
Brodie’s abscess is a form of chronic pyogenic osteomyelitis that can be difficult to diagnose, particularly in rare locations. CT scans are helpful in diagnosing Brodie’s abscesses in hospitals with limited resources.
Dr. El Mouloua Ahmed, Paediatric Surgery Unit, Sidi Mohamed Ben Abdellah Hospital, Essaouira, Morocco. E-mail: elmouloua.ahmed@gmail.com
Abstract
Introduction: Brodie’s abscess is a form of localized sub-acute osteomyelitis that rarely occurs in the humerus. Its diagnosis stems from clinical, laboratory, and imaging findings, especially magnetic resonance imaging (MRI). The current paper describes the first case in the literature of humeral paddle Brodie’s abscess.
Case Report: This report describes the first case of Brodie’s abscess in the humeral paddle of a 12-year-old boy, revealed by swelling and pain in the right elbow. Radiographs and computerized tomography (CT) scans showed a well-defined cavitary surrounded by a rim of sclerosis, alongside evidence of cortical expansion and periosteal reaction. The patient was treated with debridement and curettage of the cavity combined with antibiotics. They resulted in the complete disappearance of the cavity. After 1 year of follow-up, the patient can practice daily activities with no pain, and imaging showed no signs of recurrence.
Conclusion: The present case highlights the utility of CT scans in diagnosing Brodie’s abscesses when an MRI is either unavailable or contraindicated. CT scans serve as a valuable alternative diagnostic modality in such cases.
Keywords: Brodie’s abscess, humeral paddle, children, computerized tomography scan, case report.
Brodie’s abscess is a primary subacute pyogenic osteomyelitis with milder clinical features than the acute form. It is characterized by an infection within the myelum, surrounded by a sclerotic wall, resulting in little systemic inflammatory response. Sir Benjamin Brodie first described it in 1832 [1]. The metaphysis is the region most prone to infection in long bones due to its abundant supply of slow-flowing blood, creating an ideal environment for bacteria to accumulate and proliferate [2]. In some cases, the specific location of Brodie’s abscess may lead to a delayed diagnosis and subsequent complications. It is important to consider differential diagnoses such as tuberculosis, Ewing sarcoma, and osteoid osteoma. We present the first case in the literature of Brodie’s abscess in the humeral occurring in a 12-year-old boy diagnosed on a computerized tomography (CT) scan with good outcomes after treatment.
A 12-year-old boy was presented to the emergency department with complaints of pain and swelling in his right elbow for the 3 weeks prior. With no recent trauma reported, the patient had a fever in the first 3 days; However, he had no history of weight loss, loss of appetite, cough, or surgical history. On physical examination, there was a slightly painful swelling on the right elbow, fluctuant on palpation. The skin’s local temperature was normal. There was no visible wound, hematoma, scar, or sinus. There was a painful restriction of the range of movements over the right elbow. A plain radiograph of the right elbow indicated a well-defined cavitary, osteolytic lesion surrounded by a rim of sclerosis and evidence of cortical expansion and periosteal reaction in the humeral paddle (Fig. 1). The differential diagnoses of Brodie’s abscess, tubercular abscess, and eosinophilic granuloma were considered. Magnetic resonance imaging (MRI) was not available in our institution. A CT scan showed a radiolucent lesion of the distal part of the humeral paddle measuring 1.5 × 1 cm, with sclerotic cortex thickening and mild joint effusion (Fig. 2).
The differential diagnoses of Brodie’s abscess, tubercular abscess, and eosinophilic granuloma were considered. Magnetic resonance imaging (MRI) was not available in our institution. A CT scan showed a radiolucent lesion of the distal part of the humeral paddle measuring 1.5 × 1 cm, with sclerotic cortex thickening and mild joint effusion (Fig. 2). Laboratory investigations showed an average white blood count, a raised C-reactive protein of 15 mg/dL, and an elevated erythrocyte sedimentation rate of 20 mm/h (the normal range is <10 mm/h). According to the clinical, radiological, and laboratory findings, we diagnosed Brodie’s abscess of the humeral paddle. The patient was taken to the operating room and underwent surgery. A tourniquet was used on the right arm after the elevation of the extremity for approximately 5 min. A lateral skin incision was made over the osteolytic lesion in the distal humerus. There was no cortical bone defect. Multiple samples were sent for microbiology and histology. The lytic lesion was reached by blunt dissection under the guidance of the C-arm fluoroscopic image intensifier. No frank purulence was noted. The cavity was curetted until the healthy bleeding bone was exposed and then rinsed with saline and hydrogen peroxide. Then, a closed-suction drain was left in the cavity. Intravenous amoxicillin and acid clavulanic 4 g/day were administrated. The right upper arm was held in place by a long arm cast for 3 weeks. The post-operative hospital course was uneventful. The closed-suction drain was removed on the 2nd day, and the patient was discharged and given an oral antibiotic on the 3rd post-operative day. The aerobic and anaerobic cultures were negative, and microbiological testing did not reveal any acid-fast bacillus. Blood analyses were normal. Histopathologic staining did not show any malignant cells. After a 5-month follow-up, the patient had a full range of motion, no swelling or pain, and the plain radiograph was normal (Fig. 3).
