
Delayed rupture of the pectoralis major tendon can occur as a rare long-term complication after anterior latissimus dorsi transfer, particularly when partial release of its humeral insertion is performed. Preservation of the pectoralis major insertion during the index procedure is critical to minimize this risk.
Dr. Chang Hee Baek, Department of Orthopaedic Surgery, Yeosu Baek Hospital, Jeollanam-do, Republic of Korea. E-mail: yeosubaek@gmail.com
Abstract
Introduction: Irreparable subscapularis (SSC) tears can lead to significant functional impairment, particularly affecting internal rotation (IR) and anterior shoulder stability. Anterior latissimus dorsi (LD) tendon transfer has gained popularity as a surgical option due to its favourable biomechanical alignment with the SSC. Although partial release of the pectoralis major (PM) tendon is commonly performed during LD harvest and is generally considered safe, its long-term effects on PM integrity remain unclear. This report describes a rare case of delayed spontaneous rupture of the PM humeral insertion following anterior LD transfer.
Case Report: A 57-year-old male presented with progressive IR weakness 5 years after undergoing anterior LD transfer for an irreparable SSC tear. Imaging revealed an intact transferred LD tendon but a complete rupture of the PM humeral insertion with muscle atrophy. The patient underwent PM tendon transfer with acellular dermal matrix augmentation. At 1-year follow-up, significant improvements were observed in pain (Visual Analogue Scale 4–1), Constant score (59–81), and American Shoulder and Elbow Surgeons score (57–82). IR strength improved markedly, and functional tests normalised. Imaging confirmed intact tendon healing, and the patient returned to daily activities without complications.
Conclusion: Delayed rupture of the PM tendon can occur as a long-term complication after anterior LD transfer. PM transfer represents an effective salvage procedure, restoring IR strength and shoulder function. Awareness of this potential complication and preservation of the PM insertion during the index procedure are essential.
Keywords: Pectoralis major, latissimus dorsi transfer, subscapularis tear, shoulder internal rotation, tendon transfer, delayed rupture.
The subscapularis (SSC) muscle serves as the primary internal rotator of the shoulder and is essential for maintaining the anterior force couple and glenohumeral stability. Irreparable tears of the SSC, often accompanied by fatty infiltration, muscle atrophy, and tendon retraction, can result in significant functional impairment and difficulty with daily activities that require internal rotation (IR) of the arm [1,2]. Surgical treatment options for irreparable SSC tears include pectoralis major (PM) transfer; latissimus dorsi (LD) transfer with or without teres major; anterior capsule reconstruction; and reverse shoulder arthroplasty [1,3,4,5]. Among these, LD transfer – particularly anterior LD transfer – has gained attention due to its favourable biomechanical vector alignment with the SSC and its ability to restore the anterior–posterior force couple while preserving active IR [6,7,8,9,10,11,12]. During the traditional anterior LD transfer procedure, partial release of the upper portion of the PM humeral insertion is commonly performed to facilitate exposure and harvesting of the LD tendon [7,9]. This release typically has no immediate clinical consequence, and post-operative PM dysfunction has not been widely reported. However, the long-term effects on PM tendon integrity after such release have not been fully investigated. This report presents a case of delayed, spontaneous rupture of the PM humeral insertion occurring 5 years after anterior LD transfer for an irreparable SSC tear. The patient developed progressive weakness in IR without any traumatic event, ultimately requiring PM transfer to restore shoulder function.
