholar]
- 28.Khajotia BL, Sunil S, Singh BR. Evaluation of functional outcome of titanium elastic nail (TENS) in femoral shaft fracture in children. Int J Med Res Prof 2017;3:59-63. [Google Scholar]
- 29.Jalan D, Chandra R, Sharma VK. Results of titanium elastic nailing in paediatric femoral diaphyseal fractures-report of 30 cases. Chin J Traumatol 2013;16:77-83. [Google Scholar]
- 30.Kumar N, Chaudhary L. Titanium elastic nails for pediatric femur fractures: Clinical and radiological study. Surg Sci 2010;1:15-9. [Google Scholar]
- 31.Cramer KE, Tornetta P 3rd, Spero C, Alters S, Moraljakbar H, Ieefy J. Ender rod fixation of femoral shaft fractures in children. Clin Orthop 2000;376:119-23. [Google Scholar]
- 32.Khurram B, Humayun B. Flexible intramedullary nailing versus external fixation of paediatric femoral fractures. Acta Orthop 2006;72:159-63. [Google Scholar]
- 33.Soni JF, Schelle G, Valenza W, Pavelec AC, Souza CD. Unstable femoral fractures treated with titanium elastic intramedullary nails, in children. Rev Bras Ortop 2015;47:575-80. [Google Scholar]
- 34.Yadav AD, Madhukar, Reddy VN. Prospective study of tens in femoral diaphyseal fractures among paediatric age group. IJOS 2018;4:881-4. [Google Scholar]
- 35.Khazzam M, Tassone C, Liu XC, Lyon R, Freeto B, Schwab J, et al. Use of flexible intramedullary nail fixation in treating femur fractures in children. Am J Orthop (Belle Mead NJ) 2009;38:E49-55. [Google Scholar]
- 36.Kumar YS. A prospective study of functional outcome of treatment of fracture shaft femur in children using titanium elastic nails system. IJHCR 2021;4:103-5. [Google Scholar]
- 37.Mann DC, Weddington J, Davenport K. Closed Ender nailing of femoral shaft, fractures in adolescents. J Pediatr Orthop 1986;6:651-5. [Google Scholar]
- 38.Agarwal B, Jindal RC, Singh M. Functional outcome of treatment of fracture shaft femur in children using titanium elastic nails system. J Evol Med Dent Sci 2020;9:453-7. [Google Scholar]
- 39.Lal RM. A prospective study of functional outcome of treatment of fracture shaft femur in children using titanium elastic nails system sciences. IOSRJDMS 2020;19:1-4. [Google Scholar]
- 40.Saikia K, Bhuyan S, Bhattacharya T, Saikia S. Titanium elastic nailing in femoral diaphyseal fractures of children in 6-16 years of age. Indian J Orthop 2007;41:381-5. [Google Scholar]
- 41.Bhuyan BK, Singh SM. Titanium elastic nailing in pediatric femoral diaphyseal fractures in the age group of 5-16 years-A short term study. J Clin Orthop Trauma 2014;5:203-10. [Google Scholar]
- 42.Hossain MM, Alam QS, Haque E, Rahman MS. Management of fracture shaft of femur in children with titanium elastic nailing (TEN) at Dhaka medical college hospital, Bangladesh. J Dhaka Med Coll 2015;23:24-30. [Google Scholar]
- 43.Palanisamy MB, Balasubramanian K, Kumar S, Rajan MA. A study of functional outcome of titanium elastic nailing in paediatric femoral diaphyseal fractures. IJCMPR 2016;2:789-94. [Google Scholar]
- 44.Siwach K, Kumar V, Arora K, Beniwal R, Mittal A, Nandal G. Functional assessment of diaphyseal femoral fractures in pediatric age group managed by titanium elastic nail system: A prospective study. J Orthop Dis Traumatol 2020;3:116-20. [Google Scholar]
- 45.Kayaokay K, Aktuglu K. Titanium elastic nailing in pediatric femoral diaphyseal fractures in the age group of 6-15 years mid-term and long-term outcomes. Pak J Med Sci 2018;34:1529-33. [Google Scholar]
- 46.Thapa SK, Poudel KP, Marasini RP, Dhakal S, Shrestha R. Paediatric diaphyseal femur fracture treated with intramedullary titanium elastic nail system. JCMS Nepal 2015;11:20-2. [Google Scholar]
- 47.Lohiya R, Bachhal V, Khan U, Kumar D, Vijayvargiya V, Sankhala SS, et al. Flexible intramedullary nailing in paediatric femoral fractures. A report of 73 cases. J Orthop Surg Res 2011;6:64. [Google Scholar]
- 48.Gupta S, Hegde J. Prospective study of management of diaphyseal fractures of femur in paediatric age group by titanium elastic nailing system. J Med Thesis 2014;2:19-23. [Google Scholar]
- 49.Mahar SA, Abbasi MK, Bhayo A, Chandio MS, Palh HB, Bhatti SH. Functional outcome of intramedullary fixation with titanium elastic nails in diaphyseal fractures of femur in children. PJMHS 2020;14:610-2. [Google Scholar]






