
The anterolateral approach in total hip arthroplasty provides better early functional recovery and pain relief than the posterolateral approach while maintaining comparable complication rates in patients with avascular necrosis of the femoral head.
Dr. Sunil Parmar, Department of Orthopaedics, Gandhi Medical College, Bhopal, Madhya Pradesh, India. E-mail: drsunilparmar8965@gmail.com
Abstract
Introduction: Total hip arthroplasty (THA) is a conclusive intervention for advanced avascular necrosis (AVN) of the femoral head. The anterolateral and posterolateral surgical methods are the most frequently employed; yet the ideal approach remains debated. The present study compared functional outcomes, pain relief, and post-operative complications between the anterolateral and posterolateral approaches in patients undergoing THA.
Materials and Methods: This prospective-retrospective observational study was conducted on 60 patients diagnosed with stage III and IV AVN of the femoral head who underwent THA. Patients were divided into the anterolateral (n = 29) and posterolateral (n = 31) groups. Functional results were evaluated using the Harris Hip Score (HHS), and pain was measured using the Visual Analogue Scale (VAS). Follow-up was performed at 1 and 6 months post-operatively.
Results: Both techniques showed statistically significant improvements in HHS and reductions in VAS scores over time (P < 0.001). Pre-operative functional and pain scores were similar between the two groups. The anterolateral approach resulted in significantly higher HHS and lower VAS scores than the posterolateral approach at 1 and 6 months post-operatively (P < 0.05). Post-operative complications were infrequent and did not differ between the two groups.
Conclusion: Both anterolateral and posterolateral approaches are safe and effective for the treatment of AVN of the femoral head by THA. The anterolateral approach allows for better early functional recovery and pain relief, but the overall complication rates are similar. The surgeon’s experience and the patient’s individual characteristics should determine the surgical approach.
Keywords: Total hip arthroplasty, avascular necrosis, anterolateral approach, posterolateral approach, Harris Hip Score
Total hip arthroplasty (THA) is one of the most common orthopaedic procedures globally, with consistently excellent functional outcomes and pain relief in patients with end-stage hip joint diseases, such as osteoarthritis and avascular necrosis (AVN) of the femoral head [1]. AVN is an important indication for THA in low- and middle-income countries. AVN is often related to steroid abuse, chronic alcohol consumption, trauma, and haemoglobinopathies, such as sickle cell disease. About 9–10% of primary total hip arthroplasties are performed for paediatric and adolescent hip problems, including Perthes disease, juvenile rheumatoid arthritis, slipped capital femoral epiphysis, and developmental abnormalities of the hip [2,3]. Since its introduction in the 1960s, THA has been associated with remarkable breakthroughs and remains one of the most successful surgical procedures in orthopaedics. THA is associated with post-operative complications despite positive results, and its incidence depends on the surgical technique used [4,5]. The selection of surgical technique depends on many factors, including surgeon preference, underlying pathology, patient age, bone quality, and surgical proficiency [6]. Commonly used techniques include the anterolateral, direct lateral, direct anterior, and posterior approaches. Each method varies in incision, surgical planes, and soft-tissue management, thus affecting post-operative recovery, stability, and complication rates [7,8]. The posterolateral approach is the most common and provides better exposure. Still, it requires detachment of the short external rotators and has been associated with increased dislocation rates in some studies [7]. Anterior-based techniques, such as direct anterior and anterolateral approaches, utilise intermuscular planes and are associated with lower dislocation rates and faster recovery [9]. The direct anterior approach has benefits, including decreased post-operative pain and reduced length of hospital stay, but it carries a risk of lateral femoral cutaneous nerve injury [10].
The anterolateral technique infrequently causes injury to the lateral femoral cutaneous nerve. It facilitates preservation of the anterior capsule and the iliofemoral ligament, thereby enhancing hip stability and minimising the risk of limb-length discrepancy. Nonetheless, it may be linked to temporary abductor weakness resulting from possible damage to the superior gluteal nerve [11].
Study design and setting:
This observational study, both prospective and retrospective, was conducted in the Department of Orthopaedics at Gandhi Medical College and Hamidia Hospital, Bhopal, a tertiary care referral facility, from May 2023 to October 2024. The study included both retrospectively assessed cases from hospital records and prospectively enrolled individuals throughout the study duration. Approval for the study was secured from the Institutional Ethics Committee (Approval number 18867/MC/IEC/2023 dated May 09, 2023) of Gandhi Medical College, Bhopal. Informed written consent was acquired from all patients participating in the prospective arm of the trial.
