
Treatment of adult hypophosphatemic patients with coxa vara and a femoral neck stress fractures can be surgical treatment with femoral cephalomedullary nail for combined deformity correction and fracture fixation.
Dr. Maria Tirta, Department of Orthopaedics, Aalborg University Hospital, Aalborg 9000, Denmark. E-mail: mariatirta96@gmail.com
Abstract
Introduction: X-linked hypophosphatemic rachitis (XLHR) is the most common cause of hereditary rickets that can lead to long bone deformities requiring multiple surgical correction procedures. In addition, high rates of fractures are reported in adult XLHR patients. This study aimed to report a case of femoral neck stress fracture in XLHR patient treated with mechanical axis correction. No previous studies demonstrating a combined valgus correction and cephalomedullary nail fixation were identified in the literature.
Case Report: A 47-year-old male patient with XLHR attended the outpatient clinic with severe left hip pain. X-rays revealed a left proximal femoral varus deformity and a femoral neck stress fracture. After 1 month without improvement of pain, and no radiographic sign of healing, correction of the proximal femoral varus deformity and fixation of the cervical neck fracture was achieved by a cephalomedullary nail. At 8 months follow-up, hip pain relief was achieved with radiographic healing of the femoral neck stress fracture and the proximal femoral osteotomy.
Conclusion: A review of the literature was performed to identify any case report of femoral neck fractures fixation due to coxa vara in an adult. Both coxa vara and XLHR can cause femoral neck stress fracture. This study presented the surgical technique for treating a rare case of femoral neck stress fracture in a XLHR patient with coxa vara. Pain relief and bone healing were achieved by combined deformity correction and fracture fixation with a femoral cephalomedullary nail. The technique for deformity correction and cephalomedullary nail insertion in the patient with coxa vara is shown.
Keywords: X-linked hypophosphatemic rachitis, stress fracture, femoral neck fracture, coxa vara, adult, cephalomedullary nail.
X-linked hypophosphatemic rachitis (XLHR), with an incidence of 3.9/100,000 live births, is the most common cause of hereditary rickets [1]. The etiology of XLHR is mutations in the PHEX gene which generates high levels of fibroblast growth factor 23 (FGF23) causing a defective bone mineralization [2]. XLHR usually occurs in early years of life with bowing legs and short stature that lead to pain and difficulties in walking [3]. Hypophosphatemic ricket conventional treatment includes active vitamin D analogs and oral inorganic phosphate [4]. However, a new antibody drug against FGF23, burosumab, has shown through clinical trials that it is helpful for pediatric patients with XLHR, preventing lower limb deformity [5]. Considering the surgical treatment of adult patients with XLHR, few studies are available in the literature, highlighting the use of intramedullary fixation after realignment osteotomies which are effective for long healing times, and additionally, recurrence of deformity can be prevented in the long-term [6]. We present a rare case of XLHR with severe pain due to femoral neck stress fracture treated by mechanical axis correction and femoral cephalomedullary nail. SCARE guidelines were followed to report this case [7].
A 47-year-old male patient with known history of XLHR attended the outpatient clinic after severe left hip pain, which escalated gradually during the past 8 years. This pain was load-related, as well as initiation pain, and there was no related trauma. The clinical examination of the patient showed a positive Trendelenburg sign, moderately tight internal and external rotation, but good abduction and adduction. Previous surgery on the left femur included one midshaft corrective osteotomy in his adolescence, and the patient had been complaining about mild bilateral hip and spine pain for the past 15 years. The patient had no known allergies nor smoking history, height 178 cm, and BMI 27.1 kg/m2. The patient has been under continuous check up from an endocrinologist for XLHR. The X-ray revealed a left femoral neck stress fracture in conjunction with a varus deformity with the center of rotation of angulation (CORA) at the proximal femoral metaphysis (Fig. 1). The patient was followed for a month without restrictions in daily activities. After 1 month, there was no improvement of the pain, and no sign of healing was found (Fig. 2).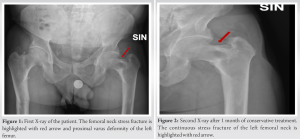 It was then decided to correct the proximal femoral varus deformity to ensure proper mechanical load of the femoral neck. The correction osteotomy was performed with a cephalomedullary nail allowing for screw fixation into the femoral neck and head. The surgical technique is presented in Fig. 3.
