
The titanium elastic nailing system (TENS) provides stable fixation with mechanical axis preservation in children with femur shaft fracture in school-aged children irrespective of fracture pattern.
Dr Ankit Tripathi, Department of Orthopaedics, Baba Raghav Das Medical College, Gorakhpur - 273013, Uttar Pradesh, India. E-mail: ankit.aki02@gmail.com
Abstract
Introduction: Paediatric femoral shaft fractures are one of the commonest injuries in early childhood and school-going children, with operative management increasingly preferred in the age group of 6–13 years. The titanium elastic nailing system (TENS) is the most preferred modality in this age group, providing stable fixation and biological preservation; however, its effect on mechanical axis alignment and early functional outcome needs evaluation. In this study, we aim to analyse the effect of femur shaft fractures being managed by TENS on the mechanical axis of the lower limb and its effect on the functional outcome of the patients after a short immobilisation period of 2 weeks.
Materials and Methods: A prospective observational study was conducted at Baba Raghav Das Medical College, Gorakhpur, between 2023 and 2025, including 32 children aged 6–13 years with femoral diaphyseal fracture undergoing TENS (excluding Gustillo-Anderson type IIIB/IIIC injuries). Regular follow-up was done at 2, 6, and 12 weeks, and functional and radiological outcomes and mechanical alignment were recorded at 12 weeks using Flynn scoring criteria and an orthoscanogram, respectively.
Results: Our study group had a mean age of 9.66 ± 2.25 years, with a higher male predilection (71.9%) and road traffic accidents (43.8%) being the common mode of injury. We observed radiological union in all the patients with a mean union time of 10.88 ± 0.9 weeks, with no significant malalignment with the mean medial proximal tibial angle and lateral distal femoral angle within an acceptable range, even after a short immobilisation period. We observed a mean knee flexion of 112.7° ± 13.7° at the 12-week follow-up, with 81.2% of patients having an excellent outcome and the remaining 18.8% having a satisfactory outcome with no poor results.
Conclusion: TENS is a safe, minimally invasive, alignment-preserving modality which provides stable fixation and excellent short-term outcomes with minimal complications in the 6–13-year age group, irrespective of age, gender, or fracture type.
Keywords: Paediatric femur shaft fracture, titanium elastic nailing system, elastic stable intramedullary nailing, mechanical axis alignment, functional outcome (Flynn criteria).
Paediatric femur shaft fractures are one of the common injuries, with an annual incidence estimated at 20–25/100,000 children in India [1], usually occurring in early childhood (1–3 years) during the transition from weak woven bone to strong lamellar bone or in adolescence due to high-energy trauma, with a 2.6 times higher predilection in males [2]. Although the aetiology of the fracture varies with the age of the child, the most common cause of femur shaft fractures in children is a fall from height and road traffic accidents [3]. However, child abuse is still one of the commonest causes of these fractures in children <18 months of age, as reported by Coffey et al. [4]. Management modalities of these fractures in <5 years of age include hip spica application and interlocking nailing in adolescents over 15 years of age. Although the superiority of one particular modality has still not been established for the management of these fractures in the 5–15-year age group, evidence from multiple studies has favoured the use of the titanium elastic nailing system (TENS) with favourable outcomes allowing early mobilisation as reported amongst the school-going age group [5,6,7]. TENS as a fixation method provides rotational stability and allows micromotion, leading to early fracture union, providing high patient satisfaction; however, a high complication rate of 60% has been reported in the studies, which are primarily due to poor patient selection, improper surgical techniques, and post-operative management protocols [8]. Most of the studies reported employ various postoperative immobilisation techniques, including hip spica cast, knee immobiliser, above-knee cast, hip-knee-ankle-foot orthosis and Thomas splints for a variable period ranging from 2 to 6 weeks. These studies also mainly focus on fracture union, complications, and functional outcome after TENS nailing of paediatric femur shaft fracture, but its effect on the mechanical axis of the lower limb is scarcely reported. With our study, we aim to analyse the effect of femur shaft fractures being managed by TENS on the mechanical axis of the lower limb and its effect on the functional outcome of the patients after a short immobilisation span of 2 weeks in an above-knee plaster of Paris (POP) slab.
