
Median nerve entrapment is a rare complication following a medial epicondyle fracture dislocation of the elbow. Post-reduction pain, dysesthesia or weakness, whether immediate or delayed should be investigated for MN entrapment. If MN entrapment has occurred, this should be treated expeditiously.
Dr. Joseph Boesel, The University of Toledo College of Medicine and Life Sciences, Toledo, OH. E-mail: joseph.boesel@rockets.utoledo.edu
Abstract
Introduction: Medial epicondyle fracture dislocations are common in the pediatric population; however, they often lead to favorable patient outcomes. Rarely, the median nerve (MN) can be trapped within the joint space or fracture upon reduction. If the nerve is trapped within the fracture, the MN slowly gets compressed as the fracture heals, leading to progressive deficits in motor function and sensation. These symptoms present as a mixture of pain, numbness, weakness, and paresthesia in the distribution of the MN. Therefore, careful monitoring of the patient post-reduction is crucial in making an early diagnosis.
Case Report: A 9-year-old girl presented with an incarcerated MN following closed reduction of a left elbow medial epicondyle fracture after multiple reduction attempts. She presented 2 years post-injury with a healed medial epicondyle, median sensory deficits, and anterior interosseous palsy. Nerve studies showed deficits in median-innervated muscles. Operative exploration revealed the MN incarcerated within the healed fracture. Tendon transfer allowed for opposition and flexion of the thumb, index finger flexion, and composite fist formation.
Conclusion: MN entrapment following medial epicondyle reduction may present as ongoing sensory changes and median innervated weakness. Electromyography and advanced imaging should be obtained expeditiously.
Keywords: Median nerve, entrapment, pediatric, medial epicondyle, tendon transfer.
Medial epicondyle fractures account for 11–20% of all pediatric elbow fractures and largely coincide with elbow dislocations [1, 2]. Common complications of nerve entrapment include burning pain, numbness, and paresthesia. If treatment is delayed, weakness, loss of function, and sensory deficits may occur [3]. However, entrapment of the median nerve (MN) is rare following reduction of dislocation [4]. The mechanism of entrapment may be complex. The MN courses medial to the biceps tendon, under the lacertus fibrosus and deep to the pronator teres (PT). Pressure from these more superficial structures may play a role in displacing the MN into a fractured medial epicondyle. Four types of MN entrapment have been described. Type I and II occur when the MN is trapped within the joint space or fracture site, respectively. Type III occurs when the nerve is entrapped in the ulnohumeral joint. Finally, Type IV occurs when the nerve is trapped in the fracture site and joint space [5, 6]. This case highlights the stepwise management of nerve injuries in closed fractures. Prompt sensory and motor testing are crucial to prevent irreversible nerve damage, reducing the need for salvage treatments.
A 9-year-old right-hand dominant female was brought to an outside emergency department (ED) due to a fracture dislocation of the left medial epicondyle after falling from a slide. She presented with severe pain, but no weakness, numbness, or tingling. Radiographs revealed a medial epicondyle fracture with posterolateral dislocation (Fig. 1 and 2). The initial four reduction attempts were unsuccessful, thus she was transferred to another ED where she was still neurovascularly intact, and the subsequent reduction attempt was successful. Following reduction, pulses, sensation to light touch, anterior interosseous nerve, posterior interosseus nerve, and ulnar motor exam were normal. The patient was placed into a univalved cast and discharged with education on compartment syndrome. Twenty-four hours following reduction, the patient experienced painful dysesthesias and digital swelling. Early pain was thought to be normal post-reduction discomfort and compartment syndrome was ruled out and the cast was bivalved. At the 2.5-week follow-up, the patient could “wiggle fingers” but could not flex the distal interphalangeal (DIP) joint of the left index finger or IP joint of the left thumb. The plan was to observe AIN nerve palsy and begin therapy. We cannot assume the reasoning of the outside provider, but the palsy was initially improving according to documentation. At the 60-day follow-up, X-rays showed a healing fracture with evidence of callus and remodeling (Fig. 3 and 4).