A 57-year-old right-hand-dominant male presented with progressive loss of IR strength and limitation of left shoulder motion, without any history of trauma. The patient had previously undergone anterior LD transfer 5 years earlier for an irreparable SSC tear, with satisfactory initial results. Several months before presentation, he began experiencing weakness during IR, which progressively worsened, causing significant difficulty in performing daily activities. On physical examination, forward elevation (FE) was 160°, abduction (ABD) 150°, external rotation (ER) 40°, and IR reached the buttock level. The SSC-specific physical examination was positive for the Belly Press and Lift-Off tests. Functional assessment scores were suboptimal, with a pain visual analogue scale (VAS) of 4, a Constant score of 59/100, and an American Shoulder and Elbow Surgeons (ASES) score of 57/100. Strength measurements were 29.2 N for forward flexion, 27.1 N for ABD, 26.2 N for ER, and 9.4 N for IR. Radiographs revealed no advanced glenohumeral arthritis. Magnetic resonance imaging showed an irreparable SSC tear extending toward the glenoid surface with poor muscle quality (Goutallier et al. [13] grade III fatty infiltration and atrophy) and an intact previously transferred LD tendon. The humeral insertion of the PM tendon appeared thinned and detached, with distal muscle atrophy (Fig. 1). Based on these findings and the chronic functional deficits, PM transfer was recommended to the patient.
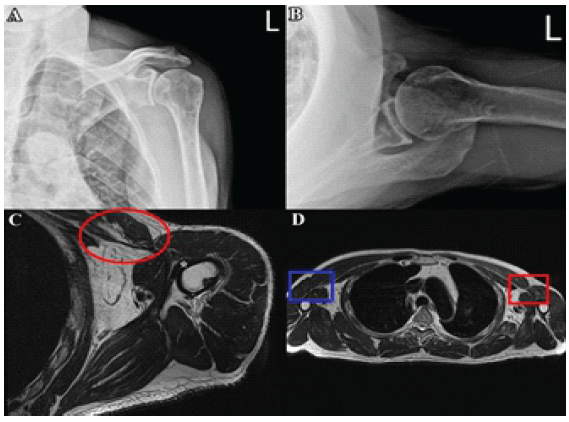
Figure 1: Pre-operative imaging of the left shoulder. Pre-operative radiographs of the left shoulder showing no evidence of advanced glenohumeral arthritis or subluxation in the (a) coronal and (b) axial views. (c) Axial Magnetic resonance imaging (MRI) of the left shoulder demonstrating complete detachment of the pectoralis major (PM) tendon from its humeral insertion, with distal muscle atrophy and tendon thinning (red circle). The previously transferred latissimus dorsi tendon remains intact (white asterisk). (d) Axial MRI of the trunk showing atrophy and complete tear of the distal PM muscle (red rectangle) compared with the intact contralateral side (blue rectangle).
Surgical procedure:
The patient was positioned in the beach-chair position under general anaesthesia. A standard deltopectoral approach was made through the previous incision and extended distally for adequate exposure. Dense adhesions from the prior anterior LD transfer were carefully dissected to identify anatomic landmarks and the transferred LD tendon, which was intact. Intraoperatively, the humeral insertion of the PM tendon was completely detached, with retraction and distal muscle atrophy (Fig. 2).
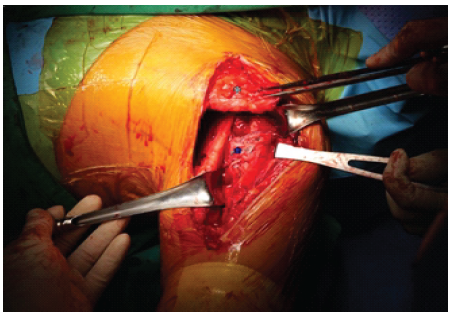
Figure 2: Intraoperative view showing intact previously transferred anterior latissimus dorsi and teres major tendons, with the detached pectoralis major tendon held with two long forceps before harvest.
The tendon stump was frayed and degenerated, precluding primary repair to the humerus. During the previous anterior LD transfer, the upper portion of the PM insertion had been partially released, and a soft-tissue tenodesis of the long head of the biceps (LHB) had been performed on the remnant PM humeral insertion. In the current surgery, dense adhesions were observed between the detached PM tendon and the previous LHB tenodesis, necessitating careful dissection and separation to mobilise the PM tendon for transfer. The PM muscle was meticulously mobilised from surrounding tissues. The tendon end was prepared and augmented with an acellular dermal matrix allograft with three high-strength non-absorbable sutures in a Krackow fashion along both borders (Fig. 3).

Figure 3: Harvested and prepared pectoralis major tendon, augmented with acellular dermal matrix and secured with free sutures, ready for transfer.
