
Classification of Monteggia fracture dislocation is as significant as to diagnose. Treatment strategies may change according to the type of injury.
Dr. Alparslan Uzun, Department of Orthopaedics and Traumatology, Istanbul Medipol University, School of Medicine, TEM Avrupa Otoyolu, Göztepe Çıkışı No: 1, 34214, Bağcılar, Istanbul, Turkey. E-mail: dralparslanuzun@gmail.com
Abstract
Introduction: Monteggia fracture dislocations are relatively common and debilitating traumas in <10 years of age. This is the second case reporting Monteggia type 3 equivalent injury treated by the same way while the first being reported also by our team in 2016.
Case Report: A 4-year-old Caucasian male patient was admitted to our clinic by his parents at the day after his fall. A long arm splint was applied with the diagnosis of Monteggia fracture dislocation in another hospital.
Conclusion: Bado introduced his classification system for Monteggia fracture dislocations in 1967. This classification system is mainly based on the direction of dislocation of the radial head. If radial head dislocated laterally with an accompanying ulnar fracture it is classified as Bado type 3 while type 4 is the anterior dislocation of the radial head accompanied with both bone forearm fracture. The unusual fracture dislocation pattern in our case is that lateral dislocation of the radial head is accompanied with both bone forearm fracture, which is an example to be named as Monteggia type 3 equivalent lesion. Closed reduction was not successful to reduce radial head. To reduce the radial head, we used an intramedullary Kirschner and a long arm splint was applied to ensure the safety of the reduction. There was no restriction in elbow movements and the result of the operation was successful.
Keywords: Monteggia fracture, bado classification, radius dislocation, ulna fracture.
The Monteggia injury is the dislocation of the radial head with an associated fracture of the ulna [1]. It is known as its hard to diagnose but easy to treat nature [2]. Physical examination and radiographic imaging should be the first step in evaluation. Bado introduced his classification system for Monteggia fracture-dislocations in 1967 (Table 1) [3]. There are also different subtypes mentioned in literature. However, this is the second type 3 equivalent case reporting that laterally dislocated radial head with accompanying both bone forearm fractures treated in the same way, while the first case was also introduced by us in 2016 [2].
A 4-year-old male presented in our outpatient clinic with a long arm splint at the day after his fall. At first, his parents had taken him to another hospital where he has given the initial treatment as closed reduction and long arm splint. In our examination, capillary refill was good, there was no sign of compartment syndrome. The family was informed that the child might have the diagnosis of Monteggia fracture but we could not reach the radiographs. We took true radiographs of both arms (Fig. 1) to look for any other pathology involving elbow and wrist joints. Both forearm bones were fractured and radial head was still dislocated laterally, despite the reduction done in the first attended clinic. In Monteggia fracture dislocation, lateral dislocation of radial head is typically seen with ulna fracture in Bado type 3 while both bone forearm fracture normally exists with anterior displacement of radial head in Bado type 4 [2]. The Bado classification system is primarily based on the direction of radial head dislocation. Therefore, we considered it as a Monteggia type III equivalent lesion and planned to do closed reduction with or without internal fixation under general anesthesia.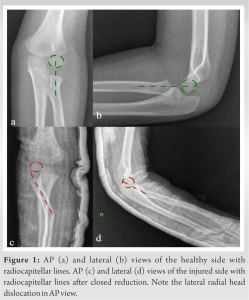
Treatment
In operation, we tried closed reduction at first. Displacement of both fractures has decreased but the radial head could not been relocated. Hence, we decided to do internal fixation. We implanted an intramedullary K-wire into the radius from it’s distal tip.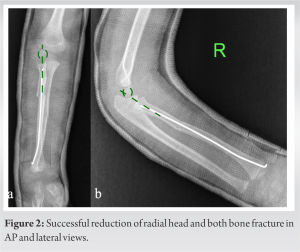 Intraoperative fluoroscopy images proved the radial head reduction and ulna fracture to be stable. Then, we applied a long arm splint and end the operation. Post-operative X-rays showed successful reduction of both bone fractures along with the radial head (Fig. 2). His splint has removed 3 weeks after operation and active motion was allowed thereafter. Post-operative radiographs were obtained in 2nd week, 4th week, and 2nd month. No displacement has been noticed in follow-ups. In the 8th week of operation, intramedullary K-wire was removed intraoperatively (Fig. 3). His elbow and wrist movements showed no restrictions. There were no sensory or motor deficits.