Over the next 9 months, the patient’s elbow range of motion improved. Her motor and sensory exam was inconsistently documented, and no demonstrable improvement was noted. At 13 months post-injury, a hand surgeon obtained the first nerve conduction study/electromyography (EMG) which reported moderate to severe left upper extremity (LUE) MN neuropathy localized distal to the innervation of the PT with changes compatible with re-innervation notably in flexor digitorum profundus (FDP) of LUE. It also found superimposed severe AIN injury without voluntary motor units in the flexor pollicis longus (FPL) and pronator quadratus.
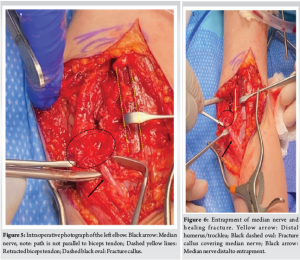
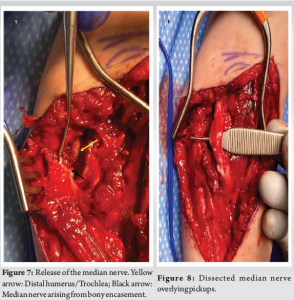
At 24 months post-injury, the patient was referred to our clinic, she had 0/5 FDP index and middle, 0/5 FPL strength, thenar atrophy, but 5/5 function of flexor digitorum superficialis (FDS). Pronation strength was 3/5, and her ulnar and radial innervated muscles demonstrated 5/5 strength. Sensation was diminished in the MN distribution, with Semmes–Weinstein testing between 4.3 and 4.9, Ulnar and radial distributions scored 3.6. Imaging showed a healed medial epicondyle fracture and no entrapped fragments. A follow-up nerve conduction study and EMG showed no sensory response across the left elbow and no motor response of the MN with severe axonometric left MN injury at the elbow above the branch to the PT with evidence of chronic reinnervation. The Abductor Pollicus Brevis, FPL, and PT had abnormal spontaneous activity. Surgical exploration of the fracture union revealed the MN circumferentially encased within the distal medial humerus, entering at the physeal scar of the medial epicondyle and exiting at the anterior medial aspect of the trochlea. We released the MN to maximize sensory recovery. Cortical bone was carefully removed using curettes, micro-osteotomes, a laminar spreader, and a pituitary rongeur, from the anterior portion of the nerve from the distal medial humerus allowing the nerve to be extracted (Fig. 5-8). Gross continuity was preserved, although the nerve was significantly compressed. Nerve stimulation revealed no motor conduction distally as expected due to the chronicity of injury. The decision was made to avoid intercalary grafting and allow sensory recovery to progress now that entrapment was relieved.
Next, because the injury persisted for more than 12 months a tendon transfer was conducted to restore index and thumb function. An extended carpal tunnel incision was made, and the FPL and ring FDS were identified. A chevron incision was made over the ring finger PIP joint and the FDS was released at the middle phalanx. It was reflected proximally and a pulvertaft weave was performed from the FDS to FPL with a neutral wrist and the IP joint of the thumb at 45° of flexion and MP at 30° of flexion.
A 6 cm incision was made at the volar distal third forearm over the flexor carpi radialis tendon. Dissection was carried down to the index FDP. Another incision was made over the dorsal index metacarpal base and the extensor carpi radialis longus (ECRL) was released. The ECRL was tunneled volarly and a pulvertaft weave was performed with the index MP and PIP joints at 45° of flexion and wrist neutral. The tension of both transfers was assessed with passive range of motion. At 6 weeks post-operative, the left elbow range of motion was 120–25° short of full extension. There was ongoing decreased sensation in the MN distribution with a Tinel’s sign at the elbow. The patient could activate the transfers, and motion was improving with therapy. At 1-year post-operative, the patient could form a composite fist, flex the thumb at the IP joint, perform thumb opposition, and flex the DIP joint of the left index finger. Left elbow range of motion along with passive and active wrist flexion and extension are symmetric to the contralateral side. Sensation in the MN distribution was intact with Semmes-Weinstein monofilament testing at 3.61 g. Grip strength is 50% and pinch strength is 66% of the contralateral side.