Further medial release was performed to achieve tension-free excursion. The prepared PM tendon was rerouted laterally, passing superficial to the conjoined tendon and lateral to the bicipital groove. With the arm in 45° ABD and maximum IR, the intended fixation site was marked approximately 2 cm distal to the greater tuberosity. Three parallel transosseous tunnels were created at the upper, middle, and lower thirds of the marked site using a 1.6-mm Kirschner wire and drill bit. Each suture limb from the PM tendon was passed through the corresponding tunnel and tied over the lateral cortex. Additional looped sutures were shuttled and tied to reinforce fixation and distribute tension evenly (Fig. 4).
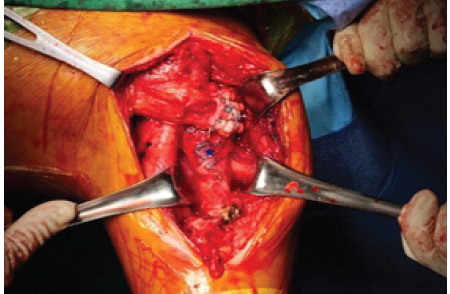
Figure 4: Final appearance after pectoralis major transfer, showing the transferred pectoralis major tendon fixed to the humeral insertion site, with the previously transferred latissimus dorsi tendon remaining intact.
The humerus was taken through full ROM to confirm the absence of impingement or tension overload. Finally, the previously detached LHB was then secured through tenodesis using a suture anchor to the proximal humeral shaft without tension. The surgical site was irrigated, and a layered closure was performed. A soft shoulder brace was applied postoperatively to maintain IR and protect the repair.
Post-operative rehabilitation:
During the first 4 weeks, the patient was immobilised in an IR, with intermittent elbow, wrist, and finger movement permitted to allow light daily activities such as eating and writing. After 4 weeks, the brace was discontinued, and active-assisted ROM exercises were initiated. Strengthening exercises in all directions were introduced at 3 months postoperatively. Heavy labour and sports were recommended to be avoided until 6 months to ensure tendon healing.
Post-operative outcome:
At 1 year postoperatively, the patient reported satisfaction with the outcome. Pain VAS improved from 4 to 1, the constant score increased from 59/100 to 81/100, and the ASES score improved from 57/100 to 82/100. ROM was 160° for FE, 160° for ABD, 40° for ER, and IR improved to the L1 level. IR strength increased from 9.4 N to 26.2 N. Postoperatively, an SSC-specific physical examination, including the Belly Press and Lift-Off tests, was negative, indicating reversal of pre-operative deficits. Radiographs showed no progression of glenohumeral arthritis or subluxation. Ultrasonography confirmed an intact transferred PM tendon with secure tendon-to-bone healing. The patient returned to work and daily activities by 6 months postoperatively and remained symptom-free without complications at the latest follow-up.
This case highlights a rare delayed complication following anterior LD transfer for an irreparable SSC tear – spontaneous rupture of the PM humeral insertion. Partial release of the superior PM tendon is commonly performed during LD tendon harvest and is generally considered benign [7,9]. However, this case suggests that even minor alterations of the PM insertion, combined with long-term altered shoulder mechanics, may predispose the tendon to progressive degeneration and rupture. Anterior LD transfer carries potential complications, including tendon retear, progression of glenohumeral arthritis, infection, and axillary nerve injury [7,10,14]. Retears are uncommon but may occur early postoperatively [15,16]. Arthritis progression can develop over long-term follow-up, particularly in patients with pre-existing degenerative changes [10]. Infection is rare but possible, and axillary nerve injury, though uncommon, may result from dissection during tendon harvest or impingement after the transfer [11,14]. Awareness of these risks is important for surgical planning and patient counselling. Theoretically, PM rupture may also occur, especially in patients who previously underwent LD transfer with partial detachment of the PM humeral insertion. Although typically unreported, if PM rupture occurs, it can lead to significant functional deficits, including loss of IR strength and impairment in performing essential daily activities. The mechanism of delayed PM rupture is likely multifactorial, including subclinical weakening of the humeral insertion during the prior LD harvest, chronic overuse of the residual PM fibres, and age-related degenerative changes. Altered IR biomechanics following anterior LD transfer may have further contributed to abnormal stress on the PM insertion. In addition, the previous soft-tissue tenodesis of the LHB during the LD transfer may have increased local tension and contributed to the rupture. The tendon rupture occurred 5 years postoperatively without trauma, suggesting a chronic degenerative process rather than an acute failure. At present, preservation of the PM insertion during anterior LD (with or without teres major transfer) is emphasised to prevent damage, often facilitated using arthroscopic techniques or instruments such as the Kobel retractor during open technique, as previously described in the literature [17,18]. In this case, primary repair of the PM tendon was not feasible due to atrophy and poor tissue quality. The PM transfer was performed as a salvage procedure, resulting in substantial improvement in pain, ROM, IR strength, and functional outcomes, without evidence of retear, progression of arthritis, or other complications. Surgeons should preserve as much of the PM humeral insertion as possible during anterior LD transfer and consider spontaneous PM rupture in patients presenting with delayed IR weakness.
