
The case highlights that shoulder tuberculosis, though rare and challenging to diagnose, can be effectively managed using Anti-Tuberculosis Treatment (ATT) and an antibiotic-coated cement spacer, emphasizing the importance of early diagnosis and a multidisciplinary approach to restore joint function and minimize complications
Dr. Kishankumar Mahida, Department of Orthopaedics, Dr. D.Y. Patil Medical College and Hospital, Pimpri, Pune, Maharashtra, India. E-mail: mahidakishan2198@gmail.com
Abstract
Introduction: Tuberculosis (TB) remains a significant health issue in India, with approximately 30–40% incidence. While only 18% of TB cases are extrapulmonary, shoulder TB, particularly Caries sicca, is extremely rare. Caries sicca is characterized by severe pain, restricted shoulder movements, and significant muscle wasting, often resulting in avascular necrosis (AVN) of the humeral head.
Case Report: This case report describes the management and rehabilitation of a 38-year-old woman with shoulder TB and AVN. The patient presented with a 5-year history of persistent shoulder pain and restricted motion. Radiological and histopathological examinations confirmed osteonecrosis and TB. The treatment involved arthroscopic debridement, antitubercular therapy, and staged surgical intervention including the placement of an iliac crest bone graft and antibiotic cement spacer, followed by reverse shoulder replacement.
Conclusion: Tubercular shoulder is challenging to diagnose and manage. Anti-tuberculosis treatment (ATT) combined with the use of an antibiotic-coated cement spacer provides an effective strategy to eradicate infection and prepare the joint for future replacement. Early diagnosis and a staged approach are essential to address joint destruction and restore functionality, ensuring better outcomes for patients.
Keywords: Avascular necrosis, tuberculosis, caries sicca, upper limb
Tuberculosis (TB) remains a significant cause of illness and death in India, with an incidence rate of approximately 30–40% [1]. Among TB cases, only about 18% are extrapulmonary, with shoulder TB accounting for a small proportion of 0.9–1.7% [2]. Extrapulmonary TB typically spreads hematogenously from pulmonary foci, such as lymph nodes and skeletal TB [3]. One manifestation of shoulder TB is Caries sicca, also known as the dry or atrophic form, characterized by severe pain, restricted shoulder movements, and significant muscle wasting [4]. Imaging studies often reveal regional osteopenia and/or lytic bony lesions [5]. Avascular necrosis (AVN) of the humeral head is a debilitating condition that causes severe pain, limited range of motion, and loss of shoulder function. AVN commonly affects the femoral head, with the humeral head being the next most frequently involved site [6]. Approximately 5% of shoulder arthroplasties are performed due to primary AVN of the humeral head. Treatment options for humeral head AVN include non-surgical therapies, arthroscopic debridement, core decompression, humeral head resurfacing, vascularized bone grafting, and shoulder arthroplasty [7]. This case report focuses on osteonecrosis of the humeral head and its treatment strategies.
A 38-year-old woman visited the Outpatient Department complaining of persistent right shoulder pain for the past 5 years, without any history of trauma or falls. She appeared moderately built and well-nourished, and her systemic examination was unremarkable. The patient exhibited significantly reduced range of motion in her right shoulder in all directions. Examination revealed marked tenderness in the affected area, with no signs of discharging sinus or compromise to the neurovascular structures distally.
Investigations
Radiological assessment by a normal radiograph revealed extensive destruction of the right humeral head and glenoid (Fig. 1).

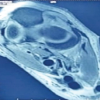
On 3D-CT scan, which correlated with the radiographs, findings indicated significant erosion and destruction affecting the medial and posterior aspects of the right humeral head as well as the glenoid (Fig. 2).

Sputum studies and CBNAAT studies were done which confirmed the diagnosis of pulmonary TB
Treatment
Subsequently, the patient underwent arthroscopic debridement followed by a biopsy. The histopathology report confirmed osteonecrosis of the humeral head, and samples sent for CBNAAT analysis tested positive for TB.
