
Both all-inside and inside-out meniscal repair techniques provide excellent healing rates and functional recovery. While the all-inside technique offers shorter operative time and fewer neurovascular complications, the choice of repair method should be individualised based on tear characteristics, patient factors, and surgeon expertise.
Dr. Prithviraj Deshmukh, Department of Trauma and Orthopaedics, Royal Lancaster Infirmary, Lancaster, United Kingdom. E-mail: drpdeshmukh012@gmail.com
Abstract
Background: Meniscal injuries rank as one of the most frequent knee injuries, which can be repaired through preservation as the best method to maintain knee joint health and prevent long-term joint deterioration. The all-inside and inside-out meniscal repair techniques represent the most commonly used surgical methods for meniscal tissue restoration. The existing research shows ongoing disagreement about which method of treatment produces better healing results and functional improvements and surgical time efficiency and rate of medical complications.
Methods: This prospective comparative study included 50 patients with meniscal tears who underwent arthroscopic repair. Patients were divided into two groups: All-inside repair (n = 25) and inside-out repair (n = 25). Demographic data, tear characteristics, operative time, complications, healing rates, and functional outcomes were assessed. Functional outcomes were evaluated using the Lysholm knee score and the International Knee Documentation Committee (IKDC) score. Patients were followed up for 6 months postoperatively.
Results: The majority of the patients were aged 26–35 years (38%) with a male predominance (70%). Operative time was significantly lower in the all-inside group (42 ± 6 min) compared to the inside-out group (58 ± 8 min). Meniscal healing was observed in 84% of patients in the all-inside group and 92% in the inside-out group. Functional outcomes improved significantly in both groups, with Lysholm scores increasing to 90 ± 5 (all-inside) and 92 ± 4 (inside-out), and IKDC scores to 88 ± 6 and 90 ± 5, respectively. Complications were fewer in the all-inside group, with no neurovascular injuries reported, whereas the inside-out group had a higher incidence of such complications. Return to pre-injury activity was achieved in 80% of patients overall.
Conclusion: Both all-inside and inside-out meniscal repair techniques demonstrated excellent healing and functional outcomes. The all-inside technique provided a shorter operative time and fewer complications, whereas the inside-out technique showed slightly higher healing rates.
Keywords: All-inside technique, functional outcome, meniscal repair, inside-out technique, knee arthroscopy.
Meniscal injuries are among the most common intra-articular knee pathologies encountered in orthopaedic practice, particularly affecting young, active individuals and athletes. The menisci play a crucial role in load transmission, shock absorption, joint stability, lubrication, and proprioception of the knee joint. Traditionally, meniscectomy was a popular surgical procedure to manage meniscal ruptures, but long-term follow-up investigations showed that meniscectomy had a strong connection with the early onset of osteoarthritis, leading to a paradigm shift to meniscal preservation and repair when possible [1]. This has been further enhanced by the progress in arthroscopic procedures and instrumentation that has resulted in the creation of different meniscal repair procedures, most notable being inside-out and all-inside. The inside-out meniscal repair technique has long been regarded as the best, as it has high fixation and good results in terms of healing. In this procedure, the sutures are placed through the intra-articular aspect of the knee to the extra-articular aspect, and the procedure entails a posterior incision to retrieve the sutures and weave them over the joint capsule. Although the technique has high success rates, it is technically challenging, time-consuming, and has associated risks such as neurovascular damage, especially to vessels such as the saphenous nerve and popliteal vessels [2]. However, a number of studies have demonstrated excellent strength of biomechanical effect and consistent healing rates with the inside-out method, particularly in tears that are in the vascular regions of the meniscus [3]. Conversely, the all-inside meniscal repair method has become popular in recent years because of its minimally invasive nature and less time spent on the operation. It is a method that uses pre-loaded devices that are arthroscopically inserted and will fix within the joint completely without using additional incisions. The benefits of the all-inside approach include a reduction in the morbidity of surgery, a lower likelihood of neurovascular events, and patient comfort [4]. Nonetheless, issues have been expressed about the biomechanical performance of fixation, complications related to implants, and the increased cost of such devices [5]. Older models of all-inside devices were linked to increased failure rates, but newer models have shown better results in comparison with conventional methods [6]. Numerous factors affect the healing of meniscal repairs, such as tear location, age of the patient, vascular supply, and other injuries, such as anterior cruciate ligament (ACL) tears. Tears in the peripheral red-red or red-white areas have a