Delayed rupture of the PM humeral insertion can occur several years after anterior LD transfer for an irreparable SSC tear, likely due to prior partial release and chronic degenerative changes. PM transfer is an effective salvage procedure, restoring IR strength and improving shoulder function. Careful preservation of the PM insertion during anterior LD transfer and awareness of potential long-term complications are essential for optimising outcomes.
Delayed pectoralis major rupture may occur years after anterior latissimus dorsi transfer, particularly when partial tendon release is performed. Surgeons should preserve the pectoralis major insertion whenever possible and maintain long-term vigilance in patients presenting with new internal rotation weakness. Pectoralis major transfer can serve as an effective salvage procedure to restore function and strength.
References
- 1. Oh JH, Park MS, Rhee SM. Treatment strategy for irreparable rotator cuff tears. Clin Orthop Surg 2018;10:119-34. [Google Scholar] [PubMed]
- 2. Collin P, Matsumura N, Lädermann A, Denard PJ, Walch G. Relationship between massive chronic rotator cuff tear pattern and loss of active shoulder range of motion. J Shoulder Elbow Surg 2014;23:1195-202. [Google Scholar] [PubMed]
- 3. Rho JY, Kwon YS, Choi S. Current concepts and recent trends in arthroscopic treatment of large to massive rotator cuff tears: A review. Clin Shoulder Elb 2019;22:50-7. [Google Scholar] [PubMed]
- 4. Mirzayan R, Korber S. Anterior capsular reconstruction with acellular dermal allograft for subscapularis deficiency: A report of two cases. Clin Shoulder Elb 2024;27:126-30. [Google Scholar] [PubMed]
- 5. Cunningham JG, Ebert JR, Campbell P, Falconer T. Does subscapularis integrity influence outcome following Latissimus dorsi tendon transfer for irreparable cuff tears? A comparative series of 48 patients. J Orthop 2022;31:129-33. [Google Scholar] [PubMed]
- 6. Lim TK, Bae KH. Arthroscopic-assisted Latissimus dorsi tendon transfer for the management of irreparable rotator cuff tears in middle-aged physically active patients. Clin Shoulder Elb 2019;22:9-15. [Google Scholar] [PubMed]
- 7. Elhassan BT, Wagner ER, Kany J. Latissimus dorsi transfer for irreparable subscapularis tear. J Shoulder Elbow Surg 2020;29:2128-34. [Google Scholar] [PubMed]
- 8. Luo Z, Lin J, Sun Y, Zhu K, Wang C, Chen J. Outcome comparison of Latissimus dorsi transfer and pectoralis major transfer for irreparable subscapularis tendon tear: A systematic review. Am J Sports Med 2022;50:2032-41. [Google Scholar] [PubMed]
- 9. Mun SW, Kim JY, Yi SH, Baek CH. Latissimus dorsi transfer for irreparable subscapularis tendon tears. J Shoulder Elbow Surg 2018;27:1057-64. [Google Scholar] [PubMed]
- 10. Baek CH, Kim JG, Kim BT. Long-term outcomes of anterior Latissimus dorsi tendon transfer for irreparable subscapularis tears. Bone Joint J. 2024;106-B:957-63. [Google Scholar] [PubMed]
- 11. Kany J, Guinand R, Croutzet P, Valenti P, Werthel JD, Grimberg J. Arthroscopic-assisted Latissimus dorsi transfer for subscapularis deficiency. Eur J Orthop Surg Traumatol 2016;26:329-34. [Google Scholar] [PubMed]