Study population:
Patients aged more than 20 years diagnosed with AVN of the femoral head, classified as Stage III or Stage IV according to the Ficat and Arlet classification, and planned for primary THA were included in the study. Patients younger than 20 years, those unwilling to provide informed consent, patients medically unfit for surgery, patients with an active focus of infection, and those undergoing revision THA were excluded. Sixty patients meeting the inclusion criteria were enrolled. Retrospective data were obtained from existing hospital clinical records, whereas prospective patients were enrolled consecutively throughout the study.
Data collection:
Data were gathered using a standardised pro forma that encompassed demographic information, clinical history, symptom duration, and the laterality of hip involvement. All patients had a comprehensive general and localised clinical assessment. The pre-operative evaluation included assessment of the Harris Hip Score (HHS). Baseline investigations included a complete blood count, renal and liver function assessments, blood glucose measurements, routine urine examination with microscopy and culture sensitivity, electrocardiography, chest radiography, pelvic X-ray with bilateral hip imaging, and magnetic resonance imaging of both hips as necessary. Perioperative and post-operative information was documented from surgical notes and patient records.
Assessment of functional outcome:
The functional result was evaluated using the HHS system, a validated and well-recognised instrument for assessing pain, function, deformity, and range of motion in patients after hip surgery. The level of pain was evaluated with the Visual Analogue Scale (VAS). Evaluations were conducted pre-operatively and at 1-month and 6-month follow-up appointments to assess improvements in functional status and relief of discomfort.
Assessment of post-operative recovery and complications:
Post-operative recovery was evaluated by documenting the time to ambulation with support and the time required to ambulate without support. Limb length discrepancy was assessed clinically during follow-up visits. Radiological evaluation included anteroposterior pelvis radiographs with both hips obtained during follow-up visits. All post-operative complications that occurred during the follow-up period were documented.
Statistical analysis:
Data were entered into Microsoft Excel 2010 and analysed using the Statistical Package for the Social Sciences version 19. Continuous variables were represented as mean ± standard deviation, whereas categorical variables were represented as frequencies and percentages. Comparisons across groups were conducted utilising the unpaired t-test for continuous variables and Fisher’s exact test for categorical data. Intra-group comparisons over time intervals were assessed utilising repeated-measures analysis of variance. A P-value below 0.05 was deemed statistically significant.
The final analysis included 60 patients with Stage III and IV AVN of the femoral head who received THA. Among these, 29 patients underwent surgery through the anterolateral approach, whereas 31 patients were operated on utilising the posterolateral method. The baseline demographic and clinical features were analogous between the two groups.
Demographic and baseline characteristics:
The demographic characteristics of the study population are encapsulated in Table 1.
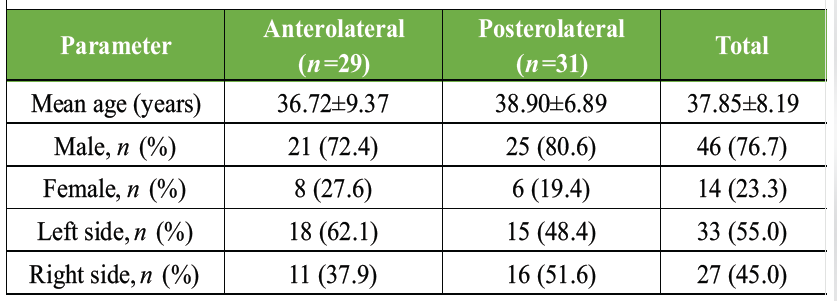
Table 1: Demographic and baseline characteristics of study groups (n=60)
The average age of patients in the anterolateral group was 36.72 ± 9.37 years, whereas in the posterolateral group it was 38.90 ± 6.89 years. A male predominance was noted in both groups. Left-sided hip involvement occurred significantly more frequently overall. No statistically significant variations were noted between the two groups concerning age, gender distribution, or laterality of hip involvement.
Functional outcome – HHS:
Both surgical methods showed statistically significant enhancements in the HHS over time (P < 0.001). Pre-operative HHS values were analogous between the two groups, signifying equivalent baseline functional status. At both the 1-month and 6-month follow-up periods, patients in the anterolateral group had higher mean HHS values than those in the posterolateral group, indicating improved early- and mid-term functional recovery. Fig. 1 depicts the progression of functional outcome improvement over time for both groups.
