
Knowledge of the Arthrex Labral Scorpion, with its smaller size and narrow, elongated tip, offers the surgeon greater variability when approaching anterior cruciate ligament repair, particularly in young children with a smaller notch width, making access to the femoral stump difficult for suture repair.
Dr. Bruce E Heck, Department of Orthopedic Surgery, University of Toledo Medical Center, Toledo, Ohio, USA/Northwest Ohio Orthopedics and Sports Medicine, Findlay, Ohio, USA. E-mail: drbruceheck@gmail.com
Abstract
Introduction: The arthrex labral scorpion suture passer, which is normally used in shoulder surgery for labral repair, is a useful tool to aid in anterior cruciate ligament (ACL) repair techniques. This technique greatly assists anatomic repair and stabilization, and allows the surgeon to complete the operation when there is limited repair instrumentation available, or the surgeon needs better access to the femoral stump. We present a case of the use of the shoulder arthrex labral scorpion used for knee ACL repair technique, which, to our knowledge, has not been reported, utilized for arthroscopic ACL mid-substance repair in a child.
Case Report: This case report presents a 12-year-old female with a mid-substance ACL tear following a valgus injury to the right knee following collision with an opponent’s leg while playing basketball. She was initially evaluated by the coaching staff and was discharged home, where she received ace wrap and crutches. The family requested follow-up with our practice several days later and requested seeing the senior author who performed ACL reconstruction on her biological mother and father. The family requested ACL repair to treat this mid-substance tear. Due to a narrow intercondylar width, an arthrex labral scorpion shoulder suture passer was essential for the ACL repair technique to access the limited recess of the femoral stump in the intercondylar notch and accomplish successful repair.
Conclusion: The arthrex labral scorpion suture passer for ACL repair techniques using the smaller and more narrow tip compared to the arthrex knee scorpion greatly increases the ability to successfully place suture in the proximal femoral stump secondary to differences in sizes of the femoral stump, different types of ACL tears, or in our case limited access secondary to a child with smaller bones and more narrow intercondylar distance.
Keywords: Anterior cruciate ligament, anterior cruciate ligament repair, arthrex labral scorpion, AR-13998QL, femoral stump, arthrex knee scorpion, AR-12990.
Mid-substance anterior cruciate ligament (ACL) tears in young patients are increasingly recognized due to greater sports participation and earlier specialization [1]. Recent literature supports timely surgical intervention using primary repair or reconstruction, though both approaches remain challenged by poor healing potential, technical complexity, and the risk of physeal injury [2,3,4]. In addition, a narrow intercondylar notch in skeletally immature patients further restricts arthroscopic access to the femoral ACL footprint and femoral stump in mid-substance tears, making conventional suture passage techniques more difficult [5,6]. A genetic predisposition to ACL tears has also been well documented, with first-degree relatives demonstrating more than double the risk of ligament injury [7,8]. The arthrex labral scorpion, an instrument normally used for shoulder labral repair, can facilitate ACL repair by enabling controlled suture placement and needle deployment within a narrow intercondylar notch, and allows the surgeon to get optimal tissue purchase in the femoral stump for repair and healing possibly reducing the risk of iatrogenic physeal injury associated with reconstruction. The literature supports the use of specialized low-profile suture passing instruments, including self-retrieving passers, knotless suture ring constructs, and modified needle-based devices, for facilitating ACL repair in pediatric patients with limited notch space [9,10,11,12]. However, no published reports detail the use of the arthrex labral scorpion for femoral stump suture passage during pediatric ACL repair, and its comparative effectiveness in this setting remains unestablished. This case report describes the use of the shoulder arthrex labral scorpion used for ACL repair in a 12-year-old female athlete who suffered a mid-substance ACL tear following a valgus collision injury to the right knee while playing basketball. Notably, both biological parents had previously sustained ACL tears that were reconstructed by the senior author, underscoring the familial predisposition described in the literature. The report highlights a novel adaptation of shoulder arthroscopy instrumentation to address limited notch access and easier access to the femoral stump during pediatric ACL repair.