Laboratory investigations showed an average white blood count, a raised C-reactive protein of 15 mg/dL, and an elevated erythrocyte sedimentation rate of 20 mm/h (the normal range is <10 mm/h). According to the clinical, radiological, and laboratory findings, we diagnosed Brodie’s abscess of the humeral paddle. The patient was taken to the operating room and underwent surgery. A tourniquet was used on the right arm after the elevation of the extremity for approximately 5 min. A lateral skin incision was made over the osteolytic lesion in the distal humerus. There was no cortical bone defect. Multiple samples were sent for microbiology and histology. The lytic lesion was reached by blunt dissection under the guidance of the C-arm fluoroscopic image intensifier. No frank purulence was noted. The cavity was curetted until the healthy bleeding bone was exposed and then rinsed with saline and hydrogen peroxide. Then, a closed-suction drain was left in the cavity. Intravenous amoxicillin and acid clavulanic 4 g/day were administrated. The right upper arm was held in place by a long arm cast for 3 weeks. The post-operative hospital course was uneventful. The closed-suction drain was removed on the 2nd day, and the patient was discharged and given an oral antibiotic on the 3rd post-operative day. The aerobic and anaerobic cultures were negative, and microbiological testing did not reveal any acid-fast bacillus. Blood analyses were normal. Histopathologic staining did not show any malignant cells. After a 5-month follow-up, the patient had a full range of motion, no swelling or pain, and the plain radiograph was normal (Fig. 3).
Brodie’s abscess is a type of localized sub-acute osteomyelitis. Its prevalence varies between 2.5% and 42% of primary bone infections. The presumed cause of this condition is likely due to the low virulence of the infecting organism and the host’s resistance. Brodie’s abscess commonly affects the metaphysis of the femur or tibia in the lower extremities due to the blood flow characteristics of its sinusoids. The incidence of humerus involvement is low, ranging from 4.6% to 8.1% [2,3]. When the bone abscess is juxta-articular localization, it can cause muscle spasms and intermittent articular hydrops [3], as in our case.
The clinical symptoms are not specific. Most often, patients present pain, swelling, and warmth, while others remain asymptomatic. Blood analysis to detect an inflammatory response is usually within normal limits. However, an erythrocyte sedimentation rate >55 mm/h highly suggests an abscess [3]. Brodie’s abscess can present a diagnostic challenge when occurring in rare localization. Subacute osteomyelitis can mime other bone pathological features, such as Ewing sarcoma, tuberculosis, Langerhans cell histiocytosis, chondrosarcoma, eosinophilic granuloma, osteoid osteoma, and aneurysmal bone cyst [4,5]. Plain radiographs often present a well-circumscribed bony lucency lesion with sclerotic margins. There can also be marked cortical destruction, a disorganized trabecular pattern, and ill-defined bony lucencies. CT has a superior bony resolution to MRI and is better at demonstrating osseous changes; however, the evaluation of osteomyelitis with CT is limited with its poorer soft-tissue resolution compared to MRI [2]. MRI offers high sensitivity. The “penumbra sign” of Brodie’s abscess, as described by Gery et al. [6], is the characteristic finding of MRI. When malignancy cannot be excluded from blood analysis and imaging, a biopsy can be performed. In this case, even with the unavailability of an MRI, the physical examination of the patient, the blood tests, and the CT scan were sufficient to confirm the diagnosis of Brodie’s abscess. Staphylococcus species are the most common pathogens isolated after culture of Brodie’s abscess; They are isolated between 30% and 60% of cases, followed by Streptococcus and Kingella, and less commonly, Pseudomonas, Salmonella, Escherichia, and Haemophilus influenzae type b, whereas 25% of the cultures are sterile [6,7]. There are controversies regarding the management of Brodie’s abscess. Some authors recommend surgical intervention for diagnostic and therapeutic reasons, with aggressive debridement, curettage of the cavity, and, when needed, a bone graft for defects over 3 cm [5,8,9]. Others suggest surgical debridement only for patients who do not respond to antibiotic treatment or show aggressive radiologic features, with a preference for antibiotics as the sole treatment option [8,10]. In our opinion, we believe that surgical debridement with curettage and drainage followed by intravenous antibiotics is the cornerstone of the management of Brodie’s abscess. We could not find any published literature reviews describing a similar case. To the best of our knowledge, this is the first report of Brodie’s abscess of the humeral paddle in children.