- 12. Baek CH, Kim JG, Baek GR. Outcomes of combined anterior Latissimus dorsi and teres major tendon transfer for irreparable anterosuperior rotator cuff tears. J Shoulder Elbow Surg 2022;31:2298-307. [Google Scholar] [PubMed]
- 13. Goutallier D, Postel JM, Bernageau J, Lavau L, Voisin MC. Fatty muscle degeneration in cuff ruptures. Pre- and postoperative evaluation by CT scan. Clin Orthop Relat Res 1994;304:78-83. [Google Scholar] [PubMed]
- 14. Elhassan B, Christensen TJ, Wagner ER. Feasibility of latissimus and teres major transfer to reconstruct irreparable subscapularis tendon tear: An anatomic study. J Shoulder Elbow Surg 2014;23:492-9. [Google Scholar] [PubMed]
- 15. Kany J, Sekaran P, Grimberg J, Amavarathi RS, Valenti P, Elhassan B, et al. Risk of Latissimus dorsi tendon rupture after arthroscopic transfer for posterior superior rotator cuff tear: A comparative analysis of 3 humeral head fixation techniques. J Shoulder Elbow Surg 2020;29:282-90. [Google Scholar] [PubMed]
- 16. Kany J, Grimberg J, Amaravathi RS, Sekaran P, Scorpie D, Werthel JD. Arthroscopically-assisted Latissimus dorsi transfer for irreparable rotator cuff insufficiency: Modes of failure and clinical correlation. Arthroscopy 2018;34:1139-50. [Google Scholar] [PubMed]
- 17. Kim BT, Miranda LA, Baek CH, Kany J. Fully arthroscopic anterior Latissimus dorsi and teres major transfer for anterosuperior irreparable rotator cuff tears. Arthrosc Tech 2025;14:103665. [Google Scholar] [PubMed]
- 18. Baek CH, Kim BT, Kim JG. Combined anterior Latissimus dorsi and teres major tendon transfer (aLDTM) for irreparable anterosuperior rotator cuff tears. JBJS Essent Surg Tech 2024;14:e23.00060. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Anterior Latissimus Dorsi and Teres Major Tendon Transfer with Total Shoulder Arthroplasty in the Setting of Subscapularis Insufficiency: A Case Report
June 1, 2026 Anterior Latissimus Dorsi and Teres Major Tendon Transfer with Total Shoulder Arthroplasty in the Setting of Subscapularis Insufficiency: A Case Report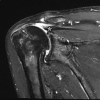 January 1, 2026 Dual Reconstruction, Combined Anterior Latissimus Dorsi with Teres Major and Middle Trapezius Tendon Transfer, Reduces Anterior Superior Humeral Subluxation: Case Report
January 1, 2026 Dual Reconstruction, Combined Anterior Latissimus Dorsi with Teres Major and Middle Trapezius Tendon Transfer, Reduces Anterior Superior Humeral Subluxation: Case Report December 1, 2025 Flexor Tendon Injuries in Zone 3: A Comprehensive Review and Case Report on Flexor Digitorum Profundus Rupture of the Middle Finger
December 1, 2025 Flexor Tendon Injuries in Zone 3: A Comprehensive Review and Case Report on Flexor Digitorum Profundus Rupture of the Middle Finger February 1, 2025 Medial Epicondyle Fracture Dislocation, Multiple Failed Reductions, and a Median Nerve Entrapment: A Case Report
February 1, 2025 Medial Epicondyle Fracture Dislocation, Multiple Failed Reductions, and a Median Nerve Entrapment: A Case Report