Attempted reduction of medial epicondyle fracture dislocations can lead to entrapment of the median or ulnar nerves within the healing fracture resulting in impaired upper extremity function. A delayed diagnosis in this patient led to severe deficits within the median-innervated muscles. However, burning dysesthesia and subacute weakness after reduction could have prompted earlier investigation into possible entrapment. EMG studies are recommended for peripheral nerve injury between 2 and 4 weeks following the injury [7] and if completed, would have potentially expedited appropriate care. In a patient with repeated reduction attempts and severe pain within 48 h, a high index of suspicion for MN entrapment should be maintained. Nerve injuries are defined by the Sunderland classification [8]. Neurapraxia presents with sensory abnormalities that often improve after reduction of fracture or relief of compression [9]. Prolonged compression leads to demyelination, and following relief of compression, Schwann cells proliferate to remyelinate the neuron [10]. Depending on the extent of nerve damage, surgeons may wait 6–12 weeks to allow spontaneous recovery [11]. However, early decision-making is crucial for reinnervation of the motor endplate, as irreversible damage to muscle fibers occurs within 12–18 months [12, 13]. As the fracture callus matured and remodeling occurred, the nerve injury likely progressed. Axonotmesis, represented by changes in the number and configuration of motor unit potentials, can be detected diagnostically by EMG [14, 15] and should be completed at 3, 6, and 9 months, if not performed earlier, to provide the clinician with evidence of nerve regeneration or lack thereof [16]. An absence of motor unit potentials at 3–6 months portends a poor prognosis for spontaneous motor recovery and allows the surgeon to decide on exploration [17]. Completing early diagnostic tests is especially important in a pediatric population, where the sensory exam is challenging. Our first visit with the patient was 2 years post-injury, thus motor recovery was not likely. Nerve decompression allowed spontaneous sensory recovery over 12 months. EMG testing was not done following the decompression, as motor recovery is not likely after 1 year. Tendon transfer resulted in functional improvements of grasp and pinch, allowing the patient to return to softball. The importance of a certified hand therapist comfortable with the pediatric population cannot be overstated.
Careful monitoring of sensation and motor function following elbow fracture dislocation is essential for early detection of MN entrapment. Advanced imaging (magnetic resonance imaging/ultrasound) at 3 months may determine if a nerve injury needs further workup via EMG. After an MN entrapment has been diagnosed, early intervention may reduce morbidity and maximize patient function.
MN entrapment is a rare complication following a medial epicondyle fracture dislocation of the elbow. Post-reduction pain, dysesthesia or weakness, whether immediate or delayed should be investigated for MN entrapment. If MN entrapment has occurredthis should be treated expeditiously.
