
Salmonella prosthetic joint infection should be suspected in immunocompromised patients with pain after arthroplasty, and staged revision with targeted antibiotics can provide successful infection control.
Dr. J K Giriraj Harshavardhan, Department of Orthopedic Surgery, Sri Ramachandra Institute of Higher Education and Research, Chennai, Tamil Nadu, India. E-mail: girirajh@yahoo.com
Abstract
Introduction: Prosthetic joint infection (PJI) following total hip arthroplasty is commonly caused by Gram-positive organisms, whereas Salmonella Typhimurium infection is rare and usually associated with immunocompromised states.
Case Reports: A 32-year-old male with long-term corticosteroid therapy for seronegative inflammatory arthritis underwent bilateral total hip arthroplasty and later presented with right hip pain and intermittent fever. Laboratory investigations revealed elevated inflammatory markers, and radiographs demonstrated prosthetic loosening. The patient underwent implant removal, extensive debridement, and insertion of an antibiotic-loaded cement spacer. Intraoperative cultures yielded Salmonella Typhimurium sensitive to ciprofloxacin. Following staged surgical management and culture-directed antibiotic therapy, the patient showed good clinical recovery with no evidence of persistent infection at follow-up.
Conclusion: Salmonella PJI is uncommon but should be considered in immunocompromised patients. Early diagnosis, staged revision surgery, and targeted antimicrobial therapy are essential for successful outcomes.
Keywords: Salmonella typhimurium, total hip arthroplasty, prosthetic joint infection, corticosteroids, cement spacer.
Prosthetic joint infection (PJI) represents a significant complication following total hip arthroplasty, with an incidence of approximately 1–2% [1]. The majority of cases are caused by Gram-positive organisms, particularly Staphylococcus species, while Gram-negative organisms contribute to a smaller proportion [2]. Among Gram-negative pathogens, Salmonella species are rarely implicated in PJIs [3]. Although typically associated with gastrointestinal illness, these organisms can occasionally spread hematogenously and involve prosthetic joints, especially in immunocompromised individuals [4-7]. Risk factors include diabetes mellitus, malignancy, and prolonged corticosteroid therapy [3]. We present a rare case of Salmonella Typhimurium infection in a young patient with bilateral total hip arthroplasty and chronic corticosteroid exposure.
A 32-year-old male had a long-standing history of seronegative inflammatory arthritis and had been on prolonged unsupervised corticosteroid therapy for 20 years. He underwent left total hip arthroplasty in February 2024 and right total hip arthroplasty in July 2025 for stage IV avascular necrosis of the femoral head with secondary arthritis. He presented with pain in the right hip for 3 months (since November 2025), associated with difficulty in weight-bearing and intermittent fever for 1 week. The pain was gradual in onset, progressively worsening, dull aching in nature, and non-radiating. There was no history of trauma or constitutional symptoms. On examination, a healed surgical scar was noted over the right hip with painful restriction of movements. No sinus or active discharge was noted. Laboratory investigations showed elevated inflammatory markers (erythrocyte sedimentation rate: 140 mm/h; C-reactive protein: 9.4 mg/dL). Blood and urine cultures showed no growth of organisms. Radiographs demonstrated features suggestive of prosthetic loosening, raising suspicion of infection (Figs. 1 and 2).
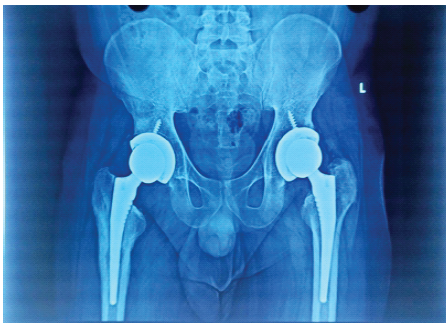
Figure 1: Anteroposterior radiograph of pelvis with both hips at presentation showing periprosthetic radiolucency and osteolysis suggestive of prosthetic loosening secondary to infection.