An observational prospective study was conducted in the Department of Orthopaedics, Baba Raghav Das Medical College, between 2023 and 2025 after obtaining Institutional Ethics Committee approval (S. No. 232/IHEC/2025), including 32 patients of the 6–13 years age group with a femur shaft fracture (except Gustilo Anderson types IIIB and IIIC injuries) after informed parental consent. After pre-operative blood investigations and radiological investigations, including anteroposterior and lateral views of full-length femur radiographs (for pre-operative planning of implant size calculation to achieve approximately 80% of canal diameter and location of pre-bending distance), after anaesthetic fitness with appropriate anaesthesia, patients were placed on the fracture table. Fracture reduction was achieved under fluoroscopy guidance, and patients were prepared and draped for the TENS nailing. Under fluoroscopic guidance, a 1–2 cm longitudinal skin incision was made over the lateral and medial aspects of the distal femur, starting 2 cm proximal to the distal femoral epiphyseal plate. The entry was made using a bone awl, and two appropriate-sized, adequately pre-bent TENS nails were introduced from the lateral and medial aspects of the distal femur till the fracture line. After anatomical or near-anatomical reduction under C-arm, the TENS nails were subsequently introduced in a retrograde manner with a rotary motion and gentle tap till the greater trochanter and femoral neck, respectively. Postoperatively, patients were maintained in an above-knee POP slab for 2 weeks till suture removal, along with a non-weight-bearing gait with a walker. Active and passive knee range of motion was started after 2 weeks, and non-weight-bearing gait was continued till 6 weeks, followed by partial weight-bearing. Full weight-bearing was permitted after confirmation of radiological union at 10–12 weeks. Patients were clinico-radiologically followed during this period at 2, 6, and 12 weeks, and mechanical axis measurement was performed using an orthoscannogram at 6 and 12-week follow-ups (Fig. 1).

Figure 1: Example case: (a) Plain pre-operative anteroposterior (AP) and lateral view radiograph of a 9-year-old male child sustaining right femoral fracture (transverse type) following a fall from bed while playing. (b) Immediate post-operative X-ray AP and lateral views of the femur shaft after titanium elastic nailing system. (c) 8-week post-operative orthoscanogram showing callus formation (arrow marked). (d) 12-week post-operative orthoscanogram showing fracture union and findings consistent with approximately 2° of residual femoral varus deformity with no limb length discrepancy.
Functional outcome was assessed using the Flynn scoring system (Table 1) at the 12-week follow-up.
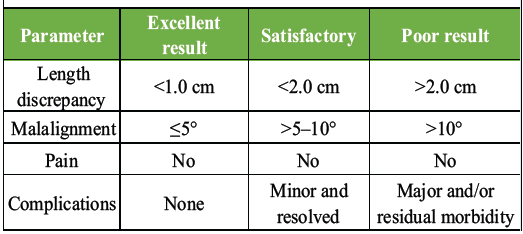
Table 1: Flynn criteria for femur shaft fracture
Statistical analysis was performed using IBM Statistical Package for the Social Sciences 28 (NY, USA) software. The normal distribution suitability was performed using the Shapiro–Wilk/Kolmogorov–Smirnov test. Categorical variables were expressed as frequency and percentage, while continuous variables were expressed as mean ± standard deviation. The comparison among groups was done using the Mann–Whitney U test and one-way analysis of variance (ANOVA) test, wherever applicable. A P < 0.05 was considered significant.
Demographics:
Out of 32 patients, 23 patients (71.9%) were male, with 9–11 years being the most common age group (13 patients; 40.6%), with a mean age of 9.66 ± 2.25 years. Road traffic accidents were the most common mode of injury occurring in 43.8% (14 patients), followed by a fall from height in 31.4% (10 patients). The majority of the patients in our study population had an oblique-type fracture pattern (16 patients; 50%), followed by a transverse fracture in 10 patients (31.3%), a spiral fracture in 5 patients (15.6%), and an intact wedge pattern in one patient (3.1%).
Outcome:
At the 12-week follow-up, clinically, the majority of the patients were found to have knee flexion of 100–130° with the mean knee flexion of 112.7° ± 13.7° with no significant effect of fracture pattern (P = 0.888; one-way ANOVA test). The functional outcome based on the Flynn scoring system showed 81.2% (26 patients) having an excellent outcome, followed by 6 patients (18.8%) with a satisfactory outcome. However, the outcome was not found to be significantly associated with different age groups, gender, and fracture pattern (P = 0.235, 0.495, and 0.873, respectively; Mann–Whitney U test) (Table 2 and Fig. 2).
