
Creatine supplementation is a biologically plausible, low-risk adjunct that may enhance post-operative muscle preservation and functional recovery after pediatric knee arthroscopy, warranting targeted clinical investigation.
Mr. Isaiah D Hoffman, Charles R. Drew University of Medicine and Science, Los Angeles, California. E-mail: isaiahhoffman@cdrewu.edu
Abstract
Introduction: Knee arthroscopy is a commonly performed minimally invasive orthopedic procedure in pediatric and adolescent populations, particularly for sports-related injuries such as ligament tears and meniscal pathology. Optimization of post-operative recovery is essential in this age group to preserve muscle mass, restore neuromuscular control, and facilitate safe return to activity during a critical period of musculoskeletal development. Perioperative nutritional strategies represent a modifiable adjunct to rehabilitation; however, their role in pediatric orthopedic recovery remains insufficiently defined.
Materials and Methods: This comprehensive narrative review synthesizes mechanistic, translational, and clinical literature on creatine supplementation to evaluate its potential role in enhancing post-operative recovery following pediatric and adolescent knee arthroscopy. Relevant literature was identified through structured searches of PubMed, Scopus, and Google Scholar, emphasizing adult orthopedic rehabilitation trials, experimental studies of skeletal muscle metabolism, perioperative nutrition research, and limited pediatric supplementation data. Although not conducted as a formal systematic review, a structured and targeted search strategy was used to enhance methodological rigor and reproducibility.
Results: Across adult surgical and immobilization models, creatine supplementation has demonstrated preservation of muscle mass, enhanced strength recovery, improved GLUT4-mediated glucose uptake, augmented glycogen storage, reduced inflammatory signaling, and attenuation of disuse-related muscle atrophy. Although direct pediatric surgical data are lacking, consistent mechanistic and clinical findings, combined with creatine’s endogenous production and favorable safety profile in youth athletic populations, provide a biologically plausible rationale for investigation in pediatric orthopedic settings.
Conclusion: The convergence of adult evidence and the absence of pediatric-specific clinical trials highlights a critical gap in the literature. Creatine supplementation represents a promising adjunct to post-operative rehabilitation following pediatric knee arthroscopy, warranting prospective clinical trials to determine its efficacy, safety, and optimal perioperative use.
Keywords: Creatine supplementation, pediatric orthopedics, knee arthroscopy, rehabilitation, muscle recovery, sports medicine.
Knee arthroscopy is a cornerstone of contemporary orthopedic care and is frequently performed in pediatric and adolescent patients for conditions such as meniscal injury, chondral pathology, ligamentous instability, and sports-related trauma [1]. Although minimally invasive, knee arthroscopy is often followed by transient muscle inhibition, strength loss, and functional deficits that may delay rehabilitation and return to sport [2]. In younger patients, these post-operative challenges occur during periods of active musculoskeletal growth and neuromuscular development, amplifying the importance of optimized recovery strategies.
Perioperative nutrition has emerged as an important modifiable factor influencing post-operative outcomes following orthopedic surgery, particularly with respect to preservation of muscle mass and functional capacity [3]. Creatine monohydrate is among the most extensively studied nutritional supplements in adult sports medicine and rehabilitation literature, with well-documented effects on energy metabolism, muscle hypertrophy, and recovery following injury or immobilization [4]. Despite its widespread use and favorable safety profile, creatine supplementation remains underexplored in pediatric orthopedic surgery populations due to ethical concerns, historical caution regarding supplementation in youth, and a paucity of targeted clinical trials.
This narrative review integrates mechanistic, clinical, and rehabilitative evidence to contextualize the potential role of creatine supplementation in recovery after pediatric and adolescent knee arthroscopy. By synthesizing adult data with developmental considerations and limited pediatric evidence, this review aims to identify actionable knowledge gaps and advocate for future pediatric clinical research.