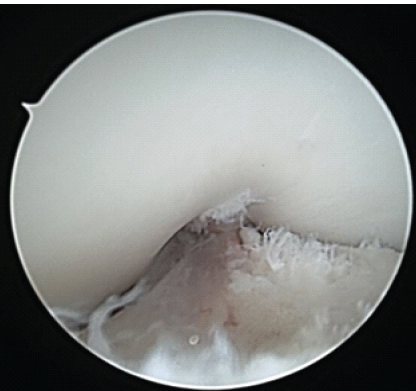
A 12-year-old and 1-month-old premenarchal female presented with a right knee injury after playing basketball when another player collided, striking the patient’s right knee on the outside. The patient sustained a valgus injury to her right knee and felt a pop, followed by pain described as 8 on a scale of 1–10. The patient could not continue playing sports. The pain was described as a dull aching pain, and the patient was unable to bear weight. Patient past medical history was significant for febrile seizures. Patient past surgical history is unremarkable. There were no known drug allergies. The patient did not take any medication. Family history was significant for previous ACL tears with reconstructions in both the mother and father by the senior author 20+ years ago. Physical examination revealed a young female, 60 inches tall and 126 pounds. Here blood pressure was 108/59 with a pulse rate of 90. Initially, the patient had an examination of the non-affected, left knee, which was noted to have no pain to palpation, full range of motion, and ligamentous stability to Lachman’s, posterior drawer, and collateral ligament testing. Next, the patient had an exam of the right knee, revealing knee effusion to visual inspection with tenderness at the lateral femoral condyle to palpation. The patient was guarding and lacked full extension. Lachman’s examination was positive. The patient had a limitation of flexion to 60° limited by pain. The posterior drawer and pivot shift tests were unable to be assessed secondary to pain. The collateral ligaments were stable, and the patient had no calf tenderness and was neurovascularly intact. Three-view radiographs of the right knee were obtained, which did not reveal evidence of fracture. The patient was placed in a knee immobilizer with crutches and was protected weight-bearing with crutches and no sports. Magnetic resonance imaging (MRI) of the right knee was completed 12 days after injury, revealing a complete ACL tear without associated fracture, bone bruise, meniscal tear, or other ligament injury noted. The patient underwent anterior tibial displacement measurement with the knee tester (KT) arthrometer, revealing 7 mm side-to-side difference between the non-involved, left leg (9 mm) and the involved leg, right leg (16 mm) at 30° of flexion. The patient and family had a review of MRI and KT results with very lengthy discussion regarding the risks and benefits of treatment options, including non-operative treatment, ACL repair, and the various types of ACL reconstruction. Due to patient’s young age, premenarchal status, and understanding of the demands required for ACL reconstruction since both parents had undergone ACL reconstruction themselves, the parents desired to proceed with ACL repair understanding that there were no guarantees on relief of pain or restoration of ligamentous healing and knee stability, and consent was obtained. Less than 4 weeks after the injury, the patient underwent ACL repair. The patient was seen in the pre-operative holding area, where she previously received a femoral nerve block. The patient had initials placed on her right knee. The patient was brought to the operating room (OR), where she underwent a general laryngeal mask airway. The patient was placed in a supine fashion on the operative table. The upper extremities and ulnar nerves were well-padded and protected. A tourniquet was applied to the right proximal thigh area. The patient was placed in a Stryker leg holder. No tourniquet was used. The left lower extremity was well-padded on a blanket and pillow. A time-out was performed with confirmation of antibiotics. We began by injecting respective anteromedial and anterolateral portal sites with 10 mL of 0.25% bupivacaine with epinephrine. The patient then had portals developed. The scope was inserted laterally. On entering, the patellofemoral joint appeared to be intact. The fat pad was debrided for visualization of the ACL midsubstance tear, with mop ends noted (Fig. 1).
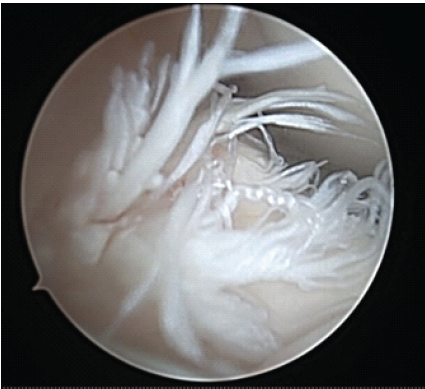
Figure 1: Intraoperative arthroscopic image from the anterolateral portal of the right knee with 30° arthroscope showing mid-substance anterior cruciate ligament rupture. Note torn mop ends of tibial stump.