greater healing potential because they are more abundant in blood, and central tears in the white-white areas have a poorer healing potential [7]. Furthermore, concomitant ACL reconstruction has been reported to improve meniscal healing, which may be a result of increased vascular response and biological augmentation at the site of repair [8]. Consequently, these variables should be taken into consideration in the comparison of the healing rates and functional outcomes of different repair techniques. Validated scoring systems, including Lysholm knee score, International Knee Documentation Committee (IKDC) score, and Tegner activity scale, are usually used to determine the functional outcomes after meniscal repair. The improvement in both inside-out and all-inside methods has been positive in these scores, which are a sign of successful restoration of the knee functionality [9]. Comparative studies have, however, yielded mixed results, with some showing no difference in the results of the two methods and others showing slightly higher healing rates with inside-out repairs [10]. The differences could be explained by the differences in study design, patient selection, properties of tears, and follow-up period. With the growing interest in minimally invasive surgery and quick recovery, the all-inside procedure is still in development and is an alternative to the conventional inside-out method. However, the decision to repair or not to repair frequently hinges on the experience of the surgeon, the arrangement of the tear, and intraoperative factors. Thus, a full comparative study of healing rates and functional outcomes of all-inside and inside-out meniscal repair methods is necessary to inform clinical decision-making and maximise patient outcomes. This research is expected to add to the existing literature by critically analysing and comparing these two commonly used methods in terms of effectiveness and clinical usability. Therefore, the present study was conducted to compare healing rates, functional outcomes, operative time, and complications between all-inside and inside-out meniscal repair techniques.
Study design:
This prospective comparative observational study was conducted to evaluate and compare the healing rates and functional outcomes of all-inside versus inside-out meniscal repair techniques. The study protocol received approval from the institutional ethics committee, and written informed consent was obtained from all participants before enrolment. The research was carried out in the orthopedics department of a tertiary care teaching hospital equipped with advanced arthroscopic facilities, and was completed over a period of 18 months, including patient recruitment, surgical intervention, and follow-up.
Inclusion criteria:
- Between 18 and 50 years
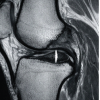
- Patients with meniscal tears who have been diagnosed through magnetic resonance imaging (MRI) and clinical examination
- Patients who have undergone arthroscopic meniscal repair (all-inside or inside-out repair)
- Patients who have informed consent and can follow up.
Exclusion criteria:
- Advanced knee osteoarthritis patients
- Patients who had knee surgery on the affected side
- Patients who have concomitant ligament injuries to be reconstructed (excluding isolated ACL injuries, included based on protocol)
- Patients with systemic inflammatory joint diseases (e.g., rheumatoid arthritis)
- Patients who are not willing or able to follow up.
Study sampling:
The study used a consecutive sampling method to get access to eligible patients who presented themselves to the orthopedic department within the timeframe of the study. Until the targeted sample size was reached, all patients meeting the inclusion criteria and giving informed consent were included. This approach made it feasible and reduced selection bias in a clinical context.
Study sample size:
The study consisted of a total of 50 patients. The sample size was determined based on expected case availability, study feasibility, and comparable previous studies evaluating meniscal repair outcomes.
Study groups:
The population of the study was split into two groups depending on the type of surgery used:
- Group A: Patients who had all-inside meniscal repair
- Group B: Patients who had inside-out meniscal repair.
There were 25 patients in each group. The surgeon allocated to the respective group was by choice nature of tears, operability factors, and other factors, as opposed to randomisation.
Study parameters:
The main parameters that were measured in the research were the rates of meniscal healing and functional outcomes. Clinical and radiological (where indicated) assessment of healing was done by MRI. The standardised scoring systems were used to measure functional outcomes, including the Lysholm Knee Score and the IKDC score. Secondary parameters were the operative time, postoperative complications, and the level of return to activity.
Study procedure:
Every patient was thoroughly preoperatively evaluated, with clinical examination and MRI of the affected knee. Meniscal repair was done using spinal or general anaesthesia. The meniscus in the all-inside technique was repaired with preloaded suture devices, and a complete repair was carried out within the joint. The inside-out method involved passing sutures through small posterior incisions to the outside and tying them over the capsule.
