
Intravenous tranexamic acid significantly reduces perioperative blood loss and blood transfusion requirements in primary total knee arthroplasty without increasing thromboembolic complications, supporting its routine use in blood conservation protocols
Dr P. Ambareesh, Department of Orthopaedics Vydehi Institute of Medical Sciences and Research Centre, Bengaluru, Karnataka, India. E-mail: ambareesh4589@vimsmail.com
Abstract
Introduction: Total knee arthroplasty (TKA) is associated with significant perioperative blood loss, often necessitating blood transfusions. Tranexamic acid (TXA), an antifibrinolytic agent, has been shown to reduce bleeding effectively. This study evaluated the efficacy and safety of intravenous TXA in reducing perioperative blood loss in patients undergoing primary unilateral TKA.
Materials and Methods: This prospective randomised controlled trial included 60 patients with Kellgren-Lawrence Grade 3 or 4 osteoarthritis undergoing primary unilateral TKA at a tertiary care centre. Patients were randomised into two groups: The TXA group (n = 30) received 1 g intravenous TXA before tourniquet release, while the control group (n = 30) received normal saline. Outcome measures included intraoperative blood loss, postoperative drain output, haemoglobin changes, and transfusion requirements.
Results: The TXA group demonstrated significantly lower intraoperative blood loss (205.33 vs. 305.67 mL, P < 0.001), total drain output (185.00 vs. 298.33 mL, P < 0.001), and proportional haemoglobin loss (14.19% vs. 19.98%, P < 0.001). Transfusion requirements were significantly reduced in the TXA group (6.67% vs. 26.67%, P = 0.039). No thromboembolic complications were observed in either group.
Conclusion: Intravenous TXA significantly reduces perioperative blood loss and transfusion requirements in TKA without increasing thromboembolic risk, supporting its routine use in blood conservation protocols.
Keywords: Tranexamic acid, total knee arthroplasty, blood loss, blood transfusion, antifibrinolytic.
Total knee arthroplasty (TKA) is a well-established surgical procedure for end-stage osteoarthritis that significantly improves pain and functional outcomes. However, TKA is associated with substantial perioperative blood loss, typically ranging from 800 to 1800 mL, which frequently necessitates allogeneic blood transfusion [1,2]. Reported transfusion rates vary widely from 10% to 67% depending on patient factors, surgical technique, and institutional protocols [3,4]. Allogeneic blood transfusion carries inherent risks, including transfusion reactions, transmission of infectious diseases, immunomodulation, and increased post-operative infection rates [5,6]. These concerns have driven the development of various blood conservation strategies, including controlled hypotension, autologous blood donation, cell salvage, and pharmacological interventions [7]. Tranexamic acid (TXA) is a synthetic derivative of lysine that competitively inhibits plasminogen activation, thereby preventing fibrin degradation and maintaining clot stability [8]. Multiple meta-analyses have demonstrated that TXA significantly reduces blood loss and transfusion requirements in TKA without increasing thromboembolic complications [9,10,11]. While TXA has been extensively studied in Western populations, there is relatively limited data from the Indian population, which may have different fibrinolytic profiles [12,13]. To assess the safety and effectiveness of intravenous TXA in reducing perioperative blood loss in patients receiving primary TKA at a tertiary care facility in India, a prospective randomised controlled trial was carried out.