The medial meniscus was stable to probing, and photographs taken. Next, the patient had attention directed toward the lateral meniscus. The lateral meniscus was unremarkable and stable to probing, with photographs taken. Next, an arthrex passport was placed in the anteromedial portal. The knee scorpion was used to pass arthrex fiberloop suture through the tibial stump. With traction on the suture in the tibial stump, there was improved access and visualization to the femoral stump. Attempts at passing suture through the femoral stump with the arthrex knee scorpion were unsuccessful as the instrument was too large to gain access to the proximal femoral stump with the constraints of the small intercondylar notch. The arthrex labral repair scorpion was utilized as it was smaller, had a larger depth of bite, and was able to gain access to the intercondylar notch for secure fixation onto the femoral stump (Figs. 2, 3, 4, 5).
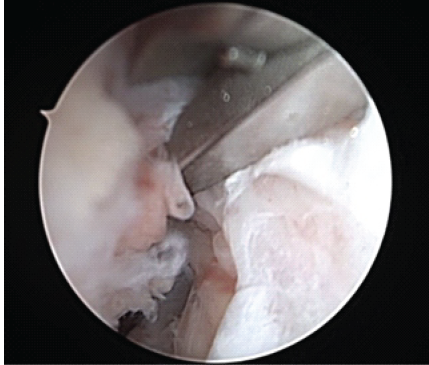
Figure 2: Intraoperative arthroscopic image of the right knee taken from the anterolateral viewing portal of Arthrex Labral Scorpion brought in from the anteromedial portal passing suture within the proximal femoral stump.
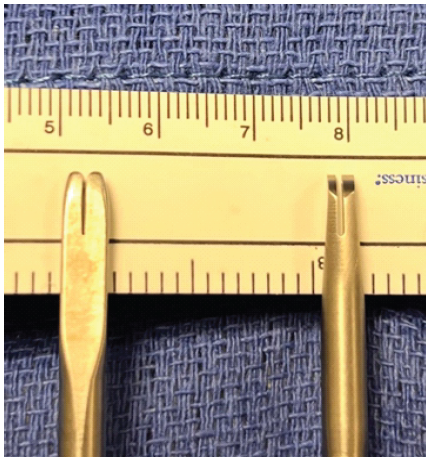
Figure 3: Photographic image taken comparing the Arthrex Labral Scorpion and the Arthrex Knee Scorpion undersurface views. Note how the Arthrex Labral Scorpion tip (right) is narrower, allowing for easier access in tight spaces.
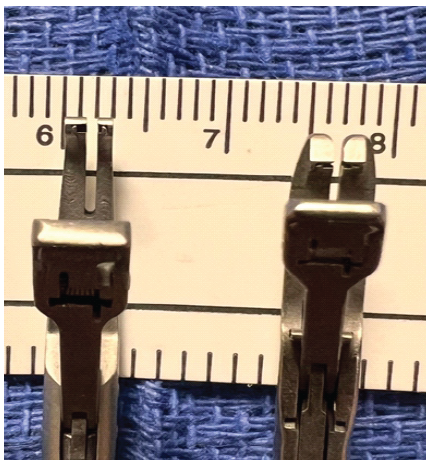
Figure 4: Photographic image taken comparing the Arthrex Labral Scorpion and the Arthrex Knee Scorpion top views. Note how the Arthrex Labral Scorpion tip (left) is narrower and elongated, allowing for easier access in tight spaces.
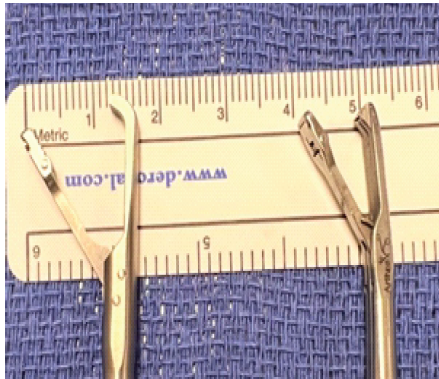
Figure 5: Photographic images taken comparing the Arthrex Labral Scorpion (left) and the Arthrex Knee Scorpion. Note how the Arthrex Labral Scorpion with an elongated and deeper bite allows for more precise placement of suture.
An arthrex fiberloop was placed. With secure fixation on the femoral and tibial stumps, the patient had ACL repair performed in extension and had sutures tied with secure fixation with the aid of a knot pusher. The knot was small and did not impinge in the notch. The patient had a stable ACL to probing and had an excellent endpoint to a gentle Lachman’s at 30° of knee flexion and no impingement along the lateral wall or notch in full extension. Multiple photographs were taken documenting and demonstrating the ACL repair (Figs. 6, 7, 8).