Study data collection:
A structured pro forma designed to gather data was used in the study. Basic demographic information, clinical observations, MRI reports, intraoperative observations, and surgical data were taken. Follow-up data comprised the outcomes of clinical examination, functional scores, and complications. To guarantee consistency and completeness, data were gathered at specified times.
Data analysis:
The data obtained were inputted in Microsoft Excel and analysed with the help of the right statistical programs, like the Statistical Package for the Social Sciences. The data were summarised using descriptive statistics such as mean, standard deviation, frequency, and percentage. Appropriate statistical tests, like the independent t-test of the continuous variable and the chi-square test of the categorical variable, were used in comparing the two groups. A P-value of below 0.05 was said to be statistically significant.
A total of 50 patients with meniscal tears underwent arthroscopic meniscal repair and were equally allocated to the all-inside (n = 25) and inside-out (n = 25) groups. The majority of the patients were aged 26–35 years (38%), with a male predominance (70%). Right knee involvement was slightly more common than left knee involvement (54% vs. 46%). Longitudinal tears were the most frequently encountered tear pattern (46%), followed by bucket-handle tears (26%). Baseline demographic and injury characteristics were comparable between the two groups (Table 1).
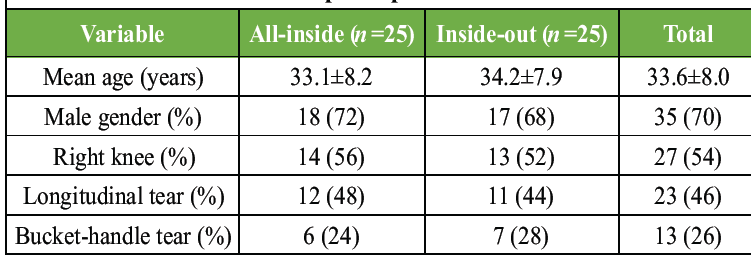
Table 1: Baseline demographic and injury characteristics of study participants
The mean operative time was significantly shorter in the all-inside group compared to the inside-out group (42 ± 6 min vs. 58 ± 8 min). Postoperative complications were infrequent in both groups; however, neurovascular injury was observed only in the inside-out group (8%), whereas no such complication occurred in the all-inside group. Overall, meniscal healing was achieved in 44 patients (88%) at 6 months’ follow-up, with healing rates of 84% in the all-inside group and 92% in the inside-out group (Fig. 1).
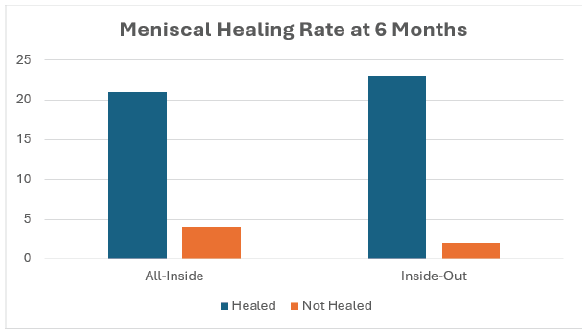
Figure 1: Comparison of meniscal healing rates at 6 months follow-up between the all-inside and inside-out repair groups.
Both techniques resulted in substantial functional improvement. The mean Lysholm knee score improved from 58 ± 7 to 90 ± 5 in the all-inside group and from 60 ± 6 to 92 ± 4 in the inside-out group. Similarly, the mean IKDC score improved from 52 ± 8 to 88 ± 6 and from 54 ± 7 to 90 ± 5, respectively. Return to pre-injury activity level was achieved in 80% of patients, including 76% in the all-inside group and 84% in the inside-out group. Functional outcome scores were comparable between groups, with a slight advantage observed in the inside-out repair cohort (Table 2 and Fig. 2).