References
- 1.Gottschalk HP, Eisner E, Hosalkar HS. Medial epicondyle fractures in the pediatric population. J Am Acad Orthop Surg 2012;20:223-32. [Google Scholar | PubMed]
- 2.Jeong C, Lee SU, Kim HG, Joo SY. Medial epicondyle fracture in children and its association with increased carrying angle. Int J Clin Pract 2022;2022:6414247. [Google Scholar | PubMed]
- 3.Dydyk AM, Negrete G, Sarwan G, Cascella M. Median nerve injury. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2024. [Google Scholar | PubMed]
- 4.Allen MJ. J. A. Ogden “Skeletal injury in the child”. Br J Sports Med 1983;17:23. [Google Scholar | PubMed]
- 5.O’Brien AC, Teh Z, Rinaldi M, Lee E, Hughes R, Aktselis I, McKean D. Intraosseous type 2 median nerve entrapment after posterior elbow dislocation diagnosed on ultrasound with MRI and surgical correlation. Cureus 2021;13:e18606. [Google Scholar | PubMed]
- 6.Dubey V, Saify A, Samant A, Shahane S. Median nerve entrapment after elbow dislocation and the role of ultrasonography - a case report. J Orthop Case Rep 2017;7:21-4. [Google Scholar | PubMed]
- 7.Sonawane K, Dixit H, Thota N, Jayaraj A, Balavenkatasubramanian J. “Knowing It before blocking it,” the ABCD of the peripheral nerves: Part D (approach to the patient with nerve injuries). Cureus 2023;15:e41782. [Google Scholar | PubMed]
- 8.Sunderland S. A classification of peripheral nerve injuries producing loss of function. Brain 1951;74:491-516. [Google Scholar | PubMed]
- 9.Holbrook HS, Hillesheim RA, Weller WJ. Acute carpal tunnel syndrome and median nerve neurapraxia: A review. Orthop Clin North Am 2022;53:197-203. [Google Scholar | PubMed]
- 10.Menorca RMG, Fussell TS, Elfar JC. Nerve physiology: Mechanisms of injury and recovery. Hand Clin 2013;29:317-30. [Google Scholar | PubMed]
- 11.MacKay BJ, Cox CT, Valerio IL, Greenberg JA, Buncke GM, Evans PJ, et al. Evidence-based approach to timing of nerve surgery: A review. Ann Plast Surg 2021;87:e1-21. [Google Scholar | PubMed]
- 12.Boecker AH, Lukhaup L, Aman M, Bergmeister K, Schwarz D, Bendszus M, et al. Evaluation of MR-neurography in diagnosis and treatment in peripheral nerve surgery of the upper extremity: A matched cohort study. Microsurgery 2022;42:160-9. [Google Scholar | PubMed]
- 13.Tung TH, Mackinnon SE. Nerve transfers: Indications, techniques, and outcomes. J Hand Surg Am 2010;35:332-41. [Google Scholar | PubMed]
- 14.Power HA, Sharma K, El-Haj M, Moore AM, Patterson MM, Mackinnon SE. Compound muscle action potential amplitude predicts the severity of cubital tunnel syndrome. J Bone Joint Surg Am 2019;101:730-8. [Google Scholar | PubMed]
- 15.Chaney B, Nadi M. Axonotmesis. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2024. [Google Scholar | PubMed]
- 16.Abel NA, Januszewski J, Vivas AC, Uribe JS. Femoral nerve and lumbar plexus injury after minimally invasive lateral retroperitoneal transpsoas approach: Electrodiagnostic prognostic indicators and a roadmap to recovery. Neurosurg Rev 2018;41:457-64. [Google Scholar | PubMed]
- 17.Mackinnon SE. Pathophysiology of nerve compression. Hand Clin 2002;18:231-41. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Concurrent Occurrence of Dysplasia Epiphysealis Hemimelica involving Lateral Malleolus and Sinus Tarsi: Rare Case with Review of Literature
July 1, 2026 Concurrent Occurrence of Dysplasia Epiphysealis Hemimelica involving Lateral Malleolus and Sinus Tarsi: Rare Case with Review of Literature July 1, 2026 Posterior Scapular Osteochondroma in a Pediatric Patient: An Uncommon Presentation of a Common Benign Tumor
July 1, 2026 Posterior Scapular Osteochondroma in a Pediatric Patient: An Uncommon Presentation of a Common Benign Tumor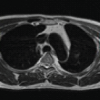 June 1, 2026 Delayed Spontaneous Pectoralis Major Tendon Rupture Following Anterior Latissimus Dorsi Transfer for Irreparable Subscapularis Tear: A Case Report
June 1, 2026 Delayed Spontaneous Pectoralis Major Tendon Rupture Following Anterior Latissimus Dorsi Transfer for Irreparable Subscapularis Tear: A Case Report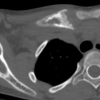 May 1, 2026 A Rare Occurrence of Chronic Recurrent Multifocal Osteomyelitis in Clavicle: Case Report
May 1, 2026 A Rare Occurrence of Chronic Recurrent Multifocal Osteomyelitis in Clavicle: Case Report