Figure 6: Arthroscopic image of right knee anterior cruciate ligament repair from anterolateral portal at 90° of flexion. Note the limited space for proximal femoral stump suture placement.
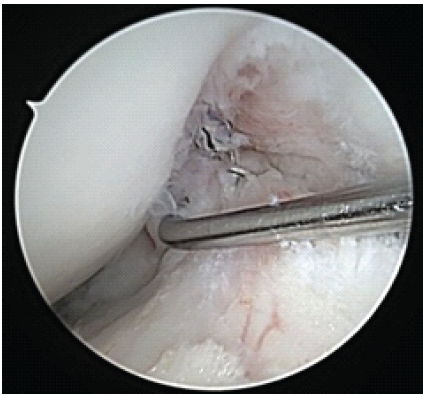
Figure 7: Arthroscopic image of right knee anterior cruciate ligament repair viewed from anterolateral portal at 30° flexion. Stable to probing.
Figures 8: Arthroscopic image of right knee anterior cruciate ligament repair in full extension, demonstrating no impingement.
The patient tolerated the procedure well. The instrumentation was removed. The arthrex passport was removed. Portal sites were closed with 3–0 nylon suture followed by sterile dressing, polar care, and knee immobilizer. The patient was transferred to the recovery room in stable condition with the toes pink, good capillary refill, and neurovascular intact.
Postoperatively, the patient was weight-bearing as tolerated with a knee immobilizer on. At 2 weeks postoperatively, the patient had nylon stitches removed and was healing uneventfully. The patient remained in physical therapy performing active assisted knee flexion in a chair with a sliding board, straight leg raise, bicycling, and neuromuscular reeducation with biphasic quad stim over the next 4 weeks. At 6 week follow-up, the patient had an excellent endpoint to gentle Lachman’s at 30° of knee flexion, full range of motion, and reported no pain or problems. The patient continued the hinged knee brace unlocked while at school for the next 6 weeks. At 3 months post-operative, the patient was advanced with strengthening exercise and fit with a custom-fit ACL brace at 4 months, which she wore at school. The patient was seen monthly for follow-up and had an uneventful recovery until 8 months while performing lunges, felt a pop and had pain localized to the tibial tubercle. Lachman’s exam was intact with a stable endpoint at 30°. Radiographs showed non-displaced tibial tubercle transverse fracture. The patient was immobilized for 4 weeks until the pain was resolved and the fracture healed. The patient resumed strengthening and finally, at 8 months post-operative passed strength testing with strength >80% of the opposite leg and passed functional progression testing. The patient had an excellent endpoint and resumed full activity, including resuming basketball without problems. Patient was last seen in the office 17 months after the repair and was doing well with her knee, with stable Lachman’s and no pivot shift, though unfortunately, due to overuse in summer basketball camps, practice, and basketball season developed stress fractures of the bilateral pedicles of L5 and the left pedicle of L4.
The arthrex labral scorpion is a straightforward, easy-to-use tool utilizing a narrower and more pointed tip (Fig. 4) to facilitate the surgeon’s ability to grasp, pierce, and pass suture for precise placement and anatomic repair during ACL repair (Fig. 2) when another suture passer, such as the arthrex knee scorpion, is of improper size or not available. This knowledge greatly assists the surgeon in anatomic repair and stabilization, and allows the surgeon to complete the operation when there is limited instrumentation, or the surgeon needs an instrument with a lower profile to gain access for soft-tissue repair in tight spaces as in our case. Perhaps, mid-substance ACL repair outcomes will be improved by the ability to get better fixation with suture purchase in the proximal stump. Although there have been many techniques described to accomplish ACL repair, there is consensus that the location of the tear, tissue quality, proper suture placement, and fixation techniques during repair of ACL tears are all important factors to achieve an optimal outcome with a lower incidence of retear [9,10,11,12]. Our patient’s family chose ACL repair after extensive discussion regarding the risks and benefits of various forms of treatment, both non-operative and operative, including ACL reconstruction. The patient and family requested to avoid the associated risk of knee pain and physeal injury associated with ACL reconstruction, which was a recommended procedure to them, due to the family history of both biological parents having undergone ACL reconstruction, and understanding the extensive post-operative therapy protocol and recovery. When evaluating ACL repair versus ACL reconstruction, evidence suggests that both ACL repair and ACL reconstruction are appropriate treatments, though ACL reconstruction shows lower rates of rerupture [4,9]. However, ACL repair may avoid physeal injury and knee pain and has the potential advantages of reduced surgical trauma, avoidance of autograft harvest complications, and maintaining native ACL tissue proprioceptive function [9,10]. One of the most