
One-stage revision arthroplasty is an effective treatment option for selected patients with low-grade periprosthetic knee infection caused by low-virulence organisms, providing reliable infection control with reduced morbidity.
Dr. Georgios Renieris, Athens Medical Group, Psychiko Clinic, Andersen 1, 11525, Athens, Greece. E-mail: renierisg@yahoo.com
Abstract
Background: Low-grade periprosthetic joint infections (PJIs) are diagnostically challenging and often present with subtle clinical and laboratory findings. The optimal surgical strategy – one-stage or two-stage revision – remains controversial.
Case Report: We report a 74-year-old male with a low-grade PJI due to Staphylococcus hominis 6 months after cruciate-retaining total knee arthroplasty. Despite normal inflammatory markers, negative aspirate culture, and inconclusive imaging, tissue cultures confirmed infection. The patient underwent a one-stage revision with a favorable outcome. The immediate post-operative management was complicated by deep venous thrombosis and pulmonary embolism, prompting consideration of the risks inherent in revision surgery.
Conclusion: One-stage revision may be a viable option for selected patients with low-grade PJI, offering comparable infection control, improved functional outcomes, and fewer complications compared with two-stage revision.
Keywords: Periprosthetic joint infection, total knee arthroplasty, one-stage revision, Staphylococcus hominis, Low-grade infection.
Periprosthetic joint infection (PJI) is a serious and feared complication following total knee arthroplasty (TKA), with an incidence of 1–2% in primary procedures and higher rates in revision cases [1,2]. PJI is associated with significant morbidity, increased healthcare costs, and a substantial impact on patient quality of life [3]. While acute PJI often presents with overt signs of infection, low-grade PJI is frequently insidious, manifesting as persistent pain, mild swelling, or subtle joint dysfunction without systemic symptoms [4]. Low-grade infections are commonly caused by low-virulence organisms such as coagulase-negative staphylococci, including Staphylococcus hominis, which are capable of forming biofilms on prosthetic surfaces and thereby evading host immune responses and antibiotic therapy [5,6]. Diagnosis is challenging because inflammatory markers, imaging studies, and joint aspiration cultures may be normal or inconclusive [4,6]. Although the Musculoskeletal Infection Society (MSIS) and International Consensus Meeting (ICM) criteria provide structured diagnostic frameworks, their sensitivity is limited in low-grade infections [3,7]. Management of PJI requires a multidisciplinary approach. Surgical options include debridement with implant retention, one-stage revision, and two-stage revision. While two-stage revision has traditionally been considered the gold standard, recent evidence suggests that one-stage revision may provide comparable infection eradication with improved functional outcomes and reduced morbidity in selected patients with low-grade PJI [1,8,9,10]. This case report underscores potential diagnostic and therapeutic pitfalls in low-grade PJI and examines the available evidence to delineate situations in which one-stage revision may confer a significant advantage over two-stage revision.
A 74-year-old male with a history of epilepsy and hypertension underwent 20 years ago a right quadriceps tendon rupture repair. Due to posttraumatic arthritis of the right knee, the patient underwent cruciate-retaining TKA. Pre-operative evaluation showed no evidence of infection or immunosuppression. The post-operative course was initially uneventful. Six months after surgery, the patient developed gradually increasing peripatellar and lateral knee pain, worse at night, associated with mild swelling and warmth. He denied fever or systemic symptoms. Examination revealed a well-healed surgical scar, mild effusion, and lateral joint line tenderness without erythema or sinus tract. Good range of motion and retained stability of the right knee (Fig. 1).
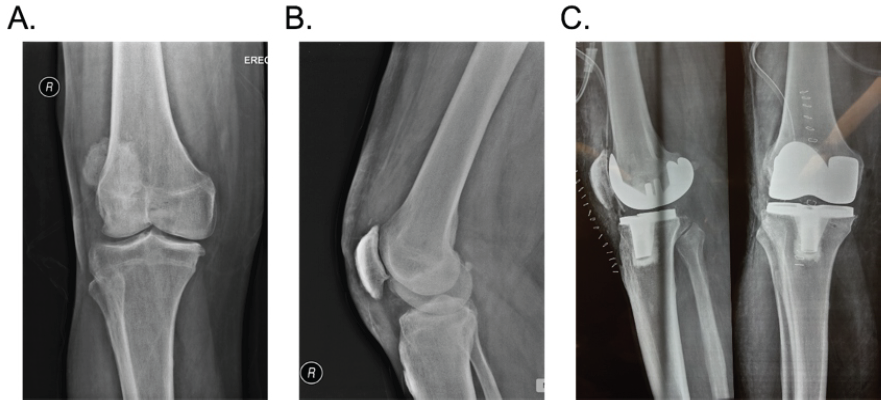
Figure 1: (a and b) Pre-operative anteroposterior and lateral radiograph of the right knee of a 74-year-old male patient with severe osteoarthritis of the right knee. (c) Post-operative anteroposterior and lateral radiograph of the right knee depicting a correct component and leg alignment after primary total knee replacement with a cruciate retaining knee system.