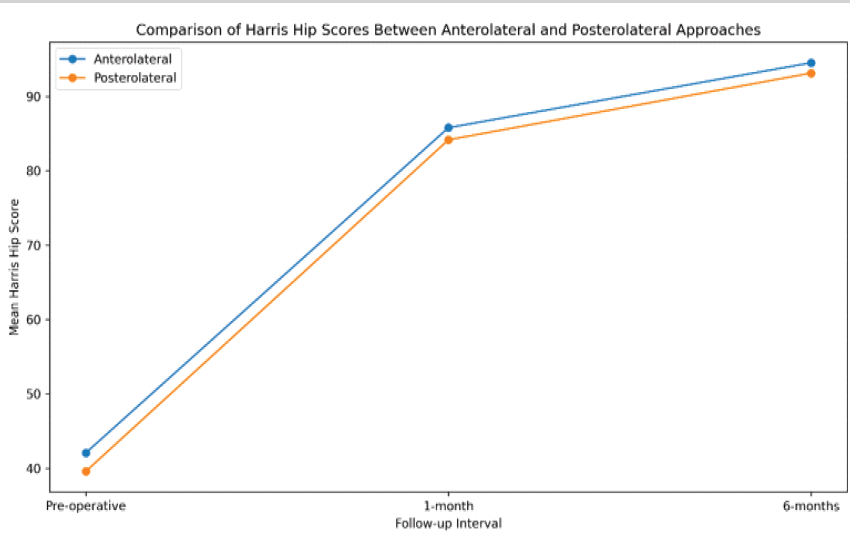
Figure 1: Comparison of mean Harris Hip Scores between anterolateral and posterolateral approaches at different follow-up intervals.
Pain assessment – VAS:
Pain scores, assessed using the VAS, showed a statistically significant reduction in both groups during follow-up (P < 0.001). Pre-operative VAS scores were comparable between the two groups.
At both 1-month and 6-month follow-ups, patients who underwent anterolateral surgery reported lower mean VAS scores than those in the posterolateral group, indicating superior post-operative pain relief. The progressive reduction in pain scores and inter-group differences over time is depicted in Fig. 2.
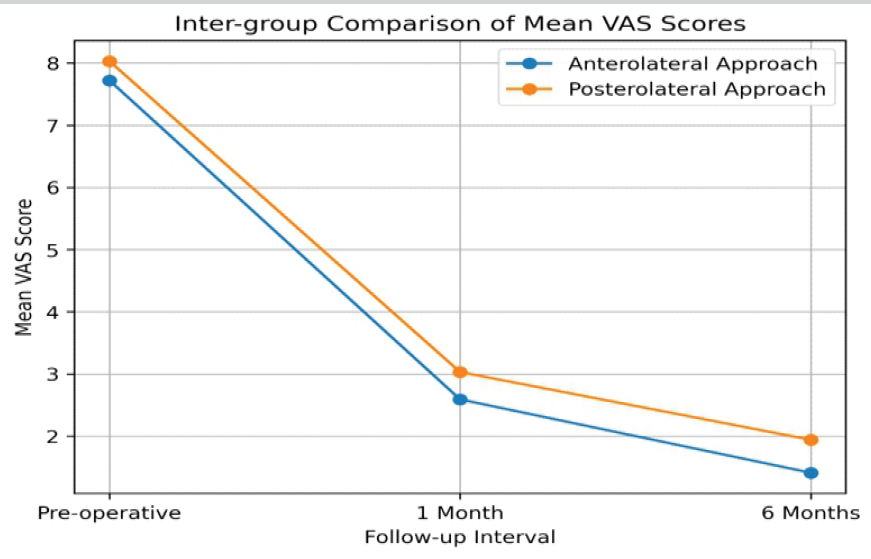
Figure 2: Trend of mean Visual Analog Scale scores following total hip arthroplasty in anterolateral and posterolateral approach groups.
Post-operative outcomes and surgical parameters:
Table 2 presents post-operative results and surgical parameters.