feared and devastating complications of ACL reconstruction in the pediatric populations, which is felt to be underreported, is damage to the physis that can lead either to a growth arrest resulting in a limb length discrepancy or an angular deformity [1,2,3,4,9]. In retrospect, ACL repair was the ideal fixation method for this patient in view of premenstrual status with open growth plates to avoid physeal injury and the family’s desire to avoid a more major surgery and harvest site morbidity. Although ACL repair particularly for mid substance tears has shown higher retear rates compared to ACL reconstruction [4,9], in recent years, there have been many studies demonstrating that ACL repair is a safe and effective method of managing such injuries in the pediatric patient while avoiding some of the complications associated with conventional ACL reconstructive techniques [9,10,11,12]. Certainly, in our case, there was extensive planning and communication before surgery with the instrumentation representatives, OR director, and operating team to ensure all necessary equipment was available to accomplish ACL repair and fixation in a timely manner to minimize OR time and surgical risks. ACL repair has been shown to be beneficial for the treatment of ACL rupture in the pediatric population with reduced surgical morbidity [9,10,11,12]. Despite our planning, the intercondylar distance did not accommodate the thickness of the arthrex knee scorpion. Fortunately, being cross trained and having the knowledge of the arthrex labral scorpion provided an easy to administer solution to successfully place suture in the femoral stump to accommodate ACL repair and stabilization which can accommodate a variety of different ACL tear locations and shapes, difference in sizes of the femoral stump, or in our case limited space secondary to a child with smaller bones and narrower intercondylar distance.
Figure 2: Intraoperative arthroscopic image of the right knee taken from the anterolateral viewing portal of Arthrex Labral Scorpion brought in from the anteromedial portal passing suture within the proximal femoral stump.
Figure 3: Photographic image taken comparing the Arthrex Labral Scorpion and the Arthrex Knee Scorpion undersurface views. Note how the Arthrex Labral Scorpion tip (right) is narrower, allowing for easier access in tight spaces.
Figure 4: Photographic image taken comparing the Arthrex Labral Scorpion and the Arthrex Knee Scorpion top views. Note how the Arthrex Labral Scorpion tip (left) is narrower and elongated, allowing for easier access in tight spaces.
Figure 5: Photographic images taken comparing the Arthrex Labral Scorpion (left) and the Arthrex Knee Scorpion. Note how the Arthrex Labral Scorpion with an elongated and deeper bite allows for more precise placement of suture.
The arthrex labral scorpion, with its narrow tip and low profile has been developed for labral repair in the shoulder, but due to its versatility is useful for ACL repair in the pediatric knee (Fig. 2,3,4,5) and is a valuable tool for the surgeon to have in his arsenal. Furthermore, as there are increasing demands from hospitals to provide specialty care for patients at smaller hospitals and insurance providers dictating care to certain hospitals, there will be times when surgeons must operate at a facility that may not provide unlimited equipment, and the shoulder arthrex labral scorpion can double as a capable suture passer in pediatric knee ACL repair. On the contrary, a surgeon at a larger hospital may have limitless resources but may otherwise be unaware of the dual application of this tool to facilitate ACL repair.
This case report highlights the importance of informed consent during the surgical process and emphasizes the need to discuss the risk and benefits of various treatment options for ACL rupture in the pediatric patient with the patient and their legal guardians. The family of this 12-year-old patient did not want the greater risks of a larger operation of ACL reconstruction and elected for repair, understanding increased retear rates. The arthrex labral scorpion for ACL repair is a useful tool to facilitate ligamentous suture placement during repair.
The arthrex labral repair suture passer for ACL repair techniques is a straight forward, easy to use tool that should be kept in the surgeons’ arsenal as the device provides a smaller and more narrow, elongated footprint onto the ACL stump and into the intercondylar notch that significantly increases the ability to successfully place sutures in good tissue and stabilize multiple variations of different ACL tears whether secondary to differences in sizes of the remaining stumps, different sizes of bones and intercondylar distance, or limited ligamentous repair tools available.
