
In every case of a terrible triad, we should be mindful of the possibility of a tear in the triceps tendon, which may be the cause of elbow instability.
Dr. Meisam Jafari Kafiabadi, Department of Orthopedic Surgery, Shohada-e Tajrish Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran. E-mail: meisamjafarikafiabadi@gmail.com
Abstract
Introduction: The terrible triad of the elbow includes an elbow dislocation or subluxation with coronoid and in combination with radial head fractures. Still, none of them are accompanied by rupture of the triceps tendon.
Case Report: The article describes a terrible triad injury in a young patient with an additional triceps rupture. The treatment involved lateral and medial approaches for the repair of various ligaments and fractures, but the elbow remained unstable. A posterior approach was used to repair the triceps rupture.
Conclusion: Triceps tendon rupture may be accompanied by dribble triad injuries, highlighting the importance of pre-operative evaluation to select the most appropriate surgical approach. The selection of an optimal surgical approach is crucial for the successful treatment and management of these injuries.
Keywords: Elbow, terrible triad, fracture, dislocation, triceps tendon, tear.
The terrible triad of the elbow was described by Hotchkiss in 1966 [1], including an elbow dislocation or subluxation with coronoid and in combination with radial head fractures. Still, none of them are accompanied by rupture of the triceps tendon [2]. Nerve injury, wound healing issues, heterotopic ossification, stiffness, non-union, malunion, infection, and instability are complications [3,4]. The elbow joint is highly congruent and stable; even a small amount of residual irregularity may cause poor outcomes [5]. This article reports a case with a terrible triad of the elbow, rupture of the triceps muscle, ipsilateral scaphoid, and distal radius fracture. Our goal is to increase attention to such injuries and the necessity of evaluating clinical and radiological images for additional injuries, such as flake signs so that with the best treatment, the best clinical performance and stability of the elbow can be obtained.
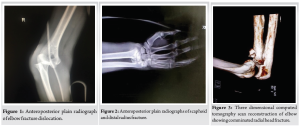
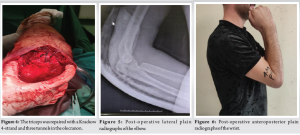
A 25-year-old male presented to the emergency department with pain and swelling in his right elbow and wrist following a fall on his right hand from a height. The patient had no significant medical, family, or drug history. On examination, the patient had deformity and tenderness in his right elbow and wrist, with ecchymosis present around the elbow but no open wounds. The neurovascular examination was intact. Radiographs revealed a posterolateral elbow fracture-dislocation (Fig. 1), a distal radius fracture, and a scaphoid waist fracture (Fig. 2). A closed reduction was performed for the elbow under intravenous sedation, and a long arm splint was applied. A computed tomography scan revealed a coronoid fracture and a highly comminuted radial head fracture (Fig. 3). Surgery was performed the next day. The radial head was resected through Kocher’s approach, and the lateral collateral ligament was repaired with an anchor suture. In the next step, due to the elbow’s instability shown in the clinical examination, a medial approach was used to transpose the ulnar nerve to the anterior of the epicondyle. Additionally, the medial collateral ligament was repaired using a trans-osseous technique. During the clinical examination, it was found that the elbow was still unstable. Here, we decided to implant an external fixator but suddenly noticed a gap posterior to the elbow during the palpation. The posterior midline approach revealed a ruptured triceps in its tendinous part. The triceps were repaired with a Krackow 4-strand and three tunnels in the olecranon (Fig. 4). Finally, the elbow joint was found to be stable both clinically and radiologically (Fig. 5), with no limitation of flexion-extension and pronation-supination. In the same surgery, the distal radius fracture was fixed with open reduction and internal fixation by a volar locking plate and three pins. The scaphoid fracture was fixed with a Herbert screw in an open method (Fig. 6). After surgery, the elbow was immobilized in 90° of flexion and neutral forearm rotation for 3 weeks, followed by progressive passive extension and active assisted elbow flexion. The patient started working on a range of motion (ROM) and stretching with the help of a physiotherapist. The distal radius fracture pins were removed after 6 weeks, and active extension of the triceps was initiated after 3 months. Valgus and Varus force was prohibited for the first 3 months due to the terrible triad injury. After 4 months, the patient’s ROM was complete (Fig. 7 and 8 ).

In cases of terrible triad elbow injuries, it is not possible to reliably test elbow extension strength. Therefore, to diagnose a triceps rupture before surgery, we rely on bony radiologic findings called the “flake sign.” This sign appears as a small fragment of bone that has separated from the olecranon, indicating a triceps tendon avulsion [6]. In some cases, triceps muscle ruptures may not exhibit the “flake sign” on radiologic imaging. Although magnetic resonance imaging can also be used to diagnose triceps muscle ruptures, it may not be cost-effective to perform this imaging for every patient with a terrible triad elbow injury [3-5].Just as it can be challenging to diagnose a rotator cuff tear in the setting of a shoulder fracture dislocation or a patellar tendon tear in the context of a knee dislocation, it can also be difficult to diagnose a triceps tear in this situation [7]. These complex injuries often require a careful and comprehensive evaluation, which may include a combination of clinical examination and imaging studies [8-11]. In cases where a triceps avulsion is suspected or confirmed, prompt and appropriate treatment is necessary to prevent long-term complications and ensure optimal outcomes for the patient [4,5,10,12]. The triceps avulsion must be surgically treated to provide maximum stability to the joint and maintain a functional elbow. The instability is much more than what usually exists in a terrible triad of elbow injuries singly [12]. Also, radial head resection in Terrible Triad will have acceptable results if the interosseous membrane is intact and patients have an acceptable ROM [13].
