
Tibialis anterior allografts, combined with transversal calcaneal anchoring, offer an effective and reliable solution for chronic Achilles tendon ruptures in older patients, ensuring functional recovery and minimizing complications associated with autograft use.
Dr. Nihar Modi, Department of Orthopaedic Surgeon, Sona Medical Centre, Jaslok Hospital and Research Centre, Criticare Asia Multispeciality Hospital and Research Centre, Mumbai, Maharashtra, India. E-mail: modi.nihar95@gmail.com
Abstract
Introduction: Chronic Achilles tendon ruptures are challenging to manage, particularly in older patients. This report describes the surgical repair of a chronic rupture using a tibialis anterior allograft in a 61-year-old male, emphasizing the technique and outcomes of this approach.
Case Report: A 60-year-old male with a 3-month-old Achilles tendon rupture presented with difficulty in walking, pain, and functional impairment. Imaging revealed a 2 cm gap. Surgical management included debridement and reconstruction using a tibialis anterior allograft anchored transversally through the calcaneus. At 2 years postoperatively, the patient had a full ankle range of motion, pain-free ambulation, and restored functionality.
Conclusion: Tibialis anterior allograft is a viable option for reconstructing chronic Achilles tendon ruptures with smaller gaps in older patients. It offers reliable functional recovery while minimizing the morbidity associated with autografts.
Keywords: Chronic Achilles tendon rupture, calcaneal tunnel technique, tibialis anterior tendon allograft, functional outcome.
The Achilles tendon being the strongest in the human musculoskeletal structure, once injured or torn can lead to significant impairment in one’s movement. Chronic Achilles tendon ruptures occur when the injury presents 4–6 weeks after the initial tear [1]. The Achilles tendon is reported to be the most commonly torn tendon, with this the load of people with chronic ruptures has increased. This is also due to the increased use of steroids for tendon-related ailments [1]. Myerson’s classification and evidence-based review guidelines suggest that defects <2 cm long can be managed conservatively or surgically with an end-to-end repair. Defects up to 5 cm are to be managed with V-Y lengthening, with or without a free tendon transfer depending on the defect and patient demographics free tendon graft procedures are recommended for gaps more than 6 cm, bridged with the use of a tendon transfer, alone or combined with a V-Y advancement [2]. These classifications are more suitable for acute tendon tears while implementing it for chronic tendon tears is still debatable. There are various surgical methods available to repair neglected Achilles tendon ruptures. In many cases, aligning the tendon ends to achieve an end-to-end anastomosis is challenging. Surgical management and technique are better decided after a proper pre-surgical assessment of the tear. Real-time ultrasound-assisted imaging and magnetic resonance imaging offer accurate tear gap analysis and, therefore, the course of treatment approach. Various techniques, such as augmentation with local tendon transfer, free tendon transfer, V-Y advances, and synthetic approaches, either open or endoscopic procedures, can be employed for the repair. In older patients, however, where the biological environment may be less favorable for healing, the treatment strategy must be tailored to optimize outcomes while minimizing complications [3,4]. This case report discusses the rationale, surgical technique, and clinical outcomes of using free anterior tibialis tendon allograft for a 2 cm gap in Achilles tendon repair in a 61-year-old patient, emphasizing the role of augmentation in optimizing recovery in older individuals.
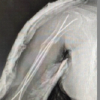
Our patient was a 61-year-old male who presented with a right unilateral closed Achilles tendon tear. The patient had twisted his right ankle 3 months back, experiencing challenges in walking and pain. Before presenting to our facility, the patient had received steroid injections as part of his initial treatment for Achilles Tendonitis elsewhere. Physical examination showed a positive Thompson test with a partial restriction of plantar flexion of the foot. Functional tests were characterized by an inability to perform a single heel rise, pain, and difficulty in walking and ascending stairs. Magnetic resonance imaging of the right ankle (Fig. 1) revealed a near total rupture of the right Achilles tendon, with a 2 cm gap 4.7 cm above the insertion point confirming chronic Achilles Tendon rupture.

A surgical line of management was chosen given that the patient had difficulty resuming routine activities. The surgical plan decided was, debridement and reconstruction using transversal calcaneal anchored anterior tibialis tendon allograft.
The patient was placed in the prone position after induction of spinal anesthesia. A pneumatic thigh tourniquet was used for the procedure, applied at the root of the operative right leg thigh. A longitudinal median incision was made ~6 cm above the insertion point and the incision was extended to the distal end of the Achilles tendon. The edges of the tear were freshened and cleaned of fibrous tissues. The degenerated part of the proximal stump was excised (Fig. 2). To prepare the calcaneal tunnel, the calcaneal tubercle was cleaned of soft tissues on either end followed by drilling a transverse tunnel. Side-by-side, the assistant surgeon thawed the frozen irradiated tibialis anterior allograft which was 28 cm long (Fig. 3a), and braided it. The braided tendon’s dimensions were (270 × 8 mm).


