
TTC nailing is a safe and effective initial treatment method for fragility fractures of the ankle in patient populations who may not adhere to weight-bearing restrictions post-operatively.
Dr. Nolan P Schmitz, Department of Orthopedics, OhioHealth, Columbus, Ohio 43228, United States. E-mail: schm3524@umn.edu
Abstract
Introduction: Ankle fractures are a common orthopedic injury traditionally treated with open reduction and internal fixation or conservative management. One complication introduced with open reduction and internal fixation is the requirement for non or partial weight bearing in the post-operative period. This requirement poses a unique challenge for patients who may not comply with these weight-bearing restrictions. This case is the first known article that specifically illustrates the validity and effectiveness of retrograde tibiotalocalcaneal (TTC) nailing for patients who are unlikely to follow weight-bearing restrictions.
Case Report: An 83-year-old Caucasian female with idiopathic mild mental retardation and Alzheimer’s presented with a minimally displaced trimalleolar ankle fracture and was treated at a single urban hospital with a retrograde TTC nail secondary to her inability to adhere to weight-bearing restrictions post-operatively. Pertinent demographic, clinical, radiographic, and surgical data were collected. The patient had minimal post-operative pain, was able to bear weight on the day of surgery, and had no post-operative complications.
Conclusion: This case report demonstrates that the use of a TTC nail is a safe and effective mode of fixation for ankle fractures in patient populations who may not adhere to weight-bearing restrictions post-operatively. The main benefits of fixation with a TTC nail are the ability to weight bear as tolerated post-operatively and decreased wound complications while having similar functional outcomes to open reduction and internal fixation. We suggest the use of TTC nails for ankle fractures in select patients who may not adhere to weight-bearing restrictions post-operatively.
Keywords: Tibiotalocalcaneal nail, ankle fractures, ankle fracture weight-bearing precautions, ankle fracture weight-bearing non-adherence.
Ankle fractures are a common orthopedic injury with an incidence of 184 fractures per 100,000 per year with the most common mechanisms being falls or trauma [1] Historically, these fractures have been typically treated conservatively or through open reduction and internal fixation. Both treatment options require a period of immobilization and evidence of fracture healing before weight bearing. In recent years, there has been a significant increase in elderly fragility fractures of the ankle in elderly populations. In the literature regarding elderly fragility fractures, utilization of intramedullary fixation has been shown to be a successful option to allow immediate weight bearing with low complication rates [2,3,4]. While patient factors such as osteoporosis, age, soft-tissue envelope, and time to healing in elderly patients have been documented as indications for the use of a retrograde tibiotalocalcaneal (TTC) nail, there is a paucity of literature on it being an option for the elderly patient with an inability to follow weight-bearing restrictions as an indication for surgery. Adherence to treatment recommendations is an important factor in the shared decision-making model that we currently employ. We present the case of an 82-year-old patient with a trimalleolar ankle fracture ultimately treated with a TTC nail after determining she is unable to comply with weight-bearing restrictions. To our knowledge, there is a minimal description of this in the literature at the time of writing this manuscript.
An 82-year-old female patient with a past medical history of osteopenia as well as idiopathic mild mental retardation and dementia presented to a community hospital emergency department (ED) after turning her ankle 24 h before initial evaluation. Initial radiographs demonstrated a trimalleolar ankle fracture without dislocation with a large posterior malleolar fragment as shown in Figure 1. 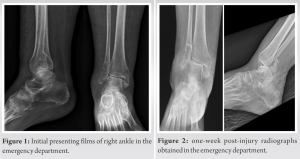 She was evaluated and placed into a well-padded three-sided splint by the on-call orthopedic resident and instructed to follow up in the orthopedic clinic within the next 5–7 days. Before this injury, the patient was ambulatory about the house and utilized a wheelchair otherwise. At the initial ED visit, she was instructed to remain non-weight bearing and to ice and elevate the extremity to alleviate swelling and pain. Exactly 1 week later, the patient was brought back to the ED due to increased pain to the right ankle. The same orthopedic resident re-evaluated her and noted significant damage to her splint. Radiographs at this point demonstrated that the patient had dislocated the tibiotalar joint while in the splint as shown in Figure 2. Inspection of the skin overlying the right ankle showed the development of serous-filled fracture blisters over the medial and lateral malleoli. The ankle was reduced and splinted by the orthopedic resident, and she was admitted to the hospital for pain control. Discussion with the patient and family revealed that she regularly was kicking a wall with her injured extremity and that they had significant difficulty with keeping her non-weight bearing. A discussion was had with the patient and family regarding treatment options with open reduction and internal fixation versus TTC nail. It was discussed that with TTC nail, there would be closed reduction and relative stability of the fracture with loss of range of motion of the ankle, but that the patient would be able to weight bear post-operatively with lower risk of hardware failure and loss of reduction requiring revision surgery [2].