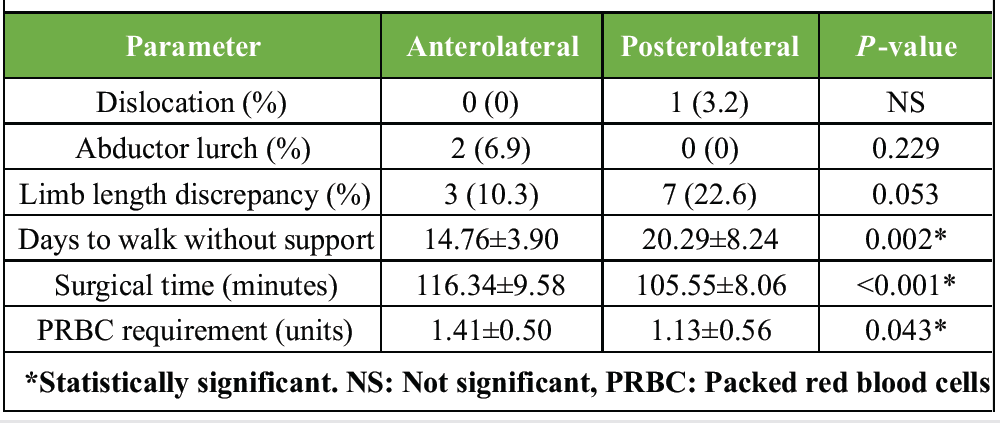
Table 2: Post-operative outcomes and surgical parameters
No post-operative infections were observed in either cohort. Post-operative dislocation was observed in one patient (3.2%) in the posterolateral cohort and in no patients in the anterolateral cohort.
Abductor lurch was present in 2 individuals (6.9%) of the anterolateral group but in none of the posterolateral group. Limb length discrepancy was more frequent in the posterolateral group, but the difference was not statistically significant. Patients in the anterolateral cohort achieved independent ambulation significantly earlier than patients in the posterolateral cohort (P = 0.002). However, the duration of surgery and the need for packed red blood cells were significantly higher in the anterolateral group.
THA is a proven and successful surgical management of advanced AVN of the femoral head, resulting in reproducible pain relief and functional recovery. The choice of surgical strategy is controversial, as each method has its own benefits and specific complications. Both anterolateral and posterolateral approaches significantly improved functional outcomes and pain relief, but the anterolateral approach was associated with better early functional recovery and post-operative pain. The study population was predominantly male in the younger age group, which is in accordance with the epidemiological pattern of AVN in developing countries, where the use of steroids and continued alcohol consumption are common etiological factors. The mean age of patients who underwent THA for AVN was 34.7 years, as reported by Teimouri et al. [12]. Goncharov et al. [13], in a comprehensive review, confirmed male predominance in THA for AVN, aligning with the demographic profile identified in the present study. In our cohort, baseline demographic data, including age, gender, and laterality, were similar between the two groups, thus eliminating confounding factors and allowing a valid comparison of post-operative outcomes. Functional outcomes assessed by the HHS showed significant improvement in both groups after surgery, which supports the effectiveness of THA in improving hip function. Pre-operative HHS was comparable between groups, enabling a meaningful comparison of post-operative results. The HHS values at the 1- and 6-month follow-ups were significantly higher in the anterolateral group, indicating better early functional recovery. Similar findings were reported by Ramadanov et al. [14], who showed better early functional outcomes with an anterior-based approach. In contrast, Amouzadeh Omrani et al. [15] reported better post-operative function with the anterolateral approach than the posterior approaches. The management of post-operative pain following THA is an important determinant of patient satisfaction and early mobilisation. In the present study, both groups showed significant reductions in VAS scores over time. Still, patients who underwent the anterolateral approach had significantly lower pain scores at both follow-up intervals. Reduced muscle trauma allows for better post-operative pain control, and Bulzan et al. [16] reported faster pain resolution and improved early rehabilitation after THA. The data support the concept that preservation of periarticular muscle is important in post-operative pain relief and rapid recovery. Post-operative complications were few and similar in the two groups. No cases of post-operative infection were reported. One dislocation occurred in the posterolateral group and none in the anterolateral group; the difference was not statistically significant. Sheth et al. [9] reported an increased risk of dislocation with the posterolateral approach, especially in the presence of a lack of complete posterior soft-tissue healing. An anterolateral approach preserving anterior stabilising features may lead to improved joint stability. Lurch from the abductor was observed in a small percentage of patients from the anterolateral cohort. This finding may be explained by the transient weakness of the abductor muscle due to surgical exposure or traction during the anterolateral approach. Similar functional changes have been studied in comparative studies comparing lateral and posterolateral approaches to THA. Limb length discrepancy was more often seen in the posterolateral group, but the difference was not statistically significant. Patients operated on with the anterolateral technique demonstrated significantly earlier independent ambulation, indicating faster functional recovery. However, the anterolateral approach was associated with a longer operative time and a greater need for blood transfusion. Pincus et al. [5] reported that the surgical approach may influence perioperative outcomes, such as operative time and blood loss, especially in anterior-based techniques. The findings may be due to the increased technical difficulty and better soft-tissue management with the anterolateral approach. This study indicates that both anterolateral and posterolateral approaches to THA are safe and effective; however, the anterolateral technique provides earlier functional recovery and greater pain reduction in the early post-operative phase.