Importantly, this review extends beyond a traditional narrative synthesis by integrating translational evidence and proposing a clinically actionable framework to guide future pediatric orthopedic trials. To ensure methodological transparency, a structured literature search was conducted across PubMed, Scopus, and Google Scholar to identify relevant studies published from January 2000 through December 2024. Search terms included combinations of “creatine supplementation,” “knee arthroscopy,” “orthopedic surgery,” “rehabilitation,” “muscle atrophy,” “GLUT4,” “pediatric,” and “adolescent.” Articles were selected based on relevance to post-operative musculoskeletal recovery, the mechanistic effects of creatine on skeletal muscle, and clinical rehabilitation outcomes. Given the absence of pediatric surgical trials, adult orthopedic and mechanistic studies were intentionally incorporated to provide a translational context. The evidence was synthesized narratively rather than systematically, with emphasis on biological plausibility, consistency of clinical findings, and identification of knowledge gaps to inform future pediatric research. Study selection prioritized higher-level evidence, including randomized controlled trials, systematic reviews, and mechanistic studies directly relevant to skeletal muscle physiology and post-operative recovery. While a formal risk-of-bias assessment was not performed, emphasis was placed on consistency of findings across studies and biological plausibility.
Biological Rationale for Creatine in Musculoskeletal Recovery
Creatine is a non-essential nitrogen-containing compound synthesized endogenously from glycine, arginine, and methionine, with the majority stored in skeletal muscle as free creatine and phosphocreatine. Its primary physiological function is to buffer intracellular adenosine triphosphate levels through the phosphocreatine system. This buffering system provides primary support for energy-demanding processes, including muscle contraction, tissue repair, and cellular regeneration. These mechanisms are particularly relevant in post-operative states characterized by inflammation, disuse, and metabolic stress [5].
Recent studies have demonstrated that creatine supplementation attenuates muscle protein breakdown, preserves muscle cross-sectional area during immobilization, and accelerates strength recovery during rehabilitation [6]. In addition, creatine has been shown to increase skeletal muscle GLUT4 expression and glucose uptake, thereby enhancing metabolic efficiency during recovery [7]. These biological effects appear to extend across age groups and may be especially important to study in pediatric and adolescent patients, whose musculoskeletal systems are in an anabolic and adaptive state. Preservation of lean mass and metabolic efficiency during post-operative recovery may have long-term implications for function and athletic participation [8].
Post-operative recovery following knee arthroscopy: Evidence from adult populations
Post-operative recovery following knee arthroscopy typically progresses through structured phases emphasizing restoration of range of motion, gradual strengthening, neuromuscular control, and sport-specific performance [2]. Adult orthopedic and sports medicine literature has extensively examined creatine supplementation across these recovery stages. Randomized controlled trials have demonstrated enhanced quadriceps strength, increased muscle cross-sectional area, and improved maximal knee extension power in adults receiving creatine during rehabilitation after immobilization or surgery [9].
Creatine supplementation has also been associated with improved muscle glycogen storage and reductions in inflammatory markers following exercise and injury, supporting its role in mitigating post-operative fatigue and catabolic stress [10]. Although some studies have reported neutral findings in older arthroplasty populations, differences in age, comorbidities, and surgical magnitude likely account for this variability [11]. Collectively, adult data suggest that creatine supplementation may favorably influences multiple dimensions of post-operative recovery that are directly relevant to pediatric arthroscopic rehabilitation.
Translational Relevance to Pediatric and Adolescent Patients
Despite robust evidence in adults, direct studies of creatine supplementation in pediatric and adolescent surgical populations remain scarce. This absence reflects a lack of targeted investigation rather than a lack of biological plausibility. Adolescents undergoing knee arthroscopy experience post-operative muscle inhibition, strength loss, and neuromuscular deficits such as those observed in adults, often compounded by the demands of growth and high athletic expectations [12].
Limited pediatric data outside surgical contexts suggest that creatine supplementation is generally well tolerated in youth athletes and may confer performance and recovery benefits [13]. Adult studies in anterior cruciate ligament (ACL) reconstruction rehabilitation have demonstrated accelerated strength recovery and improved functional outcomes with creatine supplementation, providing a strong translational rationale for pediatric investigation [9]. Given the shared physiological stressors of surgery and rehabilitation across age groups, the pediatric orthopedic population represents a logical and clinically relevant target for future trials.
Mechanistic Pathways Supporting Pediatric Investigation
Beyond its role in energy buffering, creatine supplementation has been shown to modulate inflammatory and oxidative stress pathways that are highly relevant in the post-operative environment. Reductions in pro-inflammatory cytokines and markers of muscle damage have been reported in adult studies, suggesting potential benefits in attenuating post-operative inflammation and muscle catabolism [10]. Creatine has also been implicated in enhancing neuromuscular activation and muscle fiber recruitment, processes essential for effective rehabilitation and functional recovery [14].