Laboratory investigations, including white blood cell count, C-reactive protein, and erythrocyte sedimentation rate, were within normal limits. Plain radiographs, a computed tomography (CT), and magnetic resonance imaging (MRI) showed a well-aligned prosthesis without loosening. An MRI showed a slight fluid accumulation under the tibial component, yet without signs of bone oedema or excessive knee effusion. A bone scan showed accumulation of radiopharmaceutical in the lateral femoral condyle, the patella, and the tibial plateau (Fig. 2).
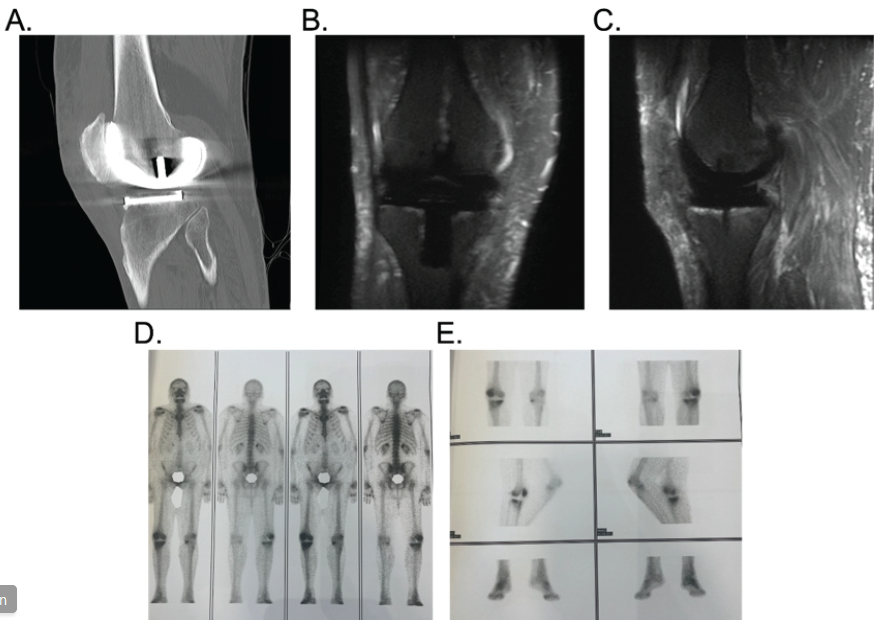
Figure 2: Evaluation of right total knee replacement in a 74-year-old patient with continuing symptoms 6 months after surgery. (a) Sagittal view of computed tomography showing no signs of loosening, component wear, or bone defects. (b and c) Coronal and sagittal views of magnetic resonance tomography showing slight fluid accumulation under the tibial component, without signs of bone edema or knee effusion. (d and e) Tc99 bone scan showing high uptake of radiopharmaceutical in the lateral femoral condyle, the patella, and the tibial plateau.
Knee aspiration yielded clear, bloody synovial fluid with elevated lymphocytes and lactate dehydrogenase; cultures were negative. Advanced imaging was inconclusive. Diagnostic arthroscopy was performed, and five tissue samples were obtained. Intraoperatively, no signs of knee effusion, excessive synovitis or tibial tray loosening. An intraoperative alpha-defensin test (Synovasure, Fa. Zimmer Biomet, Warsaw, IN, USA) was negative. Three cultures grew S. hominis. Histopathology demonstrated mild chronic inflammation. Given the identification of a low-virulence organism, absence of sinus tract or systemic signs of infection, and good soft tissue condition, a one-stage revision was selected after multidisciplinary discussion. The one-stage revision was performed under general anaesthesia without a tourniquet. Despite radiographic findings suggestive of possible component loosening, no loosening was identified intraoperatively. Similarly, no signs of polyethylene wear. The prosthesis was explanted, extensive debridement and jet lavage performed, and a semi-constrained prosthesis with patellar resurfacing implanted (Fig. 3).