Intraoperative fluoroscopy images proved the radial head reduction and ulna fracture to be stable. Then, we applied a long arm splint and end the operation. Post-operative X-rays showed successful reduction of both bone fractures along with the radial head (Fig. 2). His splint has removed 3 weeks after operation and active motion was allowed thereafter. Post-operative radiographs were obtained in 2nd week, 4th week, and 2nd month. No displacement has been noticed in follow-ups. In the 8th week of operation, intramedullary K-wire was removed intraoperatively (Fig. 3). His elbow and wrist movements showed no restrictions. There were no sensory or motor deficits.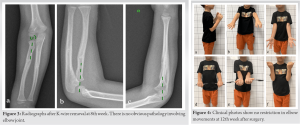
Outcome and follow-up
We discharged the patient on the day after surgery. We followed him for 12 weeks. At the 8th week, intramedullary K-wire has been removed. The examination on 12th week shows no restriction in elbow movements (Fig. 4).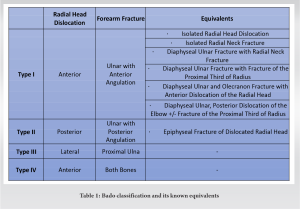
Monteggia injury is an uncommon pathology. These injuries are challenging for both diagnosis and treatment. It requires a comprehensive approach consisting of good quality radiographs and proper clinical examination. The delay in diagnosis is still reported as a major issue [4]. Compared to original types, undefined Monteggia lesions (like the one we have described in our case) are harder to recognize and treat. Therefore, it is important to examine the X-rays of patients with forearm fractures in detail regardless of the broken bone, especially including an upper and a lower joint. Samples of undefined Monteggia lesions may help orthopedic surgeons to make a better and quicker diagnosis in the future. Therefore, it is important for orthopedic surgeons to careful evaluation and interpretation of radiographs in a patient with a forearm fracture, regardless of the fractured bone. Emergent orthopedic consultation is essential for open fractures and vascular compromise. Urgent orthopedic consultation is indicated for neurologic deficits without vascular compromise [5,6,7]. According to Bado’s description, Monteggia injury consists of radial head dislocation and fracture of the ulna at various levels. Bado classification system is mainly based on the direction of dislocation of the radial head. If ulnar fracture accompanies with lateral radial head dislocation, it is classified as Bado type 3 while type 4 is anterior displacement of radial head existing with both bone forearm fractures. He also enriched his classification system to include some unusual varieties, in which he called “equivalents” or “Monteggia-like lesions [8].” However, no subtypes of this classification system have encompassed the variant described above where both bone is fractured and radial head is dislocated. This unusual pattern in our case is an example to be named as Monteggia type 3 equivalent lesion. This is the second case reporting this type of injury treated by the same way while the first being reported also by our team in 2016 [2]. Treatment begins with closed reduction. If closed reduction fails, then an open reduction is required. According to Metaizeau et al., one way to reduce the radial head fracture is to insert a curved K-wire through the distal radial metaphysis until the tip seats in the epiphysis, thereby reducing radial head fracture [9]. We performed this technique in our patient. No complications have been noticed in our follow-ups. The patient is symptom free and does not have any restrictions as indicated above.
Physical examination and radiographic imaging should be the first step in evaluation for Monteggia fracture dislocations. Direction of the radial head dislocation is the primary attribute of the classification. If ulnar fracture accompanies with lateral radial head dislocation, it is classified as Bado type 3 while type 4 is anterior displacement of radial head existing with both bone forearm fractures [10]. The unusual fracture dislocation pattern in our case where both bone fracture is associated with lateral dislocation of the radial head is an example to be named as Monteggia type 3 equivalent lesion. Treatment begins with closed reduction. Operative treatment is indicated if radial head cannot be reduced by closed reduction. In our case, by closed reduction, displacement of both fractures has decreased but the radial head could not been relocated. Hence, we decided to do internal fixation. Intramedullary K-wires can be used to successfully reduce radial head.