In pediatric and adolescent patients, these mechanisms may be amplified due to the inherently anabolic nature of the developing musculoskeletal system. Supporting muscle preservation and neuromuscular recovery during critical periods of growth may therefore yield both short-term and long-term functional benefits, further strengthening the rationale for pediatric-specific clinical investigation [3]. Taken together, these converging structural, metabolic, and inflammatory mechanisms form an integrated pathway through which creatine supplementation may enhance post-operative recovery, as illustrated in Fig. 1.
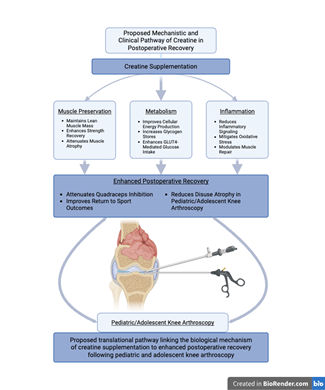
Figure 1 illustrates how creatine supplementation may support postoperative recovery through complementary structural, metabolic, and anti-inflammatory mechanisms that collectively contribute to improved strength recovery and functional outcomes. Created with BioRender.com.
Clinical and Ethical Considerations in Pediatric Supplementation Research
The limited availability of pediatric data on creatine supplementation reflects longstanding ethical considerations surrounding clinical research in children and adolescents. Contemporary pediatric research frameworks emphasize the principles of minimal risk, proportional risk-benefit balance, and the ethical obligation to generate age-specific data when adult evidence cannot be reliably extrapolated to pediatric populations without a targeted study, necessitating careful ethical and regulatory design tailored to children’s needs [15]. In orthopedic surgery, where post-operative recovery intersects with growth, neuromuscular development, and long-term function, reliance on adult data alone may inadequately capture pediatric-specific risks and benefits. Federal and ethical frameworks governing pediatric clinical research emphasize the need for age‑specific data when adult evidence cannot be reliably extrapolated, and support carefully designed pilot studies in minimal‑risk contexts when there is biological plausibility and low anticipated risk [15]. Within this framework, creatine supplementation represents an ethically appropriate candidate for pediatric investigation, given its endogenous production, dietary prevalence, and favorable safety profile in both adults and emerging pediatric research [16].
Narrative synthesis is particularly appropriate in this context, where strong mechanistic plausibility and adult clinical evidence exist alongside a clear lack of pediatric surgical trials. Future studies must prioritize age-appropriate dosing, rigorous safety monitoring, and clinically meaningful functional endpoints relevant to pediatric orthopedic surgery recovery.
Clinical Translation and Practical Implications
The translational significance of these findings lies in their direct applicability to post-operative rehabilitation strategies. Creatine supplementation represents a low-cost, accessible, and biologically plausible adjunct that may be integrated into existing rehabilitation protocols without substantial modification. Its effects on muscle preservation, metabolic efficiency, and inflammation directly target key determinants of recovery following knee arthroscopy, including quadriceps inhibition, disuse atrophy, and delayed functional progression. From a clinical perspective, incorporating perioperative nutritional strategies alongside physical therapy may enhance recovery trajectories and improve return-to-sport outcomes. However, implementation in pediatric populations must be guided by prospective clinical evidence, highlighting the importance of targeted investigation.
Integrated Future Directions and Specific Aims for Primary Pediatric Clinical Research
The existing literature strongly supports the need for prospective pediatric clinical trials evaluating creatine supplementation as an adjunct to post-operative rehabilitation following knee arthroscopy. Recent adult orthopedic rehabilitation studies consistently demonstrate improvements in muscle strength, preservation of lean mass, enhanced metabolic efficiency, and attenuation of post-operative catabolism with creatine supplementation, providing a robust evidentiary foundation for pediatric investigation [6].
The first specific aim of a future clinical trial should be to determine whether perioperative creatine supplementation improves post-operative muscle strength and functional recovery in pediatric and adolescent patients undergoing knee arthroscopy. This aim is supported by recent adult data on creatine supplementation during orthopedic rehabilitation; however, these findings have not yet been specifically evaluated in pediatric and adolescent surgical populations [12].
The second specific aim should be to evaluate the effects of creatine supplementation on post-operative muscle mass preservation and metabolic efficiency in pediatric and adolescent patients. Studies from the past few years demonstrating attenuation of disuse atrophy, increased skeletal muscle GLUT4 expression, and enhanced glycogen storage provide strong mechanistic justification for examining these outcomes in younger surgical populations [7].