A beath pin with a loop was passed from the medial to the lateral side of the calcaneal tunnel. The prepared allograft was guided through the tunnel, brought to the proximal stump, cross-weaved through the torn tendoachilles mid substance, and the remaining allograft was sutured on both sides of the Achilles tendon using fiber wires (Fig. 3b, c, d). Additional sutures were secured at the anastomosis as required. The wound was subsequently irrigated and closed in layers. Immediate postoperative negative Thompson test was verified.
A circular short-leg plaster was placed with minimal plantarflexion. The patient was advised bed rest for the initial weeks postoperative. At 4 weeks postoperatively, passive range of motion exercises were started with physiotherapy. The patient was strictly advised to restrict weight-bearing, while allowed to perform guided functional rehabilitation ankle joint flexion and extension exercises. Post-operative imaging results showed a well-restored Achilles tendon with no dilation in the calcaneal tunnel. After 3 months, the patient could walk limitation-free and perform a heel rise without difficulty. At 1-year postoperative rehabilitation, the wound healed (Fig. 4), and he was able to return to his normal activities, and the 2-year post-operative follow-up showed a full ankle range of motion.

Achilles tendon is still a debilitating pathology that demands customized treatment modalities. Managing a chronic rupture is more complex and challenging compared to an acute rupture. Although various approaches have emerged in recent years, choosing an appropriate management strategy comes down to many factors including but not limited to physical activities, comorbidities, genetic predisposition, and age-sex factors [4]. Many studies for acute tears reported that Achilles ruptures managed operatively versus non-operatively show similar retear rates [5-9]. In addition, operative management is characterized by increased costs and risk of complications. Although evidence urges toward conservative management, the number of surgical managements for Achilles tendon ruptures remains steady. This could be due to the restoration of calf muscle strength and early ankle joint range of motion post-surgical management [10]. This early mobilization and function restoration becomes inevitable in cases of young high-demand patients like athletes and sportsmen. Limited studies have been conducted on chronic tears and have shown that surgical treatment of chronic tears leads to better functional outcomes [6,11]. Free tendon grafts are generally recommended for gaps more than 6 cm, and a gap of 2 cm ideally should be managed in an end-to-end fashion. However, achieving anastomosis in chronic Achilles tendon repair becomes challenging given the atrophy of the torn stump. Aging reduces tendon cell density, alters cell shape, weakens collagen structure, and leads to joint stiffness and reduced range of motion, compromising overall Achilles tendon strength and function. In addition, older age adds to the complexity of healing, the availability of strong autografts, and recovery [3,4]. Transversal calcaneal anchored reconstruction technique [12] has been reported to provide enhanced stability, reduced bone tunnel enlargement, improved functional recovery, and minimized adhesion and graft wear, making it an effective and durable solution for acute Achilles tendon rupture repair. We used a similar technique, however, with few modifications. We used a tibialis anterior allograft instead of an autograft. In addition, to minimize the risk of micro tears or disruption of native fibers, and preserve tendon integrity, we cross-weaved and sutured the allograft instead of Double-Z sutures. This simple technique is easy to execute as well as ensures balanced load-sharing after securing the graft on either side. Further studies and biomechanical assessment preferably in a large sample size are warranted to confirm the functional outcomes of chronic Achilles tendon repair using this technique.
Surgical management of chronic Achilles tendon rupture managed by transversal calcaneal anchored reconstruction technique using tibialis anterior allograft is a safe effective approach, especially in older patients with limited healing capacity and limited native tendon strength. The technique provides stable repair, restores functionality, and avoids complications associated with autograft harvesting. Long-term 2-year follow-up in this case demonstrates excellent clinical outcomes with minimal complications. Further studies are needed to validate these findings in a larger cohort.
- Chronic Achilles tendon ruptures require customized surgical approaches based on patient demographics, tear gap size, severity of pain, and functional demands
- Tibialis anterior allografts provide an alternative to autografts, reducing donor site morbidity while maintaining functional outcomes, especially in older patients
- Techniques like cross-weaving and transversal calcaneal anchoring enhance stability and load distribution, improving recovery and reducing the risk of re-rupture
- Proper postoperative rehabilitation is essential for optimizing outcomes and ensuring the restoration of functional mobility. Early mobilization in younger patients post this technique is highly plausible.