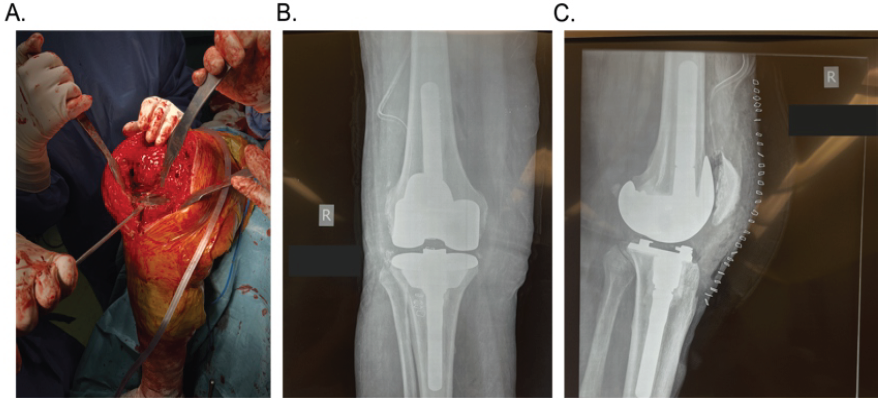
Figure 3: (a) Intraoperative image of the right knee of a 74-year-old male patient during revision surgery, after explantation of the femoral component. Despite radiographic findings suggestive of possible component loosening, no loosening was identified intraoperatively. (b and c) Postoperative anteroposterior and lateral radiograph of the right knee depicting a correct component and leg alignment after one-stage revision of the right knee with implantation of a semi-constrained knee system.
Postoperatively, targeted antibiotic therapy was administered. The patient received 4 weeks of intravenous vancomycin, followed by 4 weeks of oral daptomycin. The immediate postoperative period was complicated due to a right deep venous thrombosis and a subsequent minor lung embolism. This was treated according to standards with low-molecular-weight heparin. At 12-month follow-up, the patient was pain-free, laboratory markers remained normal, and no recurrence of infection was observed. The respective imaging showed a good implant positioning.
This case illustrates the diagnostic and therapeutic challenges of low-grade PJI following TKA. The subtle clinical presentation, normal inflammatory markers, negative aspiration cultures, and inconclusive imaging observed in this patient are typical of infections caused by low-virulence, biofilm-forming organisms such as S. hominis [5,6]. Diagnosis of low-grade PJI requires a high index of suspicion. Although the MSIS and ICM criteria have improved diagnostic standardisation, their sensitivity is reduced in low-grade infections, where biofilm-associated bacteria may evade detection [3,7]. In such cases, multiple intraoperative tissue cultures and histopathological analysis remain essential diagnostic tools. Arthroscopic biopsy, as performed in this case, can be particularly useful when non-invasive investigations are inconclusive. Despite radiographic findings suggestive of possible component loosening, intraoperative assessment may fail to confirm true mechanical instability. Several studies have demonstrated that conventional plain radiographs have limited sensitivity for detecting prosthetic loosening when compared with intraoperative findings, despite relatively high specificity when overt loosening is present [11]. In total hip arthroplasty, radiographic sensitivity for component loosening has been reported to be as low as 20–30%, indicating that radiolucent lines or subtle imaging changes may represent fibrous fixation or adaptive bone remodelling rather than true loosening [11,12]. Conversely, so-called “radiographically silent” loosening has also been described, with components found to be loose at revision surgery despite the absence of definitive preoperative imaging signs [13]. Advanced imaging modalities such as CT, MRI, or single-photon emission CT/CT may improve diagnostic accuracy in equivocal cases, but they too demonstrate variable sensitivity when validated against intraoperative findings [10,14]. These data highlight the importance of correlating radiographic findings with clinical presentation and intraoperative assessment, which remains the gold standard for confirming component stability. The optimal surgical strategy for low-grade PJI remains debated. Two-stage revision has historically been regarded as the gold standard, particularly for chronic or complex infections, due to high reported eradication rates [15,16]. However, two-stage revision is associated with prolonged treatment duration, increased morbidity, spacer-related complications, and often inferior functional outcomes, especially in elderly or comorbid patients [17,18]. Especially in the context of the present case, the development of venous thromboembolism following first-stage explantation within a two-stage revision strategy may substantially delay, or even preclude, second-stage reimplantation. Moreover, prolonged non-ambulatory status in the presence of active venous thromboembolism carries potentially disastrous consequences. Recent systematic reviews and meta-analyses have challenged the superiority of two-stage revision in low-grade infections. Zhao et al. analysed over 8,700 patients and found no significant difference in reinfection or reoperation rates between one-stage and two-stage revision for PJI [1]. Ghosh et al. reported infection clearance