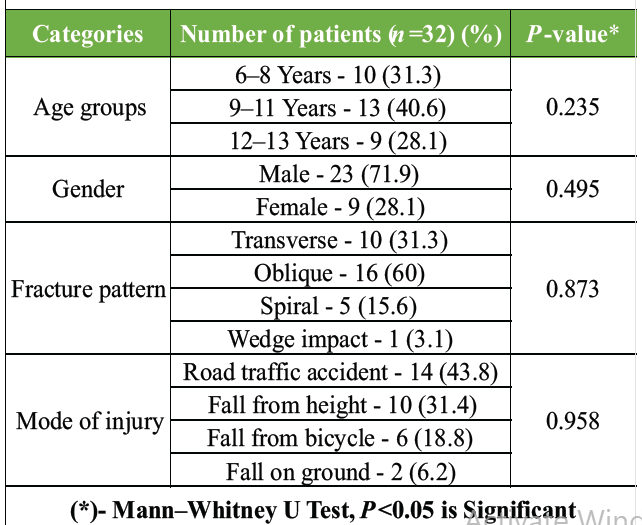
Table 2: Demographics and their effect on functional outcome

Figure 2: Bar chart showing the relationship between functional outcomes based on fracture pattern.
Radiological assessment at 12 weeks showed union in all the patients of our study, with a time of union ranging from 9 to 12 weeks, with a mean union of 10.88 ± 0.9 weeks, with no significant difference among different fracture patterns (P = 0.203; one-way ANOVA test). The mean medial proximal tibial angle (mPTA) was found to be 87.5° ± 2.1°, while the mean lateral distal femoral angle (LDFA) was 87.9° ± 3.5° with no significant association noted with the fracture pattern (P = 0.713 and 0.823, respectively; one-way ANOVA test). No significant malalignment was noted among our study participants at the end of 12 weeks, with only one patient having shortening of the affected lower limb by approximately 2 cm. No further incidences of non-union, fixation failure, and persistent pain were observed (Table 3).
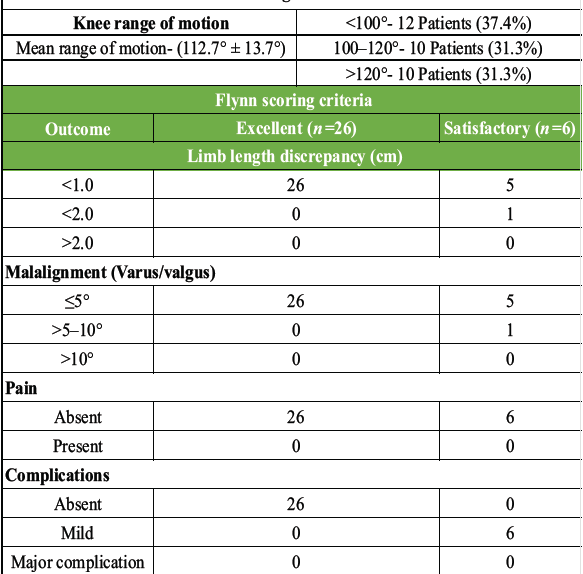
Table 3: Outcome-knee range of motion and functional outcome based on Flynn scoring criteria
Our study included 32 patients aged 6–13 years with femoral diaphyseal fractures being managed by TENS, which is the most preferred modality of fracture management in this age group, as it provides stable fixation while preserving both biology and growth potential. The demographic distribution of our study group was comparable to study groups of Flynn et al., Mann et al., Ligier et al. and others [5,9,10,11,12], where they had included patients with a mean age ranging from 8.5 to 12.7 years with road traffic accidents as the major mode of injury, similar to the mean age of 9.66 ± 2.25 years from our study group. Our study group also had 2.5 times more predilection towards school-aged boys due to higher outdoor activity and increased risk of trauma, which closely mimicked findings of Hedlund and Lindgren [3]. Fracture union was noted amongst all the patients of our study population, with time of union ranging from 9 to 12 weeks with a mean union time of 10.88 ± 0.9 weeks, which was comparable to the union time of 8–12 weeks as reported in studies by Ansari et al., Bhuyan and Mohan Singh, Mishra et al. and others [9,10,13,14,15,16,17]. In accordance with a comparative study by Sahu and Goswamy [18], we also did not observe a significant difference in the union time among different fracture patterns (P = 0.203), emphasising the importance of proper technique with an appropriately sized, pre-bent nail as used in our study in providing effective stability irrespective of fracture pattern. Further, the absence of non-union or delayed union emphasises the advantage of using a TENS nail in preserving biology at the fracture site. Maintenance of alignment remains pivotal in determining long-term functional outcome in paediatric femoral shaft fractures. In accordance with the findings of a meta-analysis by Imam et al. and Kayaokay and Aktuglu [19,20], the radiological parameters such as mean mPTA (87.5° ± 2.1°) and mean LDFA (87.9° ± 3.5°) of our study group with a short immobilisation period of 2 weeks in an above-knee POP slab remained within acceptable