It was then decided to correct the proximal femoral varus deformity to ensure proper mechanical load of the femoral neck. The correction osteotomy was performed with a cephalomedullary nail allowing for screw fixation into the femoral neck and head. The surgical technique is presented in Fig. 3.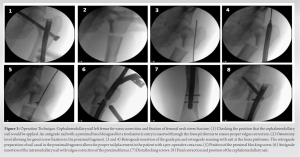 The patient was discharged 1 week postoperatively with the guidance to bear weight. Phosphate-A and vitamin D treatment was administered during the 3-month post-operative period. At 8 months follow-up, hip pain was relieved, while the femoral neck stress fracture and the proximal femoral osteotomy had radiographically healed. The follow up X-rays in 3 months (Fig. 4a) and in 8 months (Fig. 4b) show the bone healing.
The patient was discharged 1 week postoperatively with the guidance to bear weight. Phosphate-A and vitamin D treatment was administered during the 3-month post-operative period. At 8 months follow-up, hip pain was relieved, while the femoral neck stress fracture and the proximal femoral osteotomy had radiographically healed. The follow up X-rays in 3 months (Fig. 4a) and in 8 months (Fig. 4b) show the bone healing.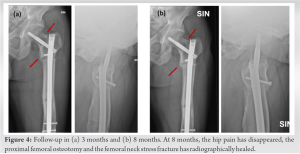
XLHR is an inheritable disorder that can lead to long bone deformities, requiring multiple surgical correction procedures. Surgical intervention is required for correction of the lower limb deformity in more than half of the patients with XLHR, with the complication rates of these surgeries being high [8]. A stable protection against recurrence of deformities is facilitated by the intramedullary nail, even if the patient develops metabolic decompensation postoperatively. One of the possible complications in the surgical treatment of XLHR adult patients is subsequent loss of correction or recurrence of the deformity. The patient presented in this case report had no complications and no loosening of the intramedullary nail. In general, when evaluating patients with stress fractures, other metabolic causes should also be ruled out, including eating disorders, hyperparathyroidism, and osteoporosis. In the presented case, the patient had no metabolic disease other than XLHR. The femoral neck stress fracture of the XLHR patient presented in this report was due to the proximal femoral varus deformity altering the mechanical load of the femoral neck. Coxa vara in hip is defined as the neck-shaft angle being below 120. Carpintero et al. [9] compared in a retrospective study 22 femoral stress fractures of the femoral neck between patients with coxa vara (12 patients) and without coxa vara (ten patients). Patients sustaining a femoral neck fracture and having coxa vara were younger and had longer duration of symptoms than patients without a coxa vara deformity suggesting that a focal concentration of mechanical stress in the femoral neck may have been produced due to coxa vara. A review of the literature was performed to identify any case report of femoral neck fractures fixation due to coxa vara in an adult, and the studies are presented in Table 1 [10,11,12,13,14,15] highlighting the different treatment options that were used in accordance with patients’ age and medical history. Three cases reported on femoral neck stress fractures in patients with coxa vara and osteomalacia. Tomar et al. treated the patient with total hip arthroplasty [15], while two cases report successful healing by valgus correction using either a 135 angulated plate [11] or a dynamic hip screw [13]. We could not find any previous studies demonstrating a combined valgus correction and cephalomedullary nail fixation.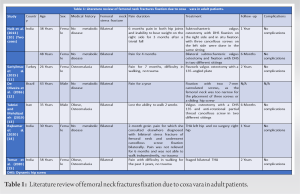
Both coxa vara and XLHR can cause femoral neck stress fracture. This study presented the surgical technique for treating a rare case of femoral neck stress fracture in a XLHR patient with coxa vara. Pain relief and bone healing were achieved by combined deformity correction and fracture fixation with a femoral cephalomedullary nail.
The possible cause leading to femoral neck stress fracture should always be taken in consideration when planning patient’s surgical treatment. Femoral cephalomedullary nail for combined deformity correction and fracture fixation is a treatment option in adult hypophosphatemic patients with coxa vara and a femoral neck stress fracture.