References
- 1. Frank JS, Gambacorta PL. Anterior cruciate ligament injuries in the skeletally immature athlete: Diagnosis and management. J Am Acad Orthop Surg 2013;21:78-87. [Google Scholar] [PubMed]
- 2. Defrancesco CJ, Storey EP, Shea KG, Kocher MS, Ganley TJ. Challenges in the management of anterior cruciate ligament ruptures in skeletally immature patients. J Am Acad Orthop Surg 2018;26:e50-61. [Google Scholar] [PubMed]
- 3. Attri M, D’Ambrosi R, Farinelli L, Malik SS, De Sa D, Tapasi S, et al. ACL reconstruction in skeletally immature athletes: Current concepts. Medicina (kaunas) 2025;61:562. [Google Scholar] [PubMed]
- 4. Bales CP, Guettler JH, Moorman CT 3rd. Anterior cruciate ligament injuries in children with open physes: Evolving strategies of treatment. Am J Sports Med 2004;32:1978-85. [Google Scholar] [PubMed]
- 5. Lima FM, Debieux P, Aihara AY, Cardoso FN, Franciozi CE, Grimberg A, et al. The development of the intercondylar notch in the pediatric population. Knee 2020;27:747-54. [Google Scholar] [PubMed]
- 6. Lima FM, Debieux P, Astur DC, Luzo MV, Cohen M, Cardoso FN, et al. The development of the anterior cruciate ligament in the paediatric population. Knee Surg Sports Traumatol Arthrosc 2019;27:3354-63. [Google Scholar] [PubMed]
- 7. Hasani S, Feller JA, Webster KE. Familial predisposition to anterior cruciate ligament injury: A systematic review with meta-analysis. Sports Med 2022;52:2657-68. [Google Scholar] [PubMed]
- 8. Magnusson K, Turkiewicz A, Hughes V, Frobell R, Englund M. High genetic contribution to anterior cruciate ligament rupture: Heritability ∼69. Br J Sports Med 2021;55:385-9. [Google Scholar] [PubMed]
- 9. Tang C, Kwaees TA, Accadbled F, Turati M, Green DW, Nicolaou N. Surgical techniques in the management of pediatric anterior cruciate ligament tears: Current concepts. J Child Orthop 2023;17:12-21. [Google Scholar] [PubMed]
- 10. Jabara J, Trotter M, Confino JE, Zhang AL. Anterior cruciate ligament repair with suture tape augmentation using self-tapping knotless anchors. Arthrosc Tech 2025;14:103532. [Google Scholar] [PubMed]
- 11. Smeltzer K, Meyers A, Nelson R. All-epiphyseal anterior cruciate ligament repair using suture ring device in the skeletally immature patient. Arthrosc Tech 2023;12:e745-50. [Google Scholar] [PubMed]
- 12. Maliwankul K, Chuaychoosakoon C. Suturing the anterior cruciate ligament using a No. 16 intravenous catheter needle in avulsion anterior cruciate ligament injury. Arthrosc Tech 2020;9:e1191-6. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Functional Outcomes of Arthroscopic Anterior Cruciate Ligament Reconstruction Using Hamstring Tendon Autograft in a Predominantly Chronic Anterior Cruciate Ligament Injury Cohort: A Prospective Study
June 1, 2026 Functional Outcomes of Arthroscopic Anterior Cruciate Ligament Reconstruction Using Hamstring Tendon Autograft in a Predominantly Chronic Anterior Cruciate Ligament Injury Cohort: A Prospective Study June 1, 2026 Artelon Graft Augmentation in Revision Anterior Cruciate Ligament Reconstruction: Surgical Technique Guide
June 1, 2026 Artelon Graft Augmentation in Revision Anterior Cruciate Ligament Reconstruction: Surgical Technique Guide May 1, 2026 All-Inside Anterior Cruciate Ligament Reconstruction: A Minimally Invasive Bone Preserving Approach with Promising Functional Outcomes
May 1, 2026 All-Inside Anterior Cruciate Ligament Reconstruction: A Minimally Invasive Bone Preserving Approach with Promising Functional Outcomes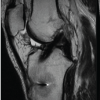 May 1, 2026 Anterior Cruciate Ligament Reconstruction Using Tibial Attachment – Preserving Hamstring Grafts: Early Clinical and Magnetic Resonance Imaging Assessment of Graft Ligamentization
May 1, 2026 Anterior Cruciate Ligament Reconstruction Using Tibial Attachment – Preserving Hamstring Grafts: Early Clinical and Magnetic Resonance Imaging Assessment of Graft Ligamentization