limits with no clinically significant malalignment irrespective of fracture pattern and only one patient reporting shortening of approximately 2 cm at 12 weeks of follow-up. These findings further affirm superior coronal and sagittal alignment, along with clinically insignificant limb length discrepancy (LLD) with TENS when compared with conservative management when used with proper technique. However, inter-observer and intra-observer variability assessment and rotational malalignment were not included in this study. Functionally, at 12-week follow-up, the majority of the patients had achieved a knee range of motion of 100–130° and a mean of 112.7° ± 13.7° with no significant impact of fracture pattern (P = 0.888). According to the Flynn Scoring Criteria, we observed 81.2% of patients to have excellent and the remaining 18.8% to have satisfactory outcomes with no poor outcomes, which was consistent with previously reported outcomes where 80–90% of patients had excellent to satisfactory outcomes [5,7,9,13,14,16,21,22]. Furthermore, as the functional outcomes observed in our study were not significantly associated with age, gender, and fracture patterns, it emphasises the uniform effectiveness of TENS across all the subgroups within 6–13 years of age (Table 4).
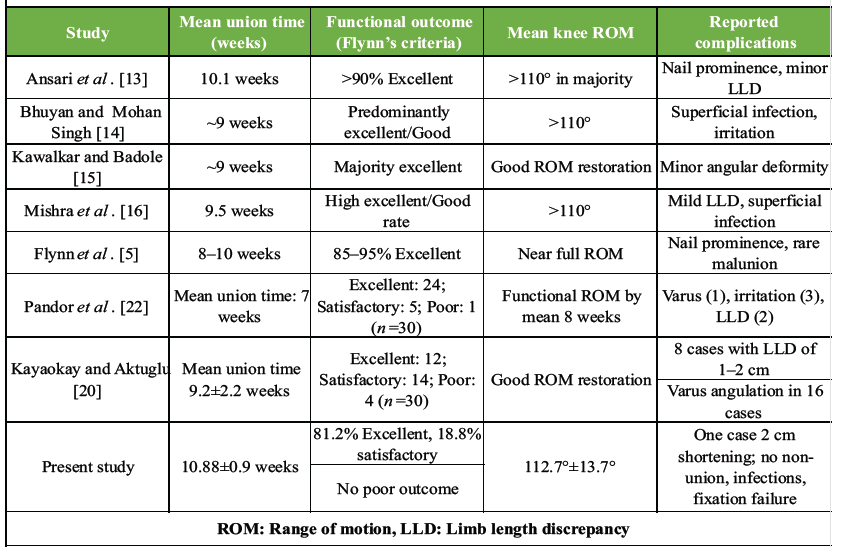
Table 4: Comparison table of literature review with our study on the titanium elastic nailing system of pediatric femur shaft fractures
With a varied post-operative immobilisation as reported in literature, ranging from 6 weeks of immobilisation in a Thomas splint by Ansari et al. [13] to a long knee brace for a varied period of 2–5 weeks by Bhuyan and Mohan Singh, Donati et al. and others [5,14,21], with our short immobilisation period of 2 weeks in an above-knee brace, we found no malalignment or significant LLD in our study group with an excellent to satisfactory outcome in all the patients. However, in contrast to our study, Hathiwale et al., Pandor et al., and Bairwa et al. [7,9,22] observed that a complete knee range of movement was achieved early, compared to a mean range of 112.7° ± 13.7° at 12 weeks in our study group. They had also observed a higher rate of complication, that is, varus malalignment, LLD, with a comparatively higher rate of poor functional outcome when no post-operative immobilisation was used, emphasising the superiority of our method of short post-operative immobilisation for 2 weeks compared to immediate post-operative mobilisation in maintaining alignment and achieving a higher functional outcome. Despite having the strength of being a prospective study where a short immobilisation period was given to achieve a good functional and radiological outcome, along with a knee range of movement. Our study is limited by its small sample size, single-centre design, short follow-up duration, and lack of a comparative group, which may limit generalisability of our findings in the population and understanding of long-term effects of remodelling on malalignment. We also noted that due to the short follow-up duration, the common complications such as implant irritation and related infections, refracture after implant removal, and late LLD could not be assessed.