Triceps tendon rupture may be accompanied by terrible triad injuries, highlighting the importance of pre-operative evaluation to select the most appropriate surgical approach. The selection of an optimal surgical approach is crucial for the successful treatment and management of these injuries.
The authors of this article recommend that in every patient with a terrible triad injury before surgery, attention should be paid to the triceps rupture.
References
- 1.Hotchkiss RN. Fractures and Dislocations of the Elbow. Fractures in Adults. Philadelphia, PA: Lippincott-Raven; 1996. p. 929-1024. [Google Scholar | PubMed]
- 2.Ebrahimzadeh MH, Amadzadeh-Chabock H, Ring D. Traumatic elbow instability. J Hand Surg 2010;35:1220-5. [Google Scholar | PubMed]
- 3.Dodds SD, Fishler T. Terrible triad of the elbow. Orthop Clin 2013;44:47-58. [Google Scholar | PubMed]
- 4.Mathew PK, Athwal GS, King GJ. Terrible triad injury of the elbow: Current concepts. J Am Acad Orthop Surg 2009;17:137-51. [Google Scholar | PubMed]
- 5.Ring D, Jupiter JP, Zilberfarb J. Posterior dislocation of the elbow with fractures of the radial head and coronoid. J Bone Joint Surg Am 2002;84:547-51. [Google Scholar | PubMed]
- 6.Pina A, Garcia I, Sabater M. Traumatic avulsion of the triceps brachii. J Orthop Trauma 2002;16:273-6. [Google Scholar | PubMed]
- 7.Dehghani Nazhvani HR, Bemani Lirgeshasi S, Bahari M. Terrible triad elbow fracture dislocation with ipsilateral triceps avulsion and radial shaft fracture: A case report. JBJS Case Connect 2020;10:e20.00308. [Google Scholar | PubMed]
- 8.Garrigues GE, Wray WH 3rd, Lindenhovius AL, Ring DC, Ruch DS. Fixation of the coronoid process in elbow fracture-dislocations. JBJS 2011;93:1873-81. [Google Scholar | PubMed]
- 9.Leigh WB, Ball CM. Radial head reconstruction versus replacement in the treatment of terrible triad injuries of the elbow. J Shoulder Elbow Surg 2012;21:1336-41. [Google Scholar | PubMed]
- 10.Rodriguez-Martin J, Pretell-Mazzini J, Andres-Esteban EM, Larrainzar-Garijo R. Outcomes after terrible triads of the elbow treated with the current surgical protocols. A review. Int Orthop 2011;35:851-60. [Google Scholar | PubMed]
- 11.Watters TS, Garrigues GE, Ring D, Ruch DS. Fixation versus replacement of radial head in terrible triad: Is there a difference in elbow stability and prognosis? Clin Orthop Relat Res 2014;472:2128-35. [Google Scholar | PubMed]
- 12.Lindenhovius AL, Jupiter JB, Ring D. Comparison of acute versus subacute treatment of terrible triad injuries of the elbow. J Hand Surg 2008;33:920-6. [Google Scholar | PubMed]
- 13.Najd Mazhar F, Ebrahimi H, Jafari D, Mirzaei A. Comparison of radial head resection with radial head fixation in the terrible triad injury of the elbow. J Res Orthop Sci 2019;6:19-24. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 December 1, 2025 Engagement of the Radial Head in Posterior Capitellum Fracture: Defining the Critical Point
December 1, 2025 Engagement of the Radial Head in Posterior Capitellum Fracture: Defining the Critical Point January 1, 2025 Open Ankle Injury without Associated Fracture or Dislocation Requiring Surgical Intervention: A Case Report
January 1, 2025 Open Ankle Injury without Associated Fracture or Dislocation Requiring Surgical Intervention: A Case Report July 10, 2024 Management of Bilateral Posterior Sternoclavicular Joint Dislocation: A Case Report
July 10, 2024 Management of Bilateral Posterior Sternoclavicular Joint Dislocation: A Case Report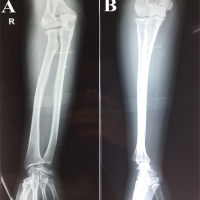 December 10, 2023 Neglected Elbow Dislocation leading to Ankylosis of Elbow: A Case Report
December 10, 2023 Neglected Elbow Dislocation leading to Ankylosis of Elbow: A Case Report