The third specific aim should be to assess the safety and tolerability of creatine supplementation in the perioperative pediatric orthopedic population. Although available evidence suggests a favorable safety profile, systematic pediatric surgical data are required to inform clinical guidelines, parental counseling, and long-term post-operative management [16]. Together, these aims establish a structured and testable clinical framework that bridges existing adult evidence with pediatric-specific research needs.
Summary of Key Studies
Recent randomized controlled trials and mechanistic studies have increasingly demonstrated that creatine supplementation significantly enhances muscle cross-sectional area and strength in immobilized adult patients undergoing rehabilitation [3]. It has been shown to increase GLUT4 protein expression in skeletal muscle, which supports improved glucose uptake and greater muscle energy efficiency [6]. Creatine supplementation can enhance recovery of muscle force following exercise-induced muscle damage in adults [17]. However, clinical trials in post-operative orthopedic settings such as ACL reconstruction have not shown accelerated strength recovery compared with controls [12]. In addition, Cordingley et al. (2022) [10] documented reductions in inflammatory markers and muscle damage, reinforcing creatine’s anti-inflammatory and anti-catabolic effects.
Collectively, these findings support the potential role of creatine in enhancing post-operative recovery following orthopedic procedures by promoting tissue repair, reducing inflammation, and improving functional strength outcomes. Although direct extrapolation to pediatric populations warrants caution, the consistency of these mechanistic and clinical effects in adult populations provides a strong foundation for further investigation. To illustrate how adult creatine studies converge across structural, metabolic, and inflammatory domains of recovery, the key findings from representative trials are summarized in Table 1.
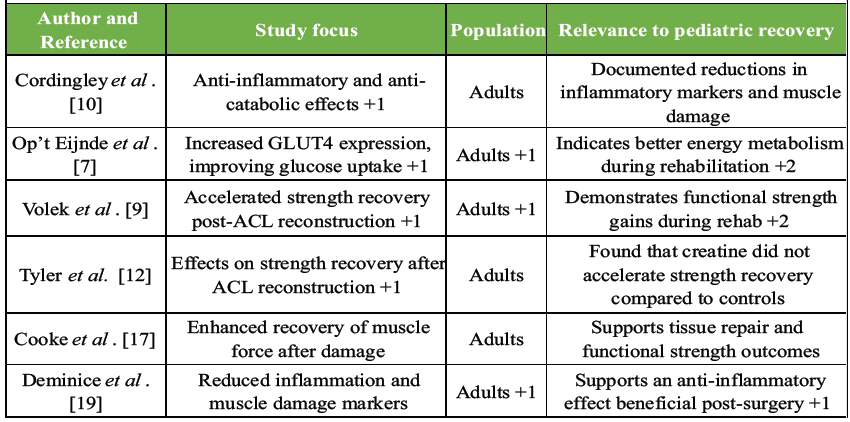
Table 1: Summary of key mechanistic and clinical studies supporting creatine supplementation in orthopedic recovery.
Table 1 synthesizes key adult clinical and mechanistic studies that collectively demonstrate how creatine supplementation supports post-operative recovery through complementary structural, metabolic, and biologic pathways. Hespel et al. (2001) [18] showed that creatine supplementation enhances muscle cross-sectional area and strength during rehabilitation following immobilization, underscoring its role in structural muscle recovery. Op’t Eijnde et al. (2001) [7] further demonstrated that creatine supplementation increases skeletal muscle GLUT4 protein expression after immobilization, supporting improved glucose uptake and enhanced metabolic efficiency during rehabilitation. In functional recovery settings, Volek et al. (2004) [9] reported accelerated strength recovery following ACL reconstruction among individuals receiving creatine compared with control groups. In addition to these structural and metabolic effects, Deminice et al. (2013) [19] documented reductions in inflammatory markers and indices of muscle damage associated with creatine supplementation, providing evidence for its anti-inflammatory and anti-catabolic properties during periods of physiologic stress. Although these investigations were conducted exclusively in adult populations, the convergence of structural, metabolic, and inflammatory benefits across studies provides a biologically coherent rationale for investigating creatine supplementation in pediatric and adolescent patients undergoing knee arthroscopy.