As a result, the patient was initiated on a Category 1 Antitubercular Regimen, that is, isoniazid, Rifampicin, Pyrazinamide, Ethambutol, and was registered in the Directly Observed Treatment, Short-course (DOTS) scheme. The Category 1 regimen is used for newly diagnosed TB cases (pulmonary and extrapulmonary) in drug-sensitive TB. The treatment was started for 6 months (2 months intensive phase + 4 months continuation phase). At 8 weeks from the initial procedure, the patient underwent a second stage in the operating theatre. The procedure involved complete removal of the necrotic bone followed by the placement of an iliac crest bone graft to restore the bone structure of the glenoid defect. In addition, a stemmed antibiotic-coated cement spacer was applied to address the defect in the humeral head (Fig. 3). A unilateral platform reverse shoulder replacement procedure for the right shoulder was scheduled. Histopathological examination revealed the presence of Langerhans giant cells and epithelioid granulomas. As a result, the patient was started on anti-tubercular treatment (ATT) under Category 1 of the Revised National TB Control Program (RNTCP) for a duration of 12–18 months and was started on following drugs, that is, Isoniazid, Rifampicin, Pyrazinamide, EThambutol.

Outcome and follow-up
Following the procedure, the shoulder was immobilized for 8 weeks (Fig. 4). The patient received appropriate antibiotics and underwent post-operative rehabilitation, including assisted elbow range of motion exercises. At the 6-month follow-up, the patient had achieved range of motion of 0–90 of abduction and forward flexion, 0–20 external rotation, and internal rotation till L4–L5. At 9–12 months following spacer surgery and provided all the infective markers and MRI scan became negative further management was planned. As the patient had pain VAS score of 1 and she resumed all activities of daily living patient obtained to delay the further procedure, that is, reverse shoulder replacement for the future. Long-term risk of the spacer was explained to the patient which is recurrence of infection, spacer dislocation, breakage or loosening, Bone resorption, and Antibiotic resistance.
Shoulder TB is a rare form of skeletal TB, often leading to misdiagnosis or delayed diagnosis [4]. Approximately 50% of cases are initially mistaken for conditions such as frozen shoulder, rotator cuff injury, tumors, infections, or arthritis of the shoulder joint [8]. The average delay between symptom onset and TB shoulder diagnosis is around 15 months. In some cases, diagnosis occurs only after complications like pathological fractures, subluxation, or severe arthritis develop [5]. Shoulder TB, known as caries sicca, manifests as a dry, insidious, and slow-forming lesion primarily affecting adults [6]. It commonly involves the synovium and subchondral bone, leading to osteoporosis, reduced joint space, subchondral erosions, progressive joint destruction, and reactive sclerosis on radiographs [9]. Early-stage treatment options include arthroscopic debridement and core decompression of the humeral head [10]. In advanced stages, interventions such as humeral head resurfacing, hemiarthroplasty, or reverse shoulder replacement may be necessary [11]. Several case reports underscore the efficacy of surgical debridement, drainage, and ATT in managing delayed presentations of shoulder TB. For instance, successful outcomes have been achieved with open debridement and internal fixation using a rush nail alongside anti-tubercular therapy [12]. Radiographic signs of healing include restoration of trabeculae, reduction in osteoporosis, and remineralization. Despite joint degeneration, conservative therapy and rehabilitation have shown promising functional outcomes in managing shoulder TB [8]. This case highlights the unusual presentation of shoulder TB and underscores the importance of modern imaging modalities in facilitating accurate diagnosis and treatment planning for such complex cases.
Shoulder TB remains a rare yet challenging condition to diagnose and manage, particularly in regions where TB is endemic. Its non-specific clinical presentation, often mimicking other conditions like frozen shoulder or arthritis, contributes to delayed diagnosis and advanced disease at the time of treatment. This case highlights the importance of considering TB in the differential diagnosis of persistent, treatment-resistant shoulder pain. The combination of ATT and an antibiotic-coated cement spacer represents an effective and innovative strategy for managing complex cases of shoulder TB with significant joint destruction. The cement spacer not only provides local antibiotic delivery to eradicate infection but also maintains joint stability, allowing for future definitive procedures, such as joint replacement, if necessary. A staged treatment approach, including initial infection control through debridement and spacer placement, followed by long-term ATT, ensures the eradication of infection while preparing the joint for potential reconstruction. Furthermore, active post-operative rehabilitation is critical in restoring joint mobility, improving functional outcomes, and enhancing the patient’s quality of life. This case underscores the need for early diagnosis, multidisciplinary care, and advanced surgical interventions in managing shoulder TB. Comprehensive strategies combining medical therapy, surgical precision, and physiotherapy are essential to achieve successful outcomes and minimize the long-term complications associated with this condition.