rates of 96% for one-stage and 92% for two-stage revision, with similar mortality and failure rates [8]. Sun et al. demonstrated pooled reinfection rates of 10.02% for one-stage and 14.75% for two-stage revision, with significantly fewer complications following one-stage revision [9]. Earlier meta-analyses by Kunutsor et al. found comparable reinfection rates between one- and two-stage revision in both hip and knee PJI [2,10]. Masters et al. and Beswick et al. also reported similar eradication rates and emphasised the importance of patient selection [4,15]. Registry data from Lenguerrand et al. further support individualised decision-making, showing that both strategies can be effective when appropriately applied [16]. Recent cohort studies reinforce these findings. Hansen et al. and Winkler et al. demonstrated high infection control rates and favourable functional outcomes with one-stage revision, particularly in patients with known, low-virulence organisms and good soft tissue conditions [19,20]. Jacobs et al. reported no difference in reinfection or functional outcomes between one-stage and two-stage revision but observed a trend toward higher adverse event rates in the two-stage group [21]. Pradhan et al. highlighted success rates ranging from 73% to 100% for single-stage revision and emphasised strict selection criteria as a key determinant of outcome [22]. Conversely, Mercurio et al. reported that although two-stage revision achieves high eradication rates, it is associated with significant morbidity, longer treatment duration, and functional limitations [17]. Kennedy et al. reported high failure and amputation rates following repeat two-stage revision for chronic knee PJI, underscoring the need for careful consideration of alternative strategies [18]. Current consensus guidelines recommend individualised treatment planning based on organism virulence, host factors, and local tissue conditions, supported by multidisciplinary collaboration [3,6]. Our case supports the growing evidence that one-stage revision is a safe and effective option in selected patients with low-grade PJI.
Low-grade periprosthetic infection following TKA may present with subtle clinical and laboratory findings, making diagnosis challenging. One-stage revision can be a viable and effective treatment option in carefully selected patients with low-virulence organisms, emphasising the importance of individualised management and multidisciplinary care.
One-stage revision arthroplasty is an effective treatment option for selected patients with low-grade periprosthetic knee infection caused by low-virulence organisms, providing reliable infection control with reduced morbidity.
References
- 1. Zhao Y, Fan S, Wang Z, Yan X, Luo H. Systematic review and meta-analysis of single-stage vs two-stage revision for periprosthetic joint infection: A call for a prospective randomized trial. BMC Musculoskelet Disord 2024;25:153. [Google Scholar] [PubMed]
- 2. Kunutsor SK, Whitehouse MR, Lenguerrand E, Blom AW, Beswick AD, Inform Team. Re-infection outcomes following one- and two-stage surgical revision of infected knee prosthesis: A systematic review and meta-analysis. PLoS One 2016;11:e0151537. [Google Scholar] [PubMed]
- 3. Parvizi J, Gehrke T, Chen AF. Proceedings of the international consensus on periprosthetic joint infection. Bone Joint J 2013;95-B:1450-2. [Google Scholar] [PubMed]
- 4. Masters JP, Smith NA, Foguet P, Reed M, Parsons H, Sprowson AP. A systematic review of the evidence for single stage and two stage revision of infected knee replacement. BMC Musculoskelet Disord 2013;14:222. [Google Scholar] [PubMed]
- 5. Li C, Renz N, Trampuz A. Management of periprosthetic joint infection. Hip Pelvis 2018;30:138-46. [Google Scholar] [PubMed]
- 6. Trampuz A, Zimmerli W. Diagnosis and treatment of implant-associated septic arthritis and osteomyelitis. Curr Infect Dis Rep 2008;10:394-403. [Google Scholar] [PubMed]
- 7. Gehrke T, Alijanipour P, Parvizi J. The management of an infected total knee arthroplasty. Bone Joint J 2015;97-B Suppl A:20-9. [Google Scholar] [PubMed]
- 8. Ghosh A, Madanipour S, Stammers J, Mitchell P, Alazzawi S. Long-term outcomes of single-stage versus two-stage revision for prosthetic joint infection: a retrospective, observational cohort study. Orthop Rev (Pavia) 2025;17:147165. [Google Scholar] [PubMed]