Limitations of the study:
The present study had certain limitations that should be considered while interpreting the findings. The sample size was relatively small, with only 60 patients, which may have limited the statistical power to detect minor differences between the anterolateral and posterolateral approaches, particularly regarding post-operative complications. As the study was conducted at a single tertiary care centre, the results may not be fully generalisable to other institutions or healthcare settings. The observational design without randomisation may have introduced selection bias, and the combined prospective-retrospective methodology may have resulted in variations in data collection and documentation. Retrospective data were dependent on hospital records, which may be associated with incomplete documentation or information bias. The follow-up duration was limited to 6 months; therefore, long-term outcomes, such as implant survival, aseptic loosening, polyethylene wear, osteolysis, late complications, and revision rates, could not be evaluated. In addition, the study included only patients with AVN of the femoral head, so the findings may not be applicable to THA performed for other indications, such as osteoarthritis or rheumatoid arthritis. Potential confounding factors, such as body mass index, smoking, alcohol intake, comorbidities, bone quality, surgeon experience, operative technique variation, rehabilitation protocol, and patient compliance, were not separately analysed. Objective assessments, such as muscle strength testing, gait analysis, abductor function evaluation, advanced imaging for component positioning, and broader patient-reported quality-of-life measures, were also not included. Hence, larger randomised multicentre studies with longer follow-up are required to confirm these findings and evaluate the long-term functional, radiological, and complication-related outcomes of both surgical approaches.
Both the anterolateral and posterolateral methods of THA yield substantial enhancements in functional outcomes and analgesia for patients with advanced AVN of the femoral head. The anterolateral technique was shown to enhance early functional recovery and result in a greater reduction in post-operative discomfort during short-term follow-up. Despite the increased operative duration and blood transfusion requirements associated with the anterolateral approach, the overall complication rates were similar between the two methods. Consequently, although the anterolateral approach may provide benefits for early rehabilitation, both techniques are safe and efficacious, and the selection of the surgical method should be tailored to the surgeon’s proficiency, the patient’s anatomy, and the clinical situation.
The anterolateral method in total hip arthroplasty may provide enhanced early functional recovery and superior analgesia relative to the posterolateral approach without increasing complication rates, indicating a preference for patients prioritising early rehabilitation. This study advocates for personalised selection of surgical approach, highlighting improved early outcomes when the anterolateral procedure is employed in appropriate patients.