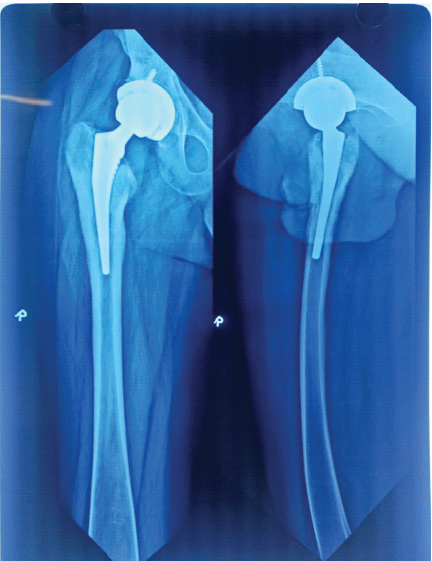
Figure 2: Anteroposterior and lateral radiograph of the right femur showing evidence of bone resorption, cortical irregularity, and periosteal reaction in the proximal femur suggestive of infection.
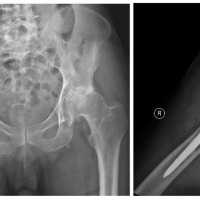
In the present case, computed tomography demonstrated peri-implant osteolysis with focal cortical breach, surrounding sclerosis, and periosteal reaction around the prosthesis, suggestive of chronic infective loosening (Fig. 3).

Figure 3: Computed tomography image showing peri-implant osteolysis and focal zone of cortical breach with dense sclerosis and periosteal reaction surrounding the implant.
These findings helped delineate the extent of peri-prosthetic bone involvement and assisted in planning staged revision surgery. A diagnosis of PJI was made, and the patient was planned for two-stage revision surgery. Pre-operative antibiotics were not administered. Intraoperatively, purulent material was identified around the prosthesis. The prosthetic components were removed. The femoral head was easily removed with an extractor, but the well-fixed acetabular component was carefully removed using acetabular osteotomes. Extensive debridement was performed. Multiple tissue samples were collected for microbiological and histopathological evaluation, and an antibiotic-loaded cement spacer (Tecres) was inserted (Fig. 4).
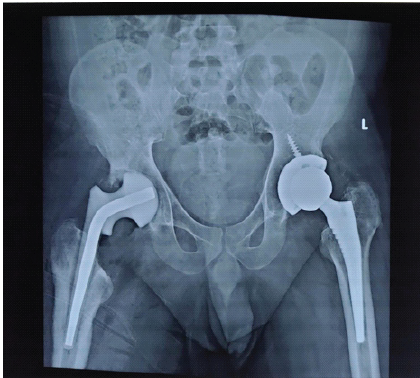
Figure 4: Immediate post-operative radiograph showing stage 1 revision arthroplasty.
Microbiological analysis revealed Salmonella Typhimurium, which was sensitive to ciprofloxacin. Based on susceptibility, intravenous ciprofloxacin 200 mg twice daily was initiated. Histopathological examination showed chronic inflammatory changes with granulation tissue. After 2 weeks of therapy, the patient demonstrated significant clinical improvement with a healthy surgical wound. Intravenous ciprofloxacin was given for 4 weeks, followed by 4 weeks of oral ciprofloxacin. At the 8-week follow-up, the wound had completely healed, inflammatory markers had normalised, and the patient remained pain-free with no evidence of persistent infection. The patient continues to be under follow-up and is planned for second-stage revision arthroplasty.
PJI caused by Salmonella species is rare, with only a limited number of cases described in the literature [4]. These infections are more frequently observed in patients with compromised immune function [3]. The present case is noteworthy due to the relatively young age of the patient and the presence of prolonged corticosteroid therapy as a major predisposing factor. Corticosteroids impair cell-mediated immunity, thereby increasing susceptibility to opportunistic infections such as Salmonella [3]. The pathogenesis is most likely haematogenous dissemination, even in the absence of overt gastrointestinal symptoms, which has been documented in previous studies [7]. Due to the rarity of such infections, management protocols are not well standardised. However, staged surgical management involving prosthetic component removal, extensive debridement, and antibiotic spacer placement is widely accepted as the preferred approach in chronic infections [5, 8-10]. Previous reports of Salmonella infection following joint arthroplasty have also demonstrated favourable outcomes with surgical intervention combined with targeted antimicrobial therapy [9,10]. Appropriate antimicrobial therapy is essential, with fluoroquinolones and third-generation cephalosporins commonly employed due to their intracellular activity against Salmonella species [6]. Early recognition and prompt intervention are critical to achieving infection control and satisfactory functional outcomes. The present report has certain limitations inherent to a single-case study. Due to the rarity of Salmonella Typhimurium PJI, comparison with larger cohorts and establishment of standardised treatment protocols remain difficult. The patient had multiple confounding factors, including prolonged corticosteroid therapy and inflammatory arthritis, which may have influenced both susceptibility to infection and clinical outcome. Blood and urine cultures were negative, and the exact source of infection could not be definitively established. Advanced molecular diagnostic methods, serum procalcitonin levels, and functional outcome scores were not evaluated. In addition, the follow-up period was relatively short, and the patient had not yet undergone second-stage revision arthroplasty at the time of reporting. Further studies with larger series and longer follow-up are required to better understand optimal management strategies and long-term outcomes of Salmonella PJIs.