References
- 1.Adukia, V. and Jha, S. (2024) ‘Management of chronic achilles tendon ruptures’, Orthopaedics and Trauma, 38(1), pp. 11–17. doi:10.1016/j.mporth.2023.11.003. [Google Scholar | PubMed | CrossRef]
- 2.Feng SM, Maffulli N, Oliva F, Saxena A, Hao YF, Hua YH, et al. Surgical management of chronic Achilles tendon rupture: Evidence-based guidelines. J Orthop Surg Res 2024;19:132. [Google Scholar | PubMed]
- 3.Carmont, M.R. et al. (2020) ‘Age and tightness of repair are predictors of heel-rise height after Achilles tendon rupture’, Orthopaedic Journal of Sports Medicine, 8(3), pp. 1–8. doi:10.1177/2325967120909556. [Google Scholar | PubMed | CrossRef]
- 4.Sankova MV, Beeraka NM, Oganesyan MV, Rizaeva NA, Sankov AV, Shelestova OS, et al. Recent developments in Achilles tendon risk-analyzing rupture factors for enhanced injury prevention and clinical guidance: Current implications of regenerative medicine. J Orthop Transl 2024;49:289-307. [Google Scholar | PubMed]
- 5.Ochen Y, Beks RB, Van Heijl M, Hietbrink F, Leenen LP, Van Der Velde D, et al. Operative treatment versus nonoperative treatment of Achilles tendon ruptures: Systematic review and meta-analysis. BMJ 2019;364:k5120. [Google Scholar | PubMed]
- 6.Cienfuegos A, Holgado MI, Díaz del Río JM, González Herranz J, Lara Bullón J. Chronic achilles rupture reconstructed with achilles tendon allograft: A case report. J Foot Ankle Surg 2013;52:95-8. [Google Scholar | PubMed]
- 7.Soroceanu A, Glazebrook M, Sidhwa F, Aarabi S, Kaufman A. Surgical versus nonsurgical treatment of acute achilles tendon rupture: A meta-analysis of randomized trials. J Bone Joint Surg Am 2012;94:2136-43. [Google Scholar | PubMed]
- 8.Willits K, Amendola A, Bryant D, Mohtadi NG, Giffin JR, Fowler P, et al. Operative versus nonoperative treatment of acute achilles tendon ruptures: A multicenter randomized trial using accelerated functional rehabilitation. J Bone Joint Surg 2010;92:2767-75. [Google Scholar | PubMed]
- 9.Lantto I, Heikkinen J, Flinkkila T, Ohtonen P, Siira P, Laine V, et al. A prospective randomized trial comparing surgical and nonsurgical treatments of acute achilles tendon ruptures. Am J Sports Med 2016;44:2406-14. [Google Scholar | PubMed]
- 10.Crook, B. S., Varshneya, K., Meyer, L. E., Anastasio, A., Cullen, M. M., & Lau, B. C. (2023). Operative Versus Nonoperative Treatment of Acute Achilles Tendon Rupture: A Propensity Score–Matched Analysis of a Large National Dataset. Orthopaedic Journal of Sports Medicine, 11(2), 1–7. https://doi.org/10.1177/23259671231152904 [Google Scholar | PubMed | CrossRef]
- 11.Maffulli N, Ajis A. Management of chronic ruptures of the achilles tendon. J Bone Joint Surg 2008;90:1348-60. [Google Scholar | PubMed]
- 12.Xue H, Xiao F, Li R, Wu G, Zhu Z, Zhang C, et al. Transversal calcaneal anchored Achilles tendon reconstruction with free semitendinosus tendon autograft for acute rupture of Achilles tendon: Clinical evaluation. Sci Rep 2024;14:17815. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Outcome of Retrograde Titanium Elastic Nailing System in Shaft of Humerus Fractures: A Case Series
August 1, 2026 Outcome of Retrograde Titanium Elastic Nailing System in Shaft of Humerus Fractures: A Case Series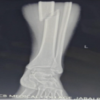 August 1, 2026 A Prospective Analysis of Physeal-Sparing Intramedullary Interlocking Nail for Adolescent Tibial Shaft Fractures
August 1, 2026 A Prospective Analysis of Physeal-Sparing Intramedullary Interlocking Nail for Adolescent Tibial Shaft Fractures August 1, 2026 Outcome Analysis of Loop Endobutton Repair for Acromioclavicular Joint Dislocation
August 1, 2026 Outcome Analysis of Loop Endobutton Repair for Acromioclavicular Joint Dislocation July 1, 2026 All-Inside Versus Inside-Out Meniscal Repair: A Comparative Study of Healing Rates And Functional Outcomes
July 1, 2026 All-Inside Versus Inside-Out Meniscal Repair: A Comparative Study of Healing Rates And Functional Outcomes