The clinical message of the article is that early diagnosis and innovative treatment strategies, such as the use of ATT combined with biopsy, debridement, and with antibiotic-coated cement spacers we can effectively manage such cases of shoulder TB.
References
- 1.Chadha VK. Tuberculosis epidemiology in India: A review. Int J Tuberc Lung Dis 2005;9:1072-82. [Google Scholar | PubMed]
- 2.Tuli SM. Tuberculosis of the shoulder. In: Tuberculosis of the Skeletal System. 1st ed. New Delhi: Jaypee Brothers Medical Publisher P Ltd.; 1993. [Google Scholar | PubMed]
- 3.Denard PJ, Wirth MA, Orfaly RM. Management of glenohumeral arthritis in the young adult. J Bone Joint Surg Am 2011;93:885-92. [Google Scholar | PubMed]
- 4.Patel PR, Patel DA, Thakker T, Shah K, Shah VB. Tuberculosis of shoulder joint. Indian J Orthop 2003;37:7. [Google Scholar | PubMed]
- 5.Darraj M. Delayed presentation of shoulder tuberculosis: A case report. Case Rep Infect Dis 2018;2018:8591075. [Google Scholar | PubMed]
- 6.Richter R, Hahn H, Nubling W, Kohler G. Shoulder girdle and shoulder joint tuberculosis. Z Rhematol 1985;44:87-92. [Google Scholar | PubMed]
- 7.Kelly PJ, Kalson AG. Musculoskeletal tuberculosis. Mayo Clin Proc 1969;44:73-80. [Google Scholar | PubMed]
- 8.Cruess RL. Osteonecrosis of bone. Current concepts as to etiology and pathogenesis. Clin Orthop Relat Res 1986;208:30-9. [Google Scholar | PubMed]
- 9.Birole U, Ranade A, Mone M. A case report of an unusual case of tuberculous osteomyelitis causing spontaneous pathological fracture of humerus in a middle aged female. J Orthop Case Rep 2017;7:41-5. [Google Scholar | PubMed]
- 10.Martini M, Benkeddache Y, Medjani Y, Gottesman H. Tuberculosis of the upper limb joints. Int Orthop 1986;10:17-23. [Google Scholar | PubMed]
- 11.Sharma PK, Madegowda A, Mittal R. Tuberculosis of patella: Non-specific presentation, treated conservatively. Int J Health Allied Sci 2017;6:194-6. [Google Scholar | PubMed]
- 12.Subasi M, Necmioglu S, Tuzuner T. The Evaluation of our Patients with Bone and Soft Tissue Tuberculosis. National Turkish Orthopaedic and Trauma Congress Book. XVI. Ankara: Sargin offset; 1999. p. 1043-5. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Tuberculosis of the Elbow in a Chronic Kidney Disease Patient with Arteriovenous Fistula: A Case Report
July 1, 2026 Tuberculosis of the Elbow in a Chronic Kidney Disease Patient with Arteriovenous Fistula: A Case Report July 1, 2026 A Comparative Study of Functional Outcome Following Total Hip Replacement by Posterolateral and Anterolateral Approach
July 1, 2026 A Comparative Study of Functional Outcome Following Total Hip Replacement by Posterolateral and Anterolateral Approach July 1, 2026 Managing Complications of Total Hip Arthroplasty for Avascular Necrosis Hip Performed Via Anterior Approach
July 1, 2026 Managing Complications of Total Hip Arthroplasty for Avascular Necrosis Hip Performed Via Anterior Approach June 1, 2026 Functional Outcomes of Total Hip Arthroplasty using Modified Harris Hip Score and Oxford Hip Score: A Prospective Study
June 1, 2026 Functional Outcomes of Total Hip Arthroplasty using Modified Harris Hip Score and Oxford Hip Score: A Prospective Study