Brodie’s abscess is rare in humeral paddle and may not be recognized early. CT scan remains a valuable alternative to diagnosing Brodie’s abscess when the MRI is unavailable or contraindicated.
The CT scan is a valuable alternative to diagnosing Brodie’s abscess when the MRI is unavailable or contraindicated.
References
- 1.Brodie BC. An account of some cases of chronic abscess of the Tibia. Med Chir Trans 1832;17:239-49. [Google Scholar | PubMed]
- 2.Lee YJ, Sadigh S, Mankad K, Kapse N, Rajeswaran G. The imaging of osteomyelitis. Quant Imaging Med Surg 2016;6:184-98. [Google Scholar | PubMed]
- 3.Connolly SA, Connolly LP, Drubach LA, Zurakowski D, Jaramillo D. MRI for detection of abscess in acute osteomyelitis of the pelvis in children. AJR Am J Roentgenol 2007;189:867-72. [Google Scholar | PubMed]
- 4.Rajakulendran K, Picardo NE, El-Daly I, Hussein R. Brodie’s abscess following percutaneous fixation of distal radius fracture in a child. Strategies Trauma Limb Reconstr 2016;11:69-73. [Google Scholar | PubMed]
- 5.Van der Naald N, Smeeing DP, Houwert RM, Hietbrink F, Govaert GA, Van der Velde D. Brodie’s abscess: A systematic review of reported cases. J Bone Jt Infect 2019;4:33-9. [Google Scholar | PubMed]
- 6.Agarwal S, Akhtar MN, Bareh J. Brodie’s abscess of the cuboid in a pediatric male. J Foot Ankle Surg 2012;51:258-61. [Google Scholar | PubMed]
- 7.Dartnell J, Ramachandran M, Katchburian M. Haematogenous acute and subacute paediatric osteomyelitis: A systematic review of the literature. J Bone Joint Surg Br 2012;94-B:584-95. [Google Scholar | PubMed]
- 8.Shih HN, Shih LY, Wong YC. Diagnosis and treatment of subacute osteomyelitis. J Trauma 2005;58:83-7. [Google Scholar | PubMed]
- 9.Dharmshaktu GS. Brodie’s abscess: Brief review of key updates from the year 2010. J Orthop Dis Traumatol 2020;4:104. [Google Scholar | PubMed]
- 10.Hamdy RC, Lawton L, Carey T, Wiley J, Marton D. Subacute hematogenous osteomyelitis: Are biopsy and surgery always indicated? J Pediatr Orthop 1996;16:220-3. [Google Scholar | PubMed]

Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2026 Case Report: Dupuytren’s Disease in a 12-Year-Old Child; Unusual Clinical Presentation
May 1, 2026 Case Report: Dupuytren’s Disease in a 12-Year-Old Child; Unusual Clinical Presentation July 1, 2026 Extradigital Glomus Tumor of the Knee Mimicking Osteoarthritis: A Case Report
July 1, 2026 Extradigital Glomus Tumor of the Knee Mimicking Osteoarthritis: A Case Report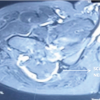 July 1, 2026 Large Posterior Proximal Femur Osteochondroma Presenting in Adulthood – Diagnostic Challenges and Management Strategy: A Case Report
July 1, 2026 Large Posterior Proximal Femur Osteochondroma Presenting in Adulthood – Diagnostic Challenges and Management Strategy: A Case Report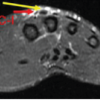 June 1, 2026 Excision without Reconstruction of a Traumatically Ruptured Extensor Indicis Proprius Tendon in a Diabetic Patient: A Case Report
June 1, 2026 Excision without Reconstruction of a Traumatically Ruptured Extensor Indicis Proprius Tendon in a Diabetic Patient: A Case Report