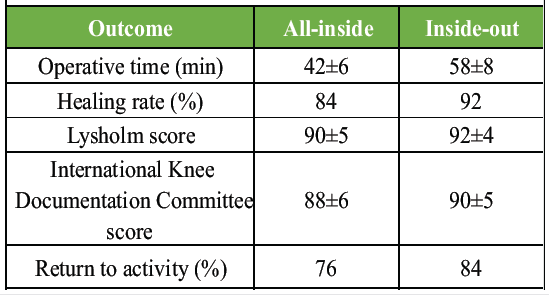
Table 2: Clinical and functional outcomes at 6 months
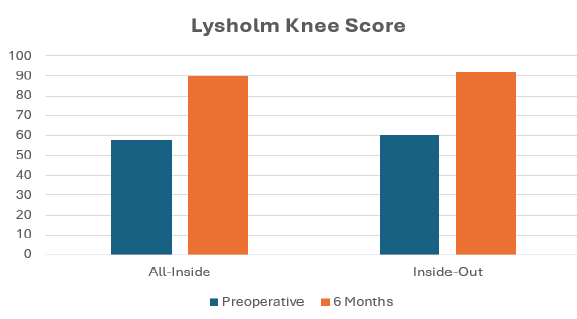
Figure 2: Comparison of functional outcomes (Lysholm knee score and International Knee Documentation Committee score) between the all-inside and inside-out repair groups at final follow-up.
The current prospective comparative analysis compared the healing rates and functional outcomes of all-inside and inside-out meniscal repair methods in 50 patients, which was very informative on the effectiveness and safety in comparison with each other. The study demographic showed that most patients fell within the 26-35 years (38%) and 36-45 years (26%) age brackets, with 70 being males. This is consistent with the epidemiology of known meniscal injuries, as they are more prevalent in young active males because they are exposed to more activities and sports. The similarity in the demographic factors of the two groups provided the assurance that the results were mainly due to the surgical methods and not the confounding factors. Longitudinal tears (46% of the total in the present study) were the most frequent, then bucket-handle tears (26%). The equal distribution of tear types between the all-inside and inside-out groups strengthened the validity of the comparison, as tear morphology significantly influences healing potential. One of the key findings of this study was the significantly shorter operative time observed in the all-inside group (42 ± 6 min) compared to the inside-out group (58 ± 8 min). This finding is strongly supported by previous literature. A meta-analysis by Elmallah et al. [11] reported that the inside-out technique had a significantly higher mean operating time compared to the all-inside technique. Similarly, Vint et al. [12] demonstrated a significant reduction in operative time favouring all-inside repair (ratio of means 0.62, P = 0.0002). These findings corroborate the results of the present study and highlight the procedural efficiency and minimally invasive advantage of the all-inside technique. With regard to complications, the present study observed a lower complication rate in the all-inside group, with no cases of neurovascular injury, compared to two cases reported in the inside-out group. This is consistent with existing evidence indicating a higher risk of nerve injury associated with the inside-out technique. Vint et al. reported that nerve injury was significantly more common in inside-out repairs, with an 85% reduction in odds when using the all-inside technique (odds ratio (OR) 0.15, P = 0.0013). Similarly, Grant et al. [13] observed a higher prevalence of nerve injury in inside-out repairs (9%) compared to all-inside repairs (2%). In the present study, although infection and knee stiffness were noted in both groups, the overall complication profile favoured the all-inside technique, supporting its safety and minimally invasive nature. The major result of meniscal healing exhibited successful results for both techniques used in treatment, where an 84% meniscus healing rate was recorded among those who underwent all-inside treatment, while for those treated through inside-out surgery, a 92% healing rate was achieved. The difference between the two healing rates was insignificant. This observation is consistent with multiple prior studies. Vint et al. found no significant difference in meniscal healing rates between the two techniques (OR 1.26, P = 0.61). Similarly, Fillingham et al. [14] reported no significant differences in clinical failure (11% vs 10%) or anatomic failure (13% vs 16%) between inside-out and all-inside repairs. Grant et al. [13] demonstrated comparable clinical failure rates (17% vs. 19%) between the two techniques. These findings collectively reinforce that both techniques provide reliable and comparable healing outcomes. Functional outcomes in the present study showed significant improvement in both groups. The Lysholm Knee Score improved from 58 ± 7 to 90 ± 5 in the all-inside group and from 60 ± 6 to 92 ± 4 in the inside-out group. Similarly, IKDC scores improved from 52 ± 8 to 88 ± 6 and from 54 ± 7 to 90 ± 5 in the respective groups. Although the inside-out group demonstrated slightly higher scores, the differences were minimal. These findings are in agreement with previous studies. Fillingham et al. reported comparable functional outcomes, with Lysholm scores of 88.0 ± 3.5 for inside-out and 90.4 ± 3.7 for all-inside repairs. Elmallah et al. [11] found comparable IKDC and Tegner scores between the two techniques. Furthermore, Samuelsen et al. [15] reported no significant differences in IKDC and Tegner scores between the groups at midterm follow-up. These consistent findings across studies confirm that both techniques achieve excellent functional recovery. Return to activity is an important functional outcome, and in the present study, 80% of patients returned to their pre-injury activity level, with slightly higher rates in the inside-out group (84% vs. 76%). This finding is consistent with the overall comparable functional outcomes reported in the literature. Samuelsen et al. demonstrated similar clinical outcomes and retear-free survival between the two techniques, with equal failure rates of 20% in both groups. This implies that the repair method does not play a significant role in long-term success, but other factors (i.e., the age of the patient, the nature of tears, and rehabilitation protocols) may have an impact. The other significant factor that has been noted as significant in the past studies is that the biological and tear-related factors may be important in influencing the healing outcomes, but not the surgical technique itself. According to Grant et al. [13], the variation in the speed of healing is more reliant on the tear pattern and related ACL repair as opposed to the repair technique itself. This confirms the results of the current research whereby the distribution of the tears was similar between the groups and probably led to the similar healing results. On the whole, the results of this research are in line with the existing literature, proving that all-inside and inside-out meniscal repair methods are equally effective and have good healing and functional outcomes. Although the inside-out method exhibited a low but significantly higher rate of healing (92% vs. 84%) and slightly better functional scores, the all-inside method had a major benefit in terms of less time spent at the operating table (42 vs. 58 min) and fewer neurovascular complications. These findings indicate that the type of technique used should be customised depending on the patient, type of tear, and the level of expertise of the surgeon. The all-inside method could be favoured due to its low invasiveness and safety profile, but the inside-out method is also a safe method of obtaining a good fixation in the right situations. The strengths of this study include its prospective comparative design, standardised surgical techniques, and use of validated functional outcome measures. However, several limitations should be acknowledged. The relatively small sample size (n = 50), single-centre setting, and non-randomised allocation of patients may limit the statistical power and generalisability and introduce potential selection bias. The short follow-up period of 6 months precluded assessment of long-term healing, re-tear rates, osteoarthritis progression, implant-related complications, and revision surgery. Potential surgeon-related bias, lack of blinding of patients and outcome assessors, variability in tear morphology, and the absence of subgroup analyses based on tear location, size, chronicity, age, sex, or activity level may have influenced outcomes. Inclusion of patients with concomitant ACL injuries could have acted as a confounding factor, while MRI confirmation of healing was not uniformly available for all patients. Functional assessment was limited to Lysholm and IKDC scores, rehabilitation compliance was not objectively monitored, and cost-effectiveness was not evaluated. Therefore, larger multicentre randomised studies with longer follow-up are needed to validate these findings.
Both all-inside and inside-out meniscal repair techniques demonstrated excellent healing rates and functional outcomes. While the inside-out technique showed slightly higher healing rates and functional scores, the all-inside technique offered the advantages of shorter operative time and fewer complications. Therefore, the choice of repair technique should be individualised based on tear characteristics, patient factors, and surgeon expertise.
Both all-inside and inside-out meniscal repair techniques provide reliable healing and good functional recovery. The all-inside technique may reduce operative time and neurovascular complications.
References
- 1. Ahn JH, Wang JH, Yoo JC. Arthroscopic all-inside suture repair of medial meniscus lesion in anterior cruciate ligament–deficient knees: Results of second-look arthroscopies in 39 cases. Arthroscopy 2004;20:936-45. [Google Scholar] [PubMed]
- 2. Albrecht-Olsen P, Kristensen G, Tormala P. Meniscus bucket-handle fixation with an absorbable Biofix tack: Development of a new technique. Knee Surg Sports Traumatol Arthrosc 1993;1:104-6. [Google Scholar] [PubMed]
- 3. Allen PR, Denham RA, Swan AV. Late degenerative changes after meniscectomy. Factors affecting the knee after operation. J Bone Joint Surg Br 1984;66:666-71. [Google Scholar] [PubMed]
- 4. Austin KS. Complications of arthroscopic meniscal repair. Clin Sports Med 1996;15:613-9. [Google Scholar] [PubMed]
- 5. Dzidzishvili L, Jackson GR, Allende F, Mameri ES, Allahabadi S, Chahla J. Meniscal radial tears repaired with all-inside and inside-out techniques result in improved clinical outcome scores, but inside-out repairs may be associated with higher failure rates clinically and on second-look arthroscopy: A systematic review. Arthroscopy 2025;41:1667-79. [Google Scholar] [PubMed]
- 6. Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav Res 2011;46:399-424. [Google Scholar] [PubMed]
- 7. Borque KA, Laughlin MS, Webster E, Jones M, Pinheiro VH, Williams A. A comparison of all-inside and inside-out meniscal repair in elite athletes. Am J Sports Med 2023;51:579-84. [Google Scholar] [PubMed]
- 8. Miller AC, Batiste AJ, McQuivey KS, McCarty EC. All-inside versus inside-out suture techniques in athletes undergoing arthroscopic meniscal repair: A systematic review and meta-analysis. Orthop J Sports Med 2025;13:23259671251361488[2.1]. [Google Scholar] [PubMed]
- 9. Barber FA, Herbert MA, Schroeder FA, Aziz-Jacobo J, Sutker MJ. Biomechanical testing of new meniscal repair techniques containing ultra high-molecular weight polyethylene suture. Arthroscopy 2009;25:959-67. [Google Scholar] [PubMed]
- 10. Villarreal‐Espinosa JB, Berreta RS, Pallone L, Rubin J, Allende F, Gómez‐Verdejo F, et al. Failure and complication rates following meniscal all‐inside and inside‐out repairs: A systematic review and meta‐analysis. Knee Surg Sports Traumatol Arthrosc 2025;33:1992-2009. [Google Scholar] [PubMed]
- 11. Elmallah R, Jones LC, Malloch L, Barrett GR. A meta-analysis of arthroscopic meniscal repair: Inside-out versus outside-in versus all-inside techniques. J Knee Surg 2019;32:750-7. [Google Scholar] [PubMed]
- 12. Vint H, Quartley M, Robinson JR. All-inside versus inside-out meniscal repair: A systematic review and meta-analysis. Knee 2021;28:326-37. [Google Scholar] [PubMed]
- 13. Grant JA, Wilde J, Miller BS, Bedi A. Comparison of inside-out and all-inside techniques for the repair of isolated meniscal tears: A systematic review. Am J Sports Med 2012;40:459-68. [Google Scholar] [PubMed]
- 14. Fillingham YA, Riboh JC, Erickson BJ, Bach BR Jr., Yanke AB. Inside-out versus all-inside repair of isolated meniscal tears: An updated systematic review. Am J Sports Med 2017;45:234-42. [Google Scholar] [PubMed]
- 15. Samuelsen BT, Johnson NR, Hevesi M, Levy BA, Dahm DL, Stuart MJ, et al. Comparative outcomes of all-inside versus inside-out repair of bucket-handle meniscal tears: A propensity-matched analysis. Orthop J Sports Med 2018;6:2325967118779045. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2026 Functional Recovery after Arthroscopic Management of Meniscal Tears
March 1, 2026 Functional Recovery after Arthroscopic Management of Meniscal Tears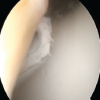 February 1, 2026 Knee Arthroscopy in Morbidly Obese Patients: Perioperative Challenges and Technical Considerations to Optimize Outcomes
February 1, 2026 Knee Arthroscopy in Morbidly Obese Patients: Perioperative Challenges and Technical Considerations to Optimize Outcomes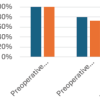 July 1, 2026 Role of Meniscal Ramp Lesion Repair in Preventing Residual Instability after Anterior Cruciate Ligament Reconstruction
July 1, 2026 Role of Meniscal Ramp Lesion Repair in Preventing Residual Instability after Anterior Cruciate Ligament Reconstruction June 1, 2026 Comparison of Radial Head Prosthesis versus Excision in Comminuted Radial Head Fractures: A Retrospective Comparative Study
June 1, 2026 Comparison of Radial Head Prosthesis versus Excision in Comminuted Radial Head Fractures: A Retrospective Comparative Study