References
- 1.Rafaelsen S, Johansson S, Raeder H, Bjerknes R. Hereditary hypophosphatemia in Norway: A retrospective population-based study of genotypes, phenotypes, and treatment complications. Eur J Endocrinol 2016;174:125-36. [Google Scholar | PubMed]
- 2.Shimada T, Mizutani S, Muto T, Yoneya T, Hino R, Takeda S, et al. Cloning and characterization of FGF23 as a causative factor of tumor-induced osteomalacia. Proc Natl Acad Sci USA 2001;98:6500-5. [Google Scholar | PubMed]
- 3.Horn A, Wright J, Bockenhauer D, Van’t Hoff W, Eastwood DM. The orthopaedic management of lower limb deformity in hypophosphataemic rickets. J Child Orthop 2017;11:298-305. [Google Scholar | PubMed]
- 4.Carpenter TO, Imel EA, Holm IA, de Beur SM, Insogna KL. A clinician’s guide to X-linked hypophosphatemia. J Bone Miner Res 2011;26:1381-8. [Google Scholar | PubMed]
- 5.Imel EA, Glorieux FH, Whyte MP, Munns CF, Ward LM, Nilsson O, et al. Burosumab versus conventional therapy in children with X-linked hypophosphataemia: A randomised, active-controlled, open-label, phase 3 trial. Lancet 2019;393:2416-27. [Google Scholar | PubMed]
- 6.Eralp L, Kocaoglu M, Toker B, Balcı HI, Awad A. Comparison of fixator-assisted nailing versus circular external fixator for bone realignment of lower extremity angular deformities in rickets disease. Arch Orthop Trauma Surg 2011;131:581-9. [Google Scholar | PubMed]
- 7.Agha RZ, Borrelli MR, Farwana R, Koshy K, Fowler AJ, Orgill DP, et al. The SCARE 2018 statement: Updating consensus Surgical CAse REport (SCARE) guidelines. Int J Surg 2018;60:132-6. [Google Scholar | PubMed]
- 8.Paludan CG, Thomsen KK, Rahbek O, Kold S. Complications of orthopedic treatment in patients diagnosed with X-linked hypophosphatemic rickets. J Pediatr Endocrinol Metab 2022;35:1003-9. [Google Scholar | PubMed]
- 9.Carpintero P, Leon F, Zafra M, Serrano-Trenas JA, Román M. Stress fractures of the femoral neck and coxa vara. Arch Orthop Trauma Surg 2003;123:273-7. [Google Scholar | PubMed]
- 10.Naik MA, Sujir P, Tripathy SK, Vijayan S, Hameed S, Rao SK. Bilateral stress fractures of femoral neck in non-athletes: A report of four cases. Chin J Traumatol 2013;16:113-7. [Google Scholar | PubMed]
- 11.Sariyilmaz K, Ozkunt O, Sungur M, Dikici F, Yazicioglu O. Osteomalacia and coxa vara. An unusual co-existence for femoral neck stress fracture. Int J Surg Case Rep 2015;16:137-40. [Google Scholar | PubMed]
- 12.De Oliveira US, Labronici PJ, Neto AJ, Nishimi AY, Pires RE, Silva LH. Bilateral stress fracture of femoral neck in non-athlete-case report. Rev Bras Ortop 2016;51:735-8. [Google Scholar | PubMed]
- 13.Tabrizi A, Mehdizadeh M. Bilateral femoral neck stress fractures in a patient with severe coxa vara, morbid obesity and osteomalacia: A case report. Shafa Ortho J 2019;6:84431. [Google Scholar | PubMed]
- 14.Rajkumar N, Soundarrajan D, Dhanasekararaja P, Rajasekaran S. Failed internal fixation in bilateral femoral neck stress fracture salvaged with total hip arthroplasty: A report of two cases with literature review. Indian J Orthop 2020;54:83-6. [Google Scholar | PubMed]
- 15.Tomar L, Govil G, Dhawan P. Bilateral femoral neck stress fracture in an obese middle-aged female with osteomalacia and coxa-vara managed by simultaneous bilateral total hip arthroplasty. Cureus 2020;12:e11478. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Posterior Acetabular Wall Fracture Mimicking a Subcapital Femoral Neck Fracture on Plain Radiographs: A Diagnostic Pitfall and the Role of Intraoperative Fluoroscopy: A Case Report
August 1, 2026 Posterior Acetabular Wall Fracture Mimicking a Subcapital Femoral Neck Fracture on Plain Radiographs: A Diagnostic Pitfall and the Role of Intraoperative Fluoroscopy: A Case Report August 1, 2026 Platelet-Rich Plasma Augmentation of Osteosynthesis in Femoral Neck Fractures: A Prospective Comparative Study Demonstrating Accelerated Union and Improved Function
August 1, 2026 Platelet-Rich Plasma Augmentation of Osteosynthesis in Femoral Neck Fractures: A Prospective Comparative Study Demonstrating Accelerated Union and Improved Function July 1, 2026 Enhanced Stability in an Unstable Femoral Neck Fracture Using the Femoral Neck System with Two Additional Cannulated Cancellous Screws: A Case Report
July 1, 2026 Enhanced Stability in an Unstable Femoral Neck Fracture Using the Femoral Neck System with Two Additional Cannulated Cancellous Screws: A Case Report June 1, 2026 Cemented versus Uncemented Hemiarthroplasty in Femoral Neck Fractures: A Comparative Case Series Using Singh Index for Surgical Decision-Making
June 1, 2026 Cemented versus Uncemented Hemiarthroplasty in Femoral Neck Fractures: A Comparative Case Series Using Singh Index for Surgical Decision-Making