References
- 1. Varacallo MA, Herzog L, Toossi N, Johanson NA. Ten-year trends and independent risk factors for unplanned readmission following elective total joint arthroplasty at a large urban academic hospital. J Arthroplasty 2017;32:1739-46. [Google Scholar] [PubMed]
- 2. Petek D, Hannouche D, Suva D. Osteonecrosis of the femoral head: Pathophysiology and current concepts of treatment. EFORT Open Rev 2019;4:85-97. [Google Scholar] [PubMed]
- 3. Lehmann TG, Engesaeter IØ, Laborie LB, Lie SA, Rosendahl K, Engesaeter LB. Total hip arthroplasty in young adults, with focus on Perthes’ disease and slipped capital femoral epiphysis: Follow-up of 540 subjects reported to the Norwegian Arthroplasty register during 1987-2007. Acta Orthop 2012;83:159-64. [Google Scholar] [PubMed]
- 4. Garofalo S, Morano C, Bruno L, Pagnotta L. A comprehensive literature review for total hip arthroplasty (THA): Part 2-material selection criteria and methods. J Funct Biomater 2025;16:184. [Google Scholar] [PubMed]
- 5. Pincus D, Jenkinson R, Paterson M, Leroux T, Ravi B. Association between surgical approach and major surgical complications in patients undergoing total hip arthroplasty. JAMA 2020;323:1070-6. [Google Scholar] [PubMed]
- 6. Al-Faifi JJ, Almuhanna NI, AlDera RM, Almohaimeed DH, Alshalan LZ, Alshaibani SK. Factors influencing decisions among the public related to the chosen surgeons for elective surgeries: A nationwide study. Surg Open Sci 2023;13:82-7. [Google Scholar] [PubMed]
- 7. Palan J, Beard DJ, Murray DW, Andrew JG, Nolan J. Which approach for total hip arthroplasty: Anterolateral or posterior? Clin Orthop Relat Res 2009;467:473-7. [Google Scholar] [PubMed]
- 8. Scalise A, Calamita R, Tartaglione C, Pierangeli M, Bolletta E, Gioacchini M, et al. Improving wound healing and preventing surgical site complications of closed surgical incisions: A possible role of incisional negative pressure wound therapy. A systematic review of the literature. Int Wound J 2016;13:1260-81. [Google Scholar] [PubMed]
- 9. Sheth D, Cafri G, Inacio MC, Paxton EW, Namba RS. Anterior and anterolateral approaches for THA are associated with lower dislocation risk without higher revision risk. Clin Orthop Relat Res 2015;473:3401-8. [Google Scholar] [PubMed]
- 10. Hax J, Leuthard L, Nauer S, Stadelmann VA, Leunig M, Rüdiger HA. Treatment options for persistent lateral femoral cutaneous nerve lesions after total hip arthroplasty via the direct anterior approach: Retrospective analysis with clinical assessment. Int Orthop 2025;49:1107-17. [Google Scholar] [PubMed]
- 11. Ukai T, Ebihara G, Watanabe M. Comparison of short-term outcomes of anterolateral supine approach and posterolateral approach for primary total hip arthroplasty: A retrospective study. J Orthop Traumatol 2021;22:6. [Google Scholar] [PubMed]
- 12. Teimouri M, Motififard M, Hatami S. Etiology of femoral head avascular necrosis in patients: A cross-sectional study. Adv Biomed Res 2022;11:115. [Google Scholar] [PubMed]
- 13. Goncharov EN, Koval OA, Bezuglov EN, Vetoshkin AA, Goncharov NG, Ramirez MJ, et al. Conservative treatment in avascular necrosis of the femoral head: A systematic review. Med Sci (Basel) 2024;12:32. [Google Scholar] [PubMed]
- 14. Ramadanov N, Voss M, Hable R, Hakam HT, Prill R, Salzmann M, et al. Postoperative Harris hip score versus Harris hip score difference in hip replacement: What to report? Orthop Surg 2025;17:3-21. [Google Scholar] [PubMed]
- 15. Amouzadeh Omrani F, Afzal S, Baroutkoub M, Salimi S, Barati H, Azadnajafabad S, et al. A comparative analysis of functional outcomes between lateral and posterolateral approaches in total hip arthroplasty. Adv Biomed Res 2025;14:13. [Google Scholar] [PubMed]
- 16. Bulzan M, Cavalu S, Voiță-Mekereș F, Hozan CT. Assessment of pain intensity after total hip arthroplasty using the visual analogue scale. J Med Life 2024;17:1049-53. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Managing Complications of Total Hip Arthroplasty for Avascular Necrosis Hip Performed Via Anterior Approach
July 1, 2026 Managing Complications of Total Hip Arthroplasty for Avascular Necrosis Hip Performed Via Anterior Approach June 1, 2026 Functional Outcomes of Total Hip Arthroplasty using Modified Harris Hip Score and Oxford Hip Score: A Prospective Study
June 1, 2026 Functional Outcomes of Total Hip Arthroplasty using Modified Harris Hip Score and Oxford Hip Score: A Prospective Study May 1, 2026 Direct Anterior THA with Leg Positioning Traction System for Avascular Necrosis: Technique and Early Outcomes
May 1, 2026 Direct Anterior THA with Leg Positioning Traction System for Avascular Necrosis: Technique and Early Outcomes March 1, 2026 Total Hip Arthroplasty in Lubumbashi (DR Congo), Outcomes in a Resource-Limited Setting
March 1, 2026 Total Hip Arthroplasty in Lubumbashi (DR Congo), Outcomes in a Resource-Limited Setting