She was evaluated and placed into a well-padded three-sided splint by the on-call orthopedic resident and instructed to follow up in the orthopedic clinic within the next 5–7 days. Before this injury, the patient was ambulatory about the house and utilized a wheelchair otherwise. At the initial ED visit, she was instructed to remain non-weight bearing and to ice and elevate the extremity to alleviate swelling and pain. Exactly 1 week later, the patient was brought back to the ED due to increased pain to the right ankle. The same orthopedic resident re-evaluated her and noted significant damage to her splint. Radiographs at this point demonstrated that the patient had dislocated the tibiotalar joint while in the splint as shown in Figure 2. Inspection of the skin overlying the right ankle showed the development of serous-filled fracture blisters over the medial and lateral malleoli. The ankle was reduced and splinted by the orthopedic resident, and she was admitted to the hospital for pain control. Discussion with the patient and family revealed that she regularly was kicking a wall with her injured extremity and that they had significant difficulty with keeping her non-weight bearing. A discussion was had with the patient and family regarding treatment options with open reduction and internal fixation versus TTC nail. It was discussed that with TTC nail, there would be closed reduction and relative stability of the fracture with loss of range of motion of the ankle, but that the patient would be able to weight bear post-operatively with lower risk of hardware failure and loss of reduction requiring revision surgery [2].  In comparison with open reduction and internal fixation, there would be anatomic reduction and absolute stability of the fracture with preserved ankle range of motion, but higher risk of hardware failure and loss of reduction requiring subsequent revision surgery if the patient were to weight bear post-operatively [3]. Ultimately, the family elected to proceed with the TTC nail due to its stability and durability and so that the patient could bear weight through the right lower extremity post-operatively. Intraoperative fluoroscopy images demonstrating near anatomic alignment of the tibiotalar joint are demonstrated in Figure 3. Post-operatively, the patient was placed into a bulky soft dressing and was given a walking boot without any weight-bearing restrictions. The remaining hospital course was uneventful, and she was discharged to home.
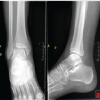
In comparison with open reduction and internal fixation, there would be anatomic reduction and absolute stability of the fracture with preserved ankle range of motion, but higher risk of hardware failure and loss of reduction requiring subsequent revision surgery if the patient were to weight bear post-operatively [3]. Ultimately, the family elected to proceed with the TTC nail due to its stability and durability and so that the patient could bear weight through the right lower extremity post-operatively. Intraoperative fluoroscopy images demonstrating near anatomic alignment of the tibiotalar joint are demonstrated in Figure 3. Post-operatively, the patient was placed into a bulky soft dressing and was given a walking boot without any weight-bearing restrictions. The remaining hospital course was uneventful, and she was discharged to home.  Two-week follow-up revealed the skin incisions to have nicely healed and the fracture blisters to have subsided. Radiographs shown in Figure 4 demonstrated maintained alignment and position of the implant without any complications. Eight-week follow-up revealed no skin complications and the patient was ambulatory without difficulty. Radiographs at this time demonstrate healed fractures in anatomic alignment as shown in Figure 5.