IRB and Pilot Trial Justification Paragraph
The proposed pediatric clinical trial is ethically justified based on the minimal incremental risk posed by creatine supplementation, its endogenous nature, and its extensive prior use in adult and limited pediatric populations. The study would adhere to federal regulations governing pediatric research, including risk minimization strategies, age-appropriate assent, parental consent, and continuous safety monitoring [20]. Given the absence of pediatric surgical outcome data, a pilot trial is a proportionate and necessary step toward evidence-based post-operative care and aligns with ethical mandates to generate pediatric-specific evidence when extrapolation from adults is insufficient.
Limitations
This narrative review is limited by its reliance on adult data and mechanistic extrapolation in the absence of pediatric surgical trials. Variability in creatine dosing protocols and rehabilitation strategies across studies further limits direct generalizability. However, these limitations underscore a critical gap in pediatric orthopedic research and reinforce the need for future primary clinical investigation. Despite these limitations, the consistency of mechanistic and clinical findings across adult studies strengthens the translational validity of the proposed framework.
Creatine supplementation demonstrates consistent mechanistic and clinical benefits in adult orthopedic and rehabilitation settings, including preservation of lean muscle mass, attenuation of disuse-related atrophy, enhanced GLUT4-mediated glucose uptake, improved metabolic efficiency, reductions in inflammatory signaling, and accelerated strength recovery in select post-operative populations. Although findings are not universally positive across all surgical contexts, the convergence of structural, metabolic, and anti-inflammatory effects provides a coherent biological framework supporting its potential role as an adjunct to post-operative rehabilitation. These outcomes directly address key determinants of recovery following knee arthroscopy, including muscle preservation, neuromuscular function, and restoration of strength.
Despite robust adult data and emerging safety evidence in youth athletic populations, no prospective pediatric surgical trials have evaluated creatine supplementation in the context of knee arthroscopy. This gap represents a critical opportunity for targeted investigation. Given creatine’s endogenous production, favorable safety profile, and biologically plausible mechanisms, carefully designed pediatric clinical trials are warranted to determine its efficacy, optimal dosing strategies, and safety in perioperative orthopedic care. Generating pediatric-specific evidence is essential to inform evidence-based rehabilitation strategies and optimize functional recovery in this growing patient population. This work provides a translational foundation for future investigation and supports the integration of perioperative nutritional strategies into evolving models of pediatric orthopedic rehabilitation.
Creatine supplementation may represent a safe, low-cost adjunct to improve post-operative muscle preservation, metabolic recovery, and functional outcomes following pediatric knee arthroscopy. While adult data are promising, pediatric orthopedic surgeons should recognize the current lack of pediatric-specific evidence and consider creatine as a candidate for future clinical trials rather than routine clinical use until pediatric-specific safety and efficacy data are established.
References
- 1. Zhang AL, Allen CR. 2014: Knee arthroscopy: The basics. In: Wolf SW, editor. Operative Techniques in Orthopaedic Surgery. Vol. 1., Ch. 32. New York: Lippincott Williams and Wilkins. [Google Scholar] [PubMed]
- 2. Logerstedt DS, Scalzitti D, Risberg MA, Engebretsen L, Webster KE, Feller J, et al. Knee stability and movement coordination impairments: Knee ligament sprain revision 2017. J Orthop Sports Phys Ther 2017;47:1-47. [Google Scholar] [PubMed]
- 3. Hirsch KR, Wolfe RR, Ferrando AA. Pre- and post-surgical nutrition for preservation of muscle mass, strength, and functionality following orthopedic surgery. Nutrients 2021;13:1675. [Google Scholar] [PubMed]
- 4. Persky AM, Brazeau GA. Clinical pharmacology of the dietary supplement creatine monohydrate. Pharmacol Rev 2001;53:161-76. [Google Scholar] [PubMed]
- 5. Wyss M, Kaddurah-Daouk R. Creatine and creatinine metabolism. Physiol Rev 2000;80:1107-213. [Google Scholar] [PubMed]