Salmonella Typhimurium PJ Following total hip arthroplasty is rare but should be considered in immunocompromised individuals receiving long-term corticosteroid therapy. Early-stage surgical intervention combined with culture-directed antibiotic therapy is essential for successful management. Long-term follow-up is necessary to evaluate reinfection rates and functional outcomes following staged revision arthroplasty.
In immunocompromised patients with prosthetic joints, rare pathogens such as Salmonella should be considered, and timely staged intervention is a key to successful treatment.
References
- 1. Kurtz SM, Lau E, Watson H, Schmier JK, Parvizi J. Economic burden of periprosthetic joint infection in the United States. J Arthroplasty 2012;27:61-5.e1. [Google Scholar] [PubMed]
- 2. Sebastian S, Dhawan B, Malhotra R, Gautam D, Kapil A. Salmonella typhimurium infection in total knee arthroplasty: A case report with review of literature. J Lab Physicians 2017;9:217-9. [Google Scholar] [PubMed]
- 3. Tande AJ, Patel R. Prosthetic joint infection. Clin Microbiol Rev 2014;27:302-45. [Google Scholar] [PubMed]
- 4. Gupta A, Berbari EF, Osmon DR, Virk A. Prosthetic joint infection due to Salmonella species: A case series. BMC Infect Dis 2014;14:633. [Google Scholar] [PubMed]
- 5. Jeroense KT, Kuiper JW, Colen S, Schade RP, Saouti R. One-stage revision in two cases of Salmonella prosthetic hip infection. World J Clin Cases 2014;2:304-8. [Google Scholar] [PubMed]
- 6. Threlfall EJ. Antimicrobial drug resistance in Salmonella: Problems and perspectives in food- and water-borne infections. FEMS Microbiol Rev 2002;26:141-8. [Google Scholar] [PubMed]
- 7. Ortiz-Neu C, Marr JS, Cherubin CE, Neu HC. Bone and joint infections due to Salmonella. J Infect Dis 1978;138:820-8. [Google Scholar] [PubMed]
- 8. Samra Y, Shaked Y, Maier MK. Nontyphoid salmonellosis in patients with total hip replacement: Report of four cases and review of the literature. Rev Infect Dis 1986;8:978-83. [Google Scholar] [PubMed]
- 9. Musante DB, Ogden WS. Salmonella infection in joint arthroplasty. Orthopedics 2004;27:770-2. [Google Scholar] [PubMed]
- 10. Oe K, Wada T, Ohno H, Kushida T, Iida H. Salmonella septic arthritis following total knee arthroplasty for rheumatoid arthritis in a patient receiving etanercept. J Orthop Sci 2011;16:258-62. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 October 10, 2023 Two-stage Partial Component Retention and Interim Cemented Liner for Infected Total Hip Arthroplasty: A Case Report
October 10, 2023 Two-stage Partial Component Retention and Interim Cemented Liner for Infected Total Hip Arthroplasty: A Case Report August 1, 2026 Total Hip Arthroplasty without Subtrochanteric Shortening Osteotomy in a Neglected Posterior Hip Dislocation: A Case Report
August 1, 2026 Total Hip Arthroplasty without Subtrochanteric Shortening Osteotomy in a Neglected Posterior Hip Dislocation: A Case Report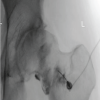 August 1, 2026 Case Report of Rapidly Destructive Osteoarthritis of the Hip following Multiple High-dose Intra-articular Steroid Injections
August 1, 2026 Case Report of Rapidly Destructive Osteoarthritis of the Hip following Multiple High-dose Intra-articular Steroid Injections August 1, 2026 Total Hip Arthroplasty in Bilateral Ankylosed Hip by Direct Anterior Approach: A Case Report with Technical Tips
August 1, 2026 Total Hip Arthroplasty in Bilateral Ankylosed Hip by Direct Anterior Approach: A Case Report with Technical Tips