Two-week follow-up revealed the skin incisions to have nicely healed and the fracture blisters to have subsided. Radiographs shown in Figure 4 demonstrated maintained alignment and position of the implant without any complications. Eight-week follow-up revealed no skin complications and the patient was ambulatory without difficulty. Radiographs at this time demonstrate healed fractures in anatomic alignment as shown in Figure 5.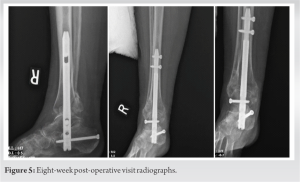
Ankle fractures in the elderly population with poor bone quality are commonly encountered. Ankle fractures are a common orthopedic injury with an incidence of 184 fractures per 100,000 per year with the most common mechanisms being falls or trauma [1]. Historically, these fractures have been typically treated non-operatively or through open reduction and internal fixation. There have been several case series published on the use of intramedullary implants for the fixation of fragility ankle fractures in the elderly population. Lemon et al. described a series of 12 patients treated with an expandable TTC nail and all patients went on to union [5]. All patients were able to bear weight immediately post-operatively, and all surgical wounds healed by 7 days. They conclude that it is a safe and effective treatment method that enables immediate weight bearing without the use of a cast. Similarly, Jonas et al. found in a retrospective review of 31 patients with a fragility fracture of the ankle treated with a TTC nail had. In a different prospective randomized control study done by Georginnos, Lampridis, and Bisbinas comparing TTC nailing versus open reduction and internal fixation of fragility fractures of the ankle in the elderly, it was found that there was a lower rate of mortality, less overall complications, and shorter hospital stays for patients who had their ankle fixed with a TTC nail [6]. A retrospective cohort study of 31 patients using a TTC nail for fragility ankle fractures showed similarly low complication rates [2]. The authors conclude that hindfoot nailing is safe and effective for ankle fracture treatment in patients with diabetes and peripheral neuropathy. Deep infection was an issue in this series, although the authors also included open fractures in this cohort which along with medical comorbidities can contribute significantly to these findings. In 2021, Lu et al. published their series of 20 patients who sustained a fragility ankle fracture and were treated with TTC nail [7]. Thirteen of their patients returned to their pre-operative functional level and all fractures went on to union. Their patient’s Charlson Comorbidity Index averaged 5.05, which correlates to a 10-year survival rate of 53%. These patients, therefore, had a high degree of medical complexity on top of their ankle fractures. Tan et al. also found that 81.5% of patients with unstable ankle fractures treated with primary TTC fusion were able to return to their pre-operative mobility level [8]. A third retrospective study done by Jonas et al. found that 29/31 patients with fragility fractures of the ankle treated with a TTC nail were able to return to the same level of mobility as pre-injury [9]. The ability to return to pre-operative functional level in most patients plays a significant role in the treatment of choice in these injuries. Our patient presented with this injury and within 10 days demonstrated additional concern of their ability to comply with weight-bearing restrictions. When contemplating treatment options and to uphold our duty as physicians to do no harm, ensuring a patient can comply and readily follow treatment recommendations must play a role in decision-making. In an article related to patient compliance and the ethics behind it, the authors state that “we are duty bound as clinicians to investigate the reasons for non-compliance and to intervene to minimize the risk of this happening again” [10]. Our patient had a known level of baseline dementia, as well as idiopathic mild mental retardation, which complicated her ability to follow weight-bearing restrictions. In combination with the literature supporting the safety and effectiveness of TTC nails in fragility fractures of the ankle, offering a procedure that would remove weight-bearing restrictions from this patient became the most reasonable way to protect the patient from further complications. There are several limitations to this study. This study represents one retrospective case review without a comparative study. With the nature of this study being a case report on one patient, it is a small sample size and further studies are needed to increase the validity of these findings. With the sample size being so small, the conclusions that can be drawn are limited, but this study is the first known in the current literature on the use of a TTC nail for ankle fragility fractures in populations who may not adhere to weight-bearing restrictions post-operatively.
Fragility fractures of the ankle are commonly encountered injuries that require special attention. In the case presented above, the patient’s ability to comply with a non-weight-bearing status became paramount to the decision for operative intervention. TTC nailing has been shown to be safe and effective at maintaining function in the elderly population and enables immediate weight bearing. We feel that in the case of elderly patients with memory issues, a TTC nail is a safe and effective treatment method that can alleviate the burden of concern for adherence to weight-bearing restrictions.