This prospective randomised controlled trial was conducted at a tertiary care centre from January 2023 to December 2023 after obtaining Institutional Ethics Committee approval. Written informed consent was obtained from all participants. Sixty patients aged 50–75 years with Kellgren-Lawrence Grade 3 or 4 primary osteoarthritis of the knee scheduled for primary unilateral TKA were enrolled. Exclusion criteria included revision surgery, inflammatory arthritis, bleeding disorders or anticoagulant therapy, history of thromboembolic disease, allergy to TXA, severe cardiovascular or renal impairment, and pre-operative haemoglobin <10 g/dL. The ethical clearance from the institution for the study was taken, and the number is VIEC/2023/APP/PG/035. Patients were selected using randomised computer-generated random numbers into two groups of 30 patients each. The study followed a single-blinding technique where the patients of either group were not aware of the injection administered. The TXA group received 1 g (10 mL) of intravenous TXA administered 10 min before tourniquet release, while the control group received 10 mL of normal saline at the same time point. All surgeries were performed under spinal anaesthesia using a standard medial parapatellar approach with pneumatic tourniquet application, due to which the blood loss was minimal. Patients were managed with IV fluids for hypotension, and none of the patients in the study required a blood transfusion intraoperatively. A posterior-stabilised cemented prosthesis was implanted in all cases. A closed suction drain was placed in all patients and removed at 48 h postoperatively. Thromboprophylaxis with low molecular weight heparin was initiated 12 h postoperatively and continued for 2 weeks, as recommended in contemporary guidelines [14]. Outcome measures included intraoperative blood loss (estimated by weighing surgical mops), postoperative drain output at 24 and 48 h, haemoglobin levels (preoperative, postoperative day 1 and day 3), proportional haemoglobin loss, and transfusion requirements. Blood transfusion was indicated when haemoglobin dropped below 8 g/dL or when symptomatic anaemia occurred with haemoglobin between 8 and 10 g/dL. Patients were monitored for thromboembolic complications, including deep vein thrombosis (clinical assessment and Doppler ultrasonography if indicated) and pulmonary embolism. Sample size was calculated based on previous studies [12,15], estimating a mean difference of 200 mL in blood loss with a standard deviation of 250 mL, requiring 26 patients/group at 80% power and a 5% significance level; 30 patients/group were enrolled to account for dropouts. Statistical analysis was performed using the Statistical Package for the Social Sciences version 25.0. Continuous variables were compared using independent t-tests and categorical variables using chi-square or Fisher’s exact test. A P < 0.05 was considered statistically significant.
All 60 patients completed the study without any dropouts. Baseline demographic characteristics were comparable between the two groups. The mean age was 62.43 years in the TXA group and 63.47 years in the control group (P = 0.515). Gender distribution and baseline haemoglobin levels were similar between groups. (Chart 1).
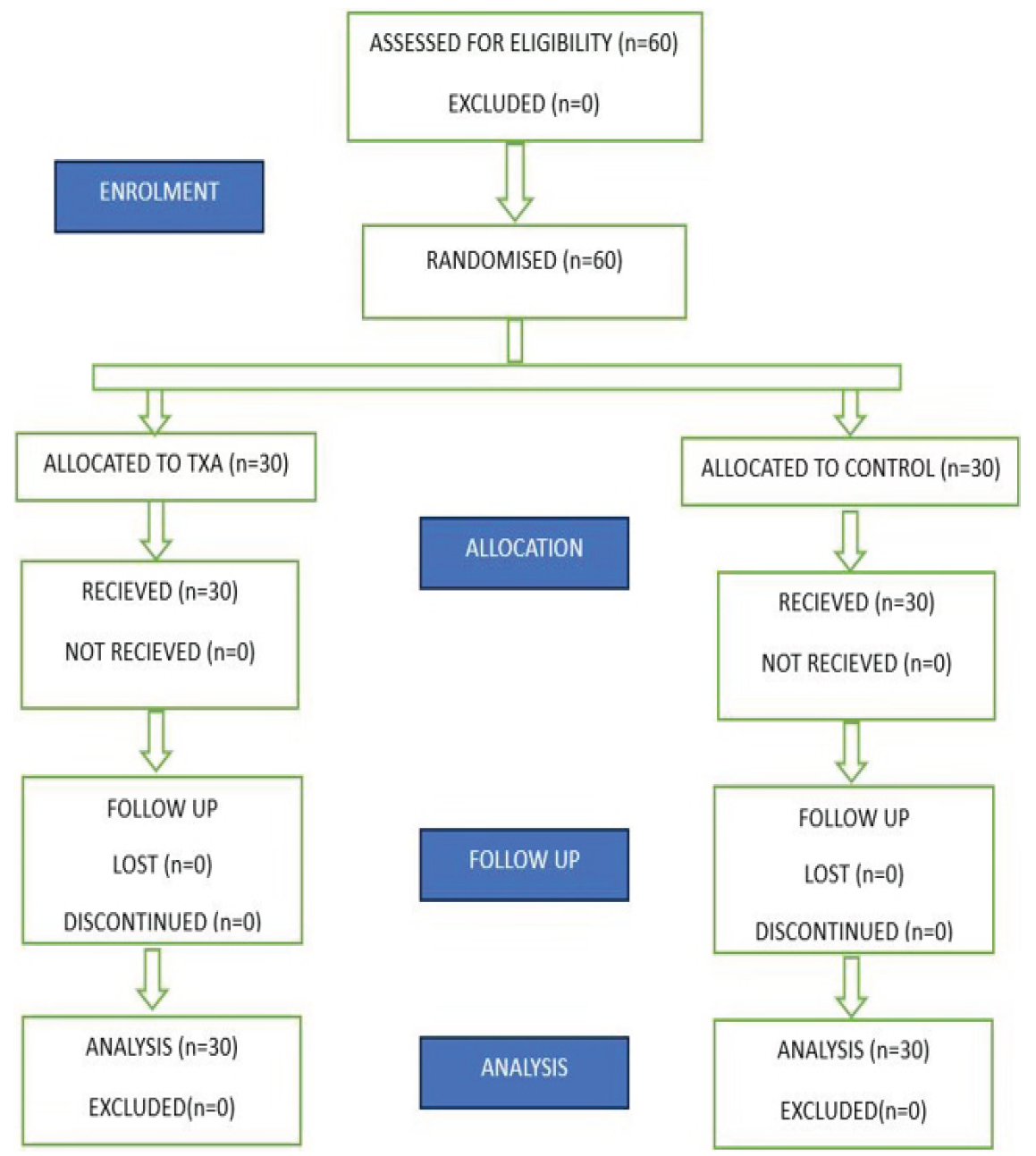
Chart 1: CONSORT flow diagram of patient enrollment, allocation, followup, and analysis.