The findings of our study support the use of TENS nails in providing stable fixation, reliable union with an excellent functional outcome, and minimal complications with early mobilisation, even with a short immobilisation period of 2 weeks. This further strengthens its role as a safe, minimally invasive, and alignment-preserving treatment modality in all the subgroups of the 6–13-year age group. However, with all the limitations of the study, we recommend the need for a large multicentric randomised comparative study with a longer follow-up duration to validate these findings and to further assess the effect of remodelling potential on limb alignment and patient-related outcome measures of TENS nailing in the 6–13 year age group.
- TENS provides stable fixation with mechanical axis preservation in children with femur shaft fracture in 6–13 years age group
- Early knee mobilization after a short immobilization period of 2 weeks does not compromise fracture healing and alignment
- Functional outcome assessment using the Flynn criteria demonstrated excellent to satisfactory result in school-aged children when proper techniques were followed
- Complication rates can be minimised with appropriate patient selection and proper techniques of fixation with adherence to fixation principles.
Recommendations:
- TENS should be considered the preferred treatment modality for diaphyseal femoral fractures in children aged 6–13 years without severe open injuries irrespective of type of fracture
- Careful pre-operative planning, including appropriate nail diameter selection and adequate pre-bending, is essential in achieving stable fixation and maintain post-operative lower limb alignment
- Early mobilization protocols with a short immobilization period can be safely implemented to enhance functional recovery without affecting knee alignment
- Larger multicentric studies with long-term follow-up are recommended to assess growth-related outcomes, late deformities, patient-reported outcome measures, including quality of life assessment, and return to activity and sports to assess post-operative recovery after TENS nailing.
References
- 1. Khosla S, Melton III LJ, Dekutoski MB, Achenbach SJ, Oberg AL, Riggs BL. Incidence of childhood distal forearm fractures over 30 years: A population-based study. JAMA 2003;290:1479-85. [Google Scholar] [PubMed]
- 2. Kumar P, Kumar P, Singh SP. Treatment of Long Bone Fracture in Children by Titanium Elastic Nailing Stabilisation. Int J Med Res Prof. 2019 Jan; 5(1):152-56. DOI:10.21276/ijmrp.2019.5.1.033. [Google Scholar] [PubMed] [CrossRef]
- 3. Hedlund R, Lindgren U. The incidence of femoral shaft fractures in children and adolescents. J Pediatr Orthop 1986;6:47-56. [Google Scholar] [PubMed]
- 4. Coffey C, Haley K, Hayes J, Groner JI. The risk of child abuse in infants and toddlers with lower extremity injuries. J Pediatr Surg 2005;40:120-3. [Google Scholar] [PubMed]
- 5. Flynn JM, Hresko T, Reynolds RA, Blasier RD, Davidson R, Kasser J. Titanium elastic nails for paediatric femur fractures: A multicentre study of early results with analysis of complications. J Pediatr Orthop 2001;21:4-8. [Google Scholar] [PubMed]
- 6. Moroz LA, Launay F, Kocher MS, Newton PO, Frick SL, Sponseller PD, et al. Titanium elastic nailing of fractures of the femur in children. Predictors of complications and poor outcome. J Bone Joint Surg Br 2006;88-B:1361-6. [Google Scholar] [PubMed]
- 7. Hathiwale MI, Mundewadi VM, Ahmed MN. Prospective study of surgical management of femoral shaft fractures in children using TENS nails. Int J Res Orthop 2023;10:69-74. [Google Scholar] [PubMed]
- 8. Parikh SN, Jain VV, Denning J, Tamai J, Mehlman CT, McCarthy JJ, et al. Complications of elastic stable intramedullary nailing in paediatric fracture management: AAOS exhibit selection. J Bone Joint Surg Am 2012;94:e184. [Google Scholar] [PubMed]