The use of a TTC nail is a safe and effective mode of initial fixation for ankle fractures in patient populations who may not adhere to weight-bearing restrictions post-operatively. The main benefits of fixation with a TTC nail are the ability to weight bear as tolerated post-operatively and decreased wound complications while having similar functional outcomes to open reduction and internal fixation.
References
- 1.Jordan RW, Chapman AW, Buchanan D, Makrides P. The role of intramedullary fixation in ankle fractures – A systematic review. Foot Ankle Surg 2018;24:1-10. [Google Scholar | PubMed]
- 2.Tarkin IS, Fourman MS. Retrograde hindfoot nailing for acute trauma. Curr Rev Musculoskelet Med 2018;11:439-44. [Google Scholar | PubMed]
- 3.Taylor BC, Hansen DC, Harrison R, Lucas DE, Degenova D. Primary retrograde tibiotalocalcaneal nailing for fragility ankle fractures. Iowa Orthop J 2016;36:75-8. [Google Scholar | PubMed]
- 4.Herrera-Pérez M, Martín-Vélez P, González-Martín D, Domínguez-Meléndez M, Galhoum AE, Valderrabano V, et al. Tibiotalocalcaneal nailing for osteoporotic ankle fractures in the frail patient: A narrative review with a clinical score proposal for the decision-making process. EFORT Open Rev 2022;7:328-36. [Google Scholar | PubMed]
- 5.Lemon M, Somayaji HS, Khaleel A, Elliott DS. Fragility fractures of the ankle: Stabilisation with an expandable calcaneotalotibial nail. J Bone Joint Surg Br 2005;87:809-13. [Google Scholar | PubMed]
- 6.Georgiannos D, Lampridis V, Bisbinas I. Fragility fractures of the ankle in the elderly: Open reduction and internal fixation versus tibio-talo-calcaneal nailing: Short-term results of a prospective randomized-controlled study. Injury 2017;48:519-24. [Google Scholar | PubMed]
- 7.Lu V, Tennyson M, Zhang J, Thahir A, Zhou A, Krkovic M. Ankle fusion with tibiotalocalcaneal retrograde nail for fragility ankle fractures: Outcomes at a major trauma centre. Eur J Orthop Surg Traumatol 2023;33:125-33. [Google Scholar | PubMed]
- 8.Tan YY, Nambiar M, Onggo JR, Hickey BA, Babazadeh S, Tay WH, et al. Tibio-Talar-calcaneal nail fixation for ankle fractures: A systematic review and meta-analysis. J Foot Ankle Surg 2021;S1067-2516. [Google Scholar | PubMed]
- 9.Jonas SC, Young AF, Curwen CH, McCann PA. Functional outcome following tibio-talar-calcaneal nailing for unstable osteoporotic ankle fractures. Injury 2013;44:994-7. [Google Scholar | PubMed]
- 10.Sciberras N, Gregori A, Holt G. The ethical and practical challenges of patient noncompliance in orthopaedic surgery. J Bone Joint Surg Am 2013;95:e61. [Google Scholar | PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2025 Chronic Syndesmotic Instability Associated with a Complex Lesion of the Posterior Inferior Tibiofibular Ligament: Review, Case Report, and Surgical Report
August 1, 2025 Chronic Syndesmotic Instability Associated with a Complex Lesion of the Posterior Inferior Tibiofibular Ligament: Review, Case Report, and Surgical Report September 1, 2024 Posterior Cruciate Ligament Avulsion Fracture of Tibia: Fixation with Screw and Augmentation Using Ethibond Suture for Improved Clinical Outcomes
September 1, 2024 Posterior Cruciate Ligament Avulsion Fracture of Tibia: Fixation with Screw and Augmentation Using Ethibond Suture for Improved Clinical Outcomes November 10, 2023 Peroneal Artery Pseudoaneurysm after Surgery for Non-union of Tibia: A Case Report with Review of Literature
November 10, 2023 Peroneal Artery Pseudoaneurysm after Surgery for Non-union of Tibia: A Case Report with Review of Literature October 6, 2019 Epithelioid Osteoblastoma of the Proximal Femur in a 19-Year-Old Female: A Case Report and Review of Literature
October 6, 2019 Epithelioid Osteoblastoma of the Proximal Femur in a 19-Year-Old Female: A Case Report and Review of Literature