- 6. Wang Z, Qiu B, Li R, Han Y, Petersen C, Liu S, et al. Effects of creatine supplementation and resistance training on muscle strength gains in adults <50 years of age: A systematic review and meta-analysis. Nutrients 2024;28:3665. [Google Scholar] [PubMed]
- 7. Op ‘t Eijnde B, Ursø B, Richter EA, Greenhaff PL, Hespel P. Effect of oral creatine supplementation on human muscle GLUT4 protein content after immobilization. Diabetes 2001;50:18-23. [Google Scholar] [PubMed]
- 8. Harmon KK, Stout JR, Fukuda DH, Pabian PS, Rawson ES, Stock MS. The application of creatine supplementation in medical rehabilitation. Nutrients 2021;27:1825. [Google Scholar] [PubMed]
- 9. Volek JS, Ratamess NA, Rubin MR, Gómez AL, French DN, McGuigan MM, et al. The effects of creatine supplementation on muscular performance and body composition responses to short-term resistance training overreaching. Eur J Appl Physiol 2004;91:628-37. [Google Scholar] [PubMed]
- 10. Cordingley DM, Cornish SM, Candow DG. Anti-inflammatory and anti-catabolic effects of creatine supplementation: A brief review. Nutrients 2022;27:544. [Google Scholar] [PubMed]
- 11. Roy BD, De Beer J, Harvey D, Tarnopolsky MA. Creatine monohydrate supplementation does not improve functional recovery after total knee arthroplasty. Arch Phys Med Rehabil 2005;86:1293-8. [Google Scholar] [PubMed]
- 12. Tyler TF, Nicholas SJ, Hershman EB, Glace BW, Mullaney MJ, McHugh MP. The effect of creatine supplementation on strength recovery after anterior cruciate ligament (ACL) reconstruction: A randomized, placebo-controlled, double-blind trial. Am J Sports Med 2004;32:383-8. [Google Scholar] [PubMed]
- 13. Metzl JD, Small E, Levine SR, Gershel JC. Creatine use among young athletes. Pediatrics 2001;108:421-5. [Google Scholar] [PubMed]
- 14. Burke R, Piñero A, Coleman M, Mohan A, Sapuppo M, Augustin F, et al. The effects of creatine supplementation combined with resistance training on regional measures of muscle hypertrophy: A systematic review with meta-analysis. Nutrients 2023;15:2116. [Google Scholar] [PubMed]
- 15. Institute of Medicine; 2004. Available from: https://www.ncbi.nlm.nih.gov/books/nbk25557 [Last accessed on 2026 Feb 02]. [Google Scholar] [PubMed]
- 16. Jagim AR, Kerksick CM. Creatine supplementation in children and adolescents. Nutrients 2021;18:664. [Google Scholar] [PubMed]
- 17. Cooke MB, Rybalka E, Williams AD, Cribb PJ, Hayes A. Creatine supplementation enhances muscle force recovery after eccentrically-induced muscle damage in healthy individuals. J Int Soc Sports Nutr 2009;2:13. [Google Scholar] [PubMed]
- 18. Hespel P, Op’t Eijnde B, Van Leemputte M, Ursø B, Greenhaff PL, Labarque V, et al. Oral creatine supplementation facilitates the rehabilitation of disuse atrophy and alters the expression of muscle myogenic factors in humans. J Physiol 2001;15:625-33. [Google Scholar] [PubMed]
- 19. Deminice R, Rosa FT, Franco GS, Jordao AA, De Freitas EC. Effects of creatine supplementation on oxidative stress and inflammatory markers after repeated-sprint exercise in humans. Nutrition 2013;29:1127-32. [Google Scholar] [PubMed]
- 20. U.S. Department of Health and Human Services. Additional Protections for Children Involved as Subjects in Research (45 CFR 46, Subpart D); 2018. Available from: https://www.hhs.gov/ohrp/regulations-and-policy/regulations/45-cfr-46/index.html. Accessed 2026 Feb 02. [Google Scholar] [PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 September 1, 2025 Operative Management of a Chronic Proximal Rectus Femoris Muscle Tear in a Collegiate Athlete: A Case Report
September 1, 2025 Operative Management of a Chronic Proximal Rectus Femoris Muscle Tear in a Collegiate Athlete: A Case Report August 1, 2026 Surgical Excision of a Rare Ventral Scapular Osteochondroma using the Prone “Chicken-Wing” Position: A Case Report
August 1, 2026 Surgical Excision of a Rare Ventral Scapular Osteochondroma using the Prone “Chicken-Wing” Position: A Case Report August 1, 2026 Serendipitous Healing of a Congenital Pseudoarthrosis of the Clavicle Following Acute Injury: A Case Report
August 1, 2026 Serendipitous Healing of a Congenital Pseudoarthrosis of the Clavicle Following Acute Injury: A Case Report August 1, 2026 Post-operative C5 Palsy Following Posterior Cervical Decompression and Fusion: A Case Report
August 1, 2026 Post-operative C5 Palsy Following Posterior Cervical Decompression and Fusion: A Case Report