
Phrenic nerve palsy can occur as a complication of anterior cervical discectomy and fusion (ACDF) in cervical spine trauma. Management of the same.
Dr. Vishal Kumar, Additional Professor, Department of Orthopaedics, PGIMER Chandigarh, India. E-mail: drkumarvishal@gmail.com
Abstract
Introduction: Phrenic nerve palsy is a rare but potentially serious complication. The clinical presentation can vary from being asymptomatic to severe respiratory distress requiring mechanical complication. In the Anglophone literature, there is only a single case report of bilateral phrenic nerve injury as a complication following anterior cervical discectomy and fusion (ACDF).
Case Report: This case report describes a 52-year-old female who developed right-sided phrenic nerve palsy after undergoing ACDF for cervical spine trauma. The patient had respiratory distress immediately after surgery and Ultrasonography and X-rays revealed Rt phrenic nerve palsy. To the best of our knowledge, this is the first case of unilateral phrenic nerve palsy after ACDF at the C5-C6 level.
Conclusion: Unilateral phrenic nerve palsy probably occurred as a complication of ACDF for cervical spine trauma. Phrenic nerve palsy should be kept in mind as a serious complication of spinal surgery.
Keywords: Phrenic nerve palsy, anterior cervical discectomy and fusion, cervical spine trauma, respiratory distress, post-operative complication.
Anterior cervical discectomy and fusion (ACDF) is the most commonly performed anterior-based surgical procedure which is usually well-tolerated and improves functional scores in patients of cervical spine pathology [1]. Despite its proven safety as a surgical procedure, there are a number of complications that can occur in the immediate perioperative period, including dysphagia 5.3%, esophageal perforation 0.2%, recurrent laryngeal nerve palsy 1.3%, infection 1.2%, adjacent segment disease 8.1%, pseudarthrosis 2.0%, graft or hardware failure 2.1%, cerebrospinal fluid leak 0.5%, hematoma 1.0%, Horner syndrome 0.4%, C5 palsy 3.0%, vertebral artery injury 0.4%, and new or worsening neurological deficit 0.5% [2]. Injury to the phrenic nerve is an extremely rare but potentially catastrophic complication [1]. The phrenic nerve supplies the diaphragm. Its injury can vary from being asymptomatic to significant respiratory compromise, manifesting as failure to wean from the ventilator post-operatively or emergent, unplanned reintubations. We report unilateral dysfunction of the diaphragm resulting from unilateral right-sided phrenic nerve palsy after anterior decompression and fusion for C5-C6 traumatic anterolisthesis.
An active, previously healthy 52-year-old female with a history of fall from height 1 month back, presented in the Out Patient Department, with complaints of decreased sensations and inability to move all the limbs. She was being treated in a local hospital conservatively with a Philadelphia collar. However, since there was no improvement even after 1 month, the patient and attendant sought consultation at our center. Physical examination revealed a conscious, oriented patient with complete sensory and motor loss below C5 with bladder and bowel dysfunction (ASIA-A). Neurologic examinations showed symmetrically active 2+ deep tendon reflexes and extensor plantar responses.
Radiologic findings
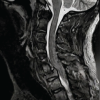
Radiographs showed C5-C6 anterolisthesis with decreased physiologic cervical lordosis (Fig. 1). Computerized tomography revealed grade II anterolisthesis of C5 over C6 vertebral body with dislocation of bilateral C5-C6 facet and uncovertebral joints causing spinal canal stenosis (Fig. 2). Magnetic resonance imaging additionally demonstrated cord contusion with upstream cord edema up to C2-C3 (Fig. 3).



The patient was planned for elective ACDF at the C5-C6 level. Pre-anesthetic check-up before surgery was done. The patient was conscious oriented and breathing spontaneously. Her room air saturation was 98%. All her investigations including chest X-ray (Fig. Pre-operative chest X-ray) and ABG were normal. She was maintaining hemodynamics with no evidence of sepsis.
Surgical procedure
The patient underwent ACDF at the C5-C6 level with a typical Smith Robinson approach from the left side. The procedure included anterior cervical discectomy and placement of an inter body fusion cage. Anesthesia induction was uneventful and the patient was intubated with a posterior collar in situ using a video laryngoscope. Injection dexamethasone was administered intra operatively. The whole surgical procedure was also uneventful. The cardiovascular and respiratory parameters were stable during the intraoperative period. The patient was extubated and shifted to the recovery room with stable hemodynamics and respiratory parameters.
Post-operative course
On the first post-operative day, the patient had shortness of breath with a fall in saturation up to 87% prompting immediate action and further investigation. Physical examination revealed labored breathing with diminished breath sounds over the right lung base. There was no change in the neuromuscular status of the patient.