Intraoperative blood loss was significantly lower in the TXA group compared to the control group (205.33 ± 52.41 mL vs. 305.67 ± 68.23 mL, P < 0.001). The mean reduction in intraoperative blood loss was 100.34 mL (32.8%) in the TXA group. Post-operative drain output was significantly reduced in the TXA group at both 24 h (115.00 ± 28.45 mL vs. 178.33 ± 42.67 mL, P < 0.001) and 48 h (70.00 ± 18.23 mL vs. 120.00 ± 32.56 mL, P < 0.001). Total drain output was 185.00 ± 38.92 mL in the TXA group compared to 298.33 ± 62.45 mL in the control group (P < 0.001), representing a 37.9% reduction (Table 1). Haemoglobin levels on post-operative day 1 and day 3 were significantly higher in the TXA group (Table 2).
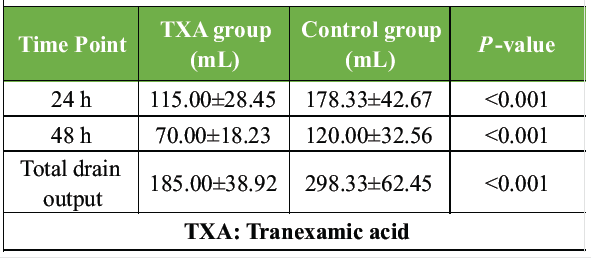
Table 1: Post-operative drain output
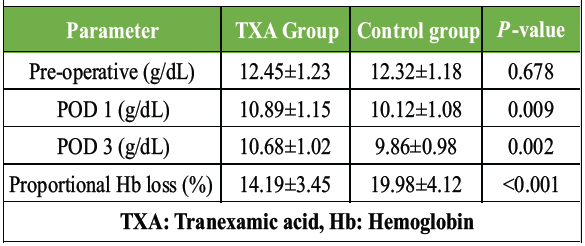
Table 2: Hemoglobin levels
The proportional haemoglobin loss was 14.19 ± 3.45% in the TXA group compared to 19.98 ± 4.12% in the control group (P < 0.001). These findings are consistent with the blood-sparing effects reported in previous meta-analyses [9,10,11,16]. Blood transfusion was required in 2 patients (6.67%) in the TXA group compared to 8 patients (26.67%) in the control group (P = 0.039), representing a 75% reduction in transfusion rate. This significant reduction is clinically meaningful as it reduces exposure to transfusion-related risks [5,6]. No thromboembolic complications, including deep vein thrombosis or pulmonary embolism, were observed in either group during the study period, consistent with the safety profile reported in large meta-analyses [9,10,11,17].
This study demonstrates that intravenous TXA significantly reduces perioperative blood loss and transfusion requirements in patients undergoing primary TKA. Our findings are consistent with the growing body of evidence supporting the efficacy and safety of TXA in joint arthroplasty surgery [9,10,11,16]. The 32.8% reduction in intraoperative blood loss and 37.9% reduction in post-operative drain output observed in our study are comparable to results reported in previous randomised controlled trials [1,12,13,15]. Gautam et al. [12] reported similar findings in the Indian population, with a mean post-operative blood loss of 272.5 mL in the TXA group compared to 685 mL in the placebo