- 9. Bairwa DK, Agarwal A, Kumar A, Gujjar S. Outcome of femoral shaft fracture in paediatric age group with titanium elastic nail. Int J Res Orthop 2025;11:1473-9. [Google Scholar] [PubMed]
- 10. Cramer DC GD. Clinical Anatomy of the Spine, Spinal Cord, and ANS. 3rd ed. Chantilly: Mosby; 2013. p. 1. [Google Scholar] [PubMed]
- 11. Mann DC, Weddington J, Davenport K. Closed ender nailing of femoral shaft fractures in adolescents. J Pediatr Orthop 1986;6:651-5. [Google Scholar] [PubMed]
- 12. Ligier J, Metaizeau J, Prevot J, Lascombes P. Elastic stable intramedullary nailing of femoral shaft fractures in children. J Bone Joint Surg Br 1988;70-B:74-7. [Google Scholar] [PubMed]
- 13. Ansari MAQ, Mahajabeen A, Fatima A. A study of titanium elastic nailing in the surgical management of fracture shafts of the femur in children. Indian J Orthop Surg. 2021;7(3):227-232. doi:10.18231/j.ijos.2021.037. [Google Scholar] [PubMed] [CrossRef]
- 14. Bhuyan BK, Mohan Singh S. Titanium elastic nailing in paediatric femoral diaphyseal fractures in the age group of 5-16 years – a short-term study. J Clin Orthop Trauma 2014;5:203-10. [Google Scholar] [PubMed]
- 15. Kawalkar A, Badole CM. Percutaneous titanium elastic nail for femoral shaft fracture in patients between 5 and 15 years. J Orthop 2018;15:695-700. [Google Scholar] [PubMed]
- 16. Mishra AK, Chalise PK, Shah SB, Adhikari V, Singh RP. Diaphyseal femoral fractures in children treated with a titanium elastic nail system. Nepal Med Coll J 2013;15:95-7. [Google Scholar] [PubMed]
- 17. Galpin RD, Willis RB, Sabano N. Intramedullary nailing of paediatric femoral fractures. J Pediatr Orthop 1994;14:184-9. [Google Scholar] [PubMed]
- 18. Sahu R, Goswamy B. A comparative study of management of femoral shaft fracture in children: A prospective study. J Orthop Traumatol Rehabil 2020;12:115-20. [Google Scholar] [PubMed]
- 19. Imam MA, Negida AS, Elgebaly A, Hussain AS, Ernstbrunner L, Javed S, et al. Titanium elastic nails versus spica cast in paediatric femoral shaft fractures: A systematic review and meta-analysis of 1012 patients. Arch Bone Jt Surg 2018; 6:176-88. [Google Scholar] [PubMed]
- 20. Kayaokay K, Aktuglu K. Titanium elastic nailing in paediatric femoral diaphyseal fractures in the age group of 6-15 years: mid-term and long-term outcomes. Pak J Med Sci 2018;34:1529-33. [Google Scholar] [PubMed]
- 21. Donati F, Mazzitelli G, Lillo M, Menghi A, Conti C, Valassina A, et al. Titanium elastic nailing in diaphyseal femoral fractures of children below six years of age. World J Orthop 2017;8:156-62. [Google Scholar] [PubMed]
- 22. Pandor I, Sharma A, Jagdale A, Shaikh A, Doifode A, Rank N. Outcome of paediatric femoral shaft fractures treated with titanium elastic nailing: A prospective study. J Orthop Case Rep 2025;15:399-404. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Outcome of Retrograde Titanium Elastic Nailing System in Shaft of Humerus Fractures: A Case Series
August 1, 2026 Outcome of Retrograde Titanium Elastic Nailing System in Shaft of Humerus Fractures: A Case Series March 1, 2025 Titanium Elastic Nail System for Middle One-Third Clavicle Fractures: Impact on Functional Recovery
March 1, 2025 Titanium Elastic Nail System for Middle One-Third Clavicle Fractures: Impact on Functional Recovery September 10, 2022 A Prospective Study on the Functional Outcome of Diaphyseal Fractures of Femur Treated with TENS Nailing in Pediatric age Group (5–15 years)
September 10, 2022 A Prospective Study on the Functional Outcome of Diaphyseal Fractures of Femur Treated with TENS Nailing in Pediatric age Group (5–15 years) September 10, 2023 Denosumab-associated Periprosthetic Atypical Femur Fracture: A Case Report
September 10, 2023 Denosumab-associated Periprosthetic Atypical Femur Fracture: A Case Report