Diagnostic evaluation
To evaluate her respiratory symptoms, immediate ABG was done which revealed hypoxia with hypercarbia. Bedside lung Ultrasonography was done to rule out pulmonary edema, atelectasis, or effusion. When the diaphragm was noticed on both sides, it showed absent movement of the diaphragm on the right side and normal excursion of the diaphragm on the left side suggestive of right phrenic nerve palsy (Fig. 4). A chest X-ray was performed, which showed an elevated right hemidiaphragm (Fig. 5) confirming the diagnosis.
Management
The patient was intubated in view of respiratory distress and hypoxia. She was closely monitored for any signs of worsening respiratory distress. Injection dexamethasone was also added.
Outcome
The patient’s condition showed gradual improvement over a few days. Over 5 days, she was weaned from respiratory support. Continued chest physiotherapy was recommended to accelerate her recovery.
C5 nerve palsy can occur in up to 30% of cervical surgery cases, but the exact frequency of phrenic nerve palsy following these surgeries is not well known [3,4]. This complication can arise from both anterior and posterior surgical approaches, as well as from laminectomies and fusion procedures. The outcome of the nerve dysfunction can vary from temporary palsy to permanent damage, although phrenic nerve weakness is usually not clinically significant. Only a few cases have been reported in the literature drawing similar inferences. The phrenic nucleus forms the grey matter of the cervical ventral horn extending from the rostrocaudal extent of C3 to the caudal part of C5. The phrenic nucleus is composed of clusters of longitudinally oriented cells of medium size, occupying the most medial portion of the ventromedial group of cells in the gray matter of the ventral horn of the C3, C4, and C5. Together these clusters constitute a straight column almost parallel to the ventral longitudinal fissure [5]. Usually, these patients are difficult to wean, but in our case patient was extubated and developed respiratory distress after approximately 24 h of the surgery. This suggests spinal edema as the most probable cause which developed gradually and settled within a few days after starting steroids [6]. Other causes could be direct damage to nerve roots from mechanical, electrical, or thermal trauma during surgery, reduced blood flow to nerve roots, spinal cord rotation before and after surgery, injury from the return of blood flow after decompression, stretching injuries due to the movement of the spinal cord, and tethering of nerve roots after decompression. While none of these theories have been conclusively proven as the main cause, research and clinical studies suggest that nerve root traction or tension after decompression might be a key factor [4,7]. The possible causes of phrenic nerve palsy after ACDF include bilateral C4 nerve root stretching, injury to the grey matter in the ventral horn, changes in blood circulation due to spinal edema, and reimpingement on the spinal cord at the cranial part of the decompression site [8]. In our case, it was more likely due to the C4 nerve stretching due to manipulation during the surgery since the injury was 1 month old and nerve root impingement due to post-surgery hematoma. Phrenic nerve palsy following ACDF, while rare, can significantly impact a patient’s post-operative recovery and quality of life. Early diagnosis is critical for effective management and point-of-care ultrasound helps in early diagnosis when portable chest ray might be delayed and dynamic fluoroscopy might not be feasible [9].
Unilateral phrenic nerve palsy probably occurred as a complication of anterior cervical decompression and fusion for cervical spine trauma. Phrenic nerve palsy should be kept in mind as a serious complication of spinal surgery. This case highlights the importance of eager awareness and early recognition of phrenic nerve palsy following ACDF. While this complication is highly uncommon, timely diagnosis and appropriate management can enhance recovery and mitigate complications.
Occurrence of phrenic nerve palsy following ACDF is a rare, but possible complication. Hence, timely diagnosis and appropriate management of palsy can help mitigate a disaster and improve the overall prognosis of the patient. It is suggested to prolong the ventilator use for patients suffering from phrenic nerve palsy.