According to Bado Classification, there is no subtype indicating lateral dislocation and both bone fractures. Because it is unusual, it is quite possible for clinicians to miss this type of pathology. If the diagnosis is missed, there is a high probability of permanent joint damage. It is important to be aware of this condition. This is one of the very few articles reporting this type of injury and its treatment.
References
- 1.Bailey DA, Wedge JH, McCulloch RG, Martin AD, Bernhardson SC. Epidemiology of fractures of the distal end of the radius in children as associated with growth. J Bone Joint Surg Am 1989;71:1225-31. [Google Scholar | PubMed]
- 2.Kara A, Kayaalp ME, İşyar M, Sever C, Malkoç M, Mahiroğulları M. An undescribed monteggia Type 3 equivalent lesion: Lateral dislocation of radial head with both-bone forearm fracture. Case Rep Orthop 2016;2016:8598139. [Google Scholar | PubMed]
- 3.Ruchelsman DE, Klugman JA, Madan SS, Chorney GS. Anterior dislocation of the radial head with fractures of the olecranon and radial neck in a young child: A monteggia equivalent fracture-dislocation variant. J Orthop Trauma 2005;19:425-8. [Google Scholar | PubMed]
- 4.Dolan M, Waters PM. Fractures and dislocations of the forearm, wrist, and hand. In: Green NE, Swiontkowski MF, editors. Skeletal Trauma in Children. Philadelphia, PA, USA: Elsevier Saunders; 2009. p. 182-4. [Google Scholar | PubMed]
- 5.Eamsobhana P, Chalayon O, Kaewpornsawan K, Ariyawatkul T. Missed monteggia fracture dislocations treated by open reduction of the radial head. Bone Joint J 2018;100-B:1117-24. [Google Scholar | PubMed]
- 6.Yoshida N, Tsuchida Y. Posterior interosseous nerve palsy due to Bado Type-III Monteggia fracture. BMJ Case Rep. 2018 Jul 30;2018:bcr2018226254. doi: 10.1136/bcr-2018-226254. PMID: 30061146; PMCID: PMC6069943. [Google Scholar | PubMed | CrossRef]
- 7.Hubbard J, Chauhan A, Fitzgerald R, Abrams R, Mubarak S, Sangimino M. Missed pediatric monteggia fractures. JBJS Rev 2018;6:e2. [Google Scholar | PubMed]
- 8.Santoso AR, Huwae TE, Wijaya AE, Pribadi A, Cendikiawan F, Abduh M. Treatment of monteggia-like-lesion in a young patient: A case report. Medicine (Baltimore) 2021;100:e24298. [Google Scholar | PubMed]
- 9.Metaizeau JP, Lascombes P, Lemelle JL, Finlayson D, Prevot J. Reduction and fixation of displaced radial neck fractures by closed intramedullary pinning. J Pediatr Orthop 1993;13:355-60. [Google Scholar | PubMed]
- 10.Rehim SA, Maynard MA, Sebastin SJ, Chung KC. Monteggia fracture-dislocations: A historical review. J Hand Surg Am 2014;39:1384-94. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2025 Triple Traumatic Fracture-Dislocation: A Rare Case of Simultaneous Ipsilateral Hip, Knee, and Ankle Fracture-Dislocation with a Review of the Literature
August 1, 2025 Triple Traumatic Fracture-Dislocation: A Rare Case of Simultaneous Ipsilateral Hip, Knee, and Ankle Fracture-Dislocation with a Review of the Literature July 10, 2016 How much Literature Review is enough for a Case Report?
July 10, 2016 How much Literature Review is enough for a Case Report? October 9, 2012 Flowerpot sequestrum of the Humerus Neglect for 10 years!!
October 9, 2012 Flowerpot sequestrum of the Humerus Neglect for 10 years!! August 1, 2026 Successful Salvage of Infected Tibial Shaft Non-union After Implant Removal with Ilizarov External Fixation: A Case Report
August 1, 2026 Successful Salvage of Infected Tibial Shaft Non-union After Implant Removal with Ilizarov External Fixation: A Case Report