- 9. Sun Y, Liu M, Xiao D, Li Q, Xiong H, Luo X, et al. Prognosis after one- and two-stage revision surgery for periprosthetic joint infection: A systematic review and meta-analysis. J Orthop Surg (Hong Kong) 2025;33:10225536251315973. [Google Scholar] [PubMed]
- 10. Kunutsor SK, Whitehouse MR, Blom AW, Beswick AD, Inform Team. Re-infection outcomes following one- and two-stage surgical revision of infected hip prosthesis: A systematic review and meta-analysis. PLoS One 2015;10:e0139166. [Google Scholar] [PubMed]
- 11. Temmerman OP, Raijmakers PG, Berkhof J, Hoekstra OS, Teule GJ, Heyligers IC. Accuracy of diagnostic imaging techniques in the diagnosis of aseptic loosening of the femoral component of a hip prosthesis: a meta-analysis. J Bone Joint Surg Br 2005;87:781-5. [Google Scholar] [PubMed]
- 12. Mulcahy H, Chew FS. Current concepts in imaging of total joint arthroplasty. AJR Am J Roentgenol 2014;203:W237-48. [Google Scholar] [PubMed]
- 13. Reininga IH, Wagenmakers R, Van Den Akker-Scheek I, Van Der Wal B, Zijlstra W, Stevens M. Radiographically silent loosening of the acetabular component in total hip arthroplasty. Clin Orthop Relat Res 2012;470:2747-54. [Google Scholar] [PubMed]
- 14. Hirschmann MT, Iranpour F, Konala P, Kerner A, Rasch H, Friederich NF. Clinical value of SPECT/CT for evaluation of patients with painful knee arthroplasty: A new dimension of diagnostics? Knee Surg Sports Traumatol Arthrosc 2011;19:939-46. [Google Scholar] [PubMed]
- 15. Beswick AD, Elvers KT, Smith AJ, Gooberman-Hill R, Lovering A, Blom AW. What is the evidence base to guide surgical treatment of infected hip prostheses? systematic review of longitudinal studies in unselected patients. BMC Med 2012;10:18. [Google Scholar] [PubMed]
- 16. Lenguerrand E, Whitehouse MR, Beswick AD, Jones SA, Porter ML, Blom AW. Revision for prosthetic joint infection following hip arthroplasty: Evidence from the national joint registry. Bone Joint Res 2017;6:391-8. [Google Scholar] [PubMed]
- 17. Mercurio M, Cofano E, Colace S, Piro F, Cerciello S, Galasso O, et al. Outcomes of two-stage revision surgery. Prosthesis 2024;6:1240-58. [Google Scholar] [PubMed]
- 18. Kennedy IW, Howard LC, Somerville L. High failure rates following repeat two-stage revision. J Arthroplasty 2026;36:101906. [Google Scholar] [PubMed]
- 19. Hansen E, Tetreault M, Zmistowski B. One-stage exchange for prosthetic joint infection. Clin Orthop Relat Res 2013;471:3215-22. [Google Scholar] [PubMed]
- 20. Winkler H, Trampuz A, Hardt S. One-stage revision of infected hip and knee prostheses. Clin Microbiol Infect 2018;24:1212-7. [Google Scholar] [PubMed]
- 21. Jacobs MM, Heesterbeek PJ, Veerman K, Goosen JH. One- versus two-stage septic hip and knee revision surgery: A comparative cohort outcome study with short- to mid-term follow-up. J Bone Joint Infect 2025;10:185-92. [Google Scholar] [PubMed]
- 22. Pradhan TN, Viswanathan VK, Badgery R, Pradhan N. Single-stage revision in the management of prosthetic joint infections after total knee arthroplasty – a review of current concepts. J Clin Orthop Trauma 2024;52:102431. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Antiphospholipid Syndrome–Associated Livedoid Vasculopathy Mimicking Recurrent Periprosthetic Joint Infection after Total Knee Arthroplasty: A Case Report
June 1, 2026 Antiphospholipid Syndrome–Associated Livedoid Vasculopathy Mimicking Recurrent Periprosthetic Joint Infection after Total Knee Arthroplasty: A Case Report January 1, 2026 A Step Beyond Convention: Three-Stage Revision with Limb Reconstruction System Fixator for Chronic Infected Total Knee Arthroplasty – A Case Report
January 1, 2026 A Step Beyond Convention: Three-Stage Revision with Limb Reconstruction System Fixator for Chronic Infected Total Knee Arthroplasty – A Case Report September 1, 2024 Case Reports: Periprosthetic Joint Infection after Total Joint Arthroplasty Following Swimming Activity
September 1, 2024 Case Reports: Periprosthetic Joint Infection after Total Joint Arthroplasty Following Swimming Activity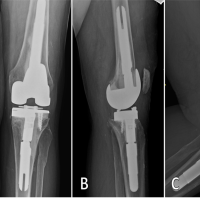 November 10, 2022 Lactococcus garvieae Periprosthetic Joint Infection in a Cattle Rancher with a Total Knee Arthroplasty: A Novel Reservoir Transmission
November 10, 2022 Lactococcus garvieae Periprosthetic Joint Infection in a Cattle Rancher with a Total Knee Arthroplasty: A Novel Reservoir Transmission