References
- 1.McAfee PC, Reah C, Gilder K, Eisermann L, Cunningham B. A meta-analysis of comparative outcomes following cervical arthroplasty or anterior cervical fusion: Results from 4 prospective multicenter randomized clinical trials and up to 1226 patients. Spine (Phila Pa 1976) 2012;37:943-52. [Google Scholar | PubMed]
- 2.Timothy JY, Swong K, Park P. Complications of anterior cervical spine surgery: A systematic review of the literature. J Spine Surg 2020;6:302-22. [Google Scholar | PubMed]
- 3.Hitchon PW, Moritani T, Woodroffe RW, Abode-Iyamah K, Tecle NE, Noeller J, et al. C5 palsy following posterior decompression and instrumentation in cervical stenosis: Single center experience and review. Clin Neurol Neurosurg 2018;174:29-35. [Google Scholar | PubMed]
- 4.Jack A, Ramey WL, Dettori JR, Tymchak ZA, Oskouian RJ, Hart RA, et al. Factors associated with C5 palsy following cervical spine surgery: A systematic review. Global Spine J 2019;9:881-94. [Google Scholar | PubMed]
- 5.Fujibayashi S, Shikata J, Yoshitomi H, Tanaka C, Nakamura K, Nakamura T. Bilateral phrenic nerve palsy as a complication of anterior decompression and fusion for cervical ossification of the posterior longitudinal ligament. Spine (Phila Pa 1976) 2001;26:E281-6. [Google Scholar | PubMed]
- 6.Hendershot KA, O’Phelan KH. Respiratory complications and weaning considerations for patients with spinal cord injuries: A narrative review. J Pers Med 2022;13:97. [Google Scholar | PubMed]
- 7.Fuller DD, Rana S, Smuder AJ, Dale EA. The phrenic neuromuscular system. Handb Clin Neurol 2022;188:393-408. [Google Scholar | PubMed]
- 8.Moon AS, Pearson JM, Pittman JL. Phrenic nerve palsy after cervical laminectomy and fusion. N Am Spine Soc J 2020;4:100022. [Google Scholar | PubMed]
- 9.Di Serafino M, Dell’Aversano Orabona G, Caruso M, Camillo C, Viscardi D, Iacobellis F, et al. Point-of-care lung ultrasound in the intensive care unit-the dark side of radiology: Where do we stand? J Pers Med 2023;13:1541. [Google Scholar | PubMed]
- 10.McAfee PC, Reah C, Gilder K, Eisermann L, Cunningham B. A meta-analysis of comparative outcomes following cervical arthroplasty or anterior cervical fusion: Results from 4 prospective multicenter randomized clinical trials and up to 1226 patients. Spine (Phila Pa 1976) 2012;37:943-52. [Google Scholar | PubMed]
- 11.Timothy JY, Swong K, Park P. Complications of anterior cervical spine surgery: A systematic review of the literature. J Spine Surg 2020;6:302-22. [Google Scholar | PubMed]
- 12.Hitchon PW, Moritani T, Woodroffe RW, Abode-Iyamah K, Tecle NE, Noeller J, et al. C5 palsy following posterior decompression and instrumentation in cervical stenosis: Single center experience and review. Clin Neurol Neurosurg 2018;174:29-35. [Google Scholar | PubMed]
- 13.Jack A, Ramey WL, Dettori JR, Tymchak ZA, Oskouian RJ, Hart RA, et al. Factors associated with C5 palsy following cervical spine surgery: A systematic review. Global Spine J 2019;9:881-94. [Google Scholar | PubMed]
- 14.Fujibayashi S, Shikata J, Yoshitomi H, Tanaka C, Nakamura K, Nakamura T. Bilateral phrenic nerve palsy as a complication of anterior decompression and fusion for cervical ossification of the posterior longitudinal ligament. Spine (Phila Pa 1976) 2001;26:E281-6. [Google Scholar | PubMed]
- 15.Hendershot KA, O’Phelan KH. Respiratory complications and weaning considerations for patients with spinal cord injuries: A narrative review. J Pers Med 2022;13:97. [Google Scholar | PubMed]
- 16.Fuller DD, Rana S, Smuder AJ, Dale EA. The phrenic neuromuscular system. Handb Clin Neurol 2022;188:393-408. [Google Scholar | PubMed]
- 17.Moon AS, Pearson JM, Pittman JL. Phrenic nerve palsy after cervical laminectomy and fusion. N Am Spine Soc J 2020;4:100022. [Google Scholar | PubMed]
- 18.Di Serafino M, Dell’Aversano Orabona G, Caruso M, Camillo C, Viscardi D, Iacobellis F, et al. Point-of-care lung ultrasound in the intensive care unit-the dark side of radiology: Where do we stand? J Pers Med 2023;13:1541. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Radiologically Devastating Yet Neurologically Intact: A Rare Case of Ambulatory C6–C7 Translational Injury with Bilateral Facet Dislocation and Vertebral Artery Thrombosis
August 1, 2026 Radiologically Devastating Yet Neurologically Intact: A Rare Case of Ambulatory C6–C7 Translational Injury with Bilateral Facet Dislocation and Vertebral Artery Thrombosis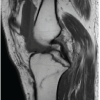 August 1, 2026 An Unusual Catastrophic Neurological Complication Following a Routine Arthroscopic Multiligament Knee Reconstruction: A Case Report
August 1, 2026 An Unusual Catastrophic Neurological Complication Following a Routine Arthroscopic Multiligament Knee Reconstruction: A Case Report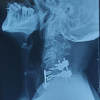 April 1, 2026 A Rare Case of C5–C6 Bilateral Facetal Dislocation with Central Cord Syndrome Managed by Staged Stabilization
April 1, 2026 A Rare Case of C5–C6 Bilateral Facetal Dislocation with Central Cord Syndrome Managed by Staged Stabilization April 1, 2026 Anterior Cervical Discectomy and Fusion with Polyetheretherketone Cage or Anterior Cervical Plate: A Comparative Evaluation of Short-term Outcomes
April 1, 2026 Anterior Cervical Discectomy and Fusion with Polyetheretherketone Cage or Anterior Cervical Plate: A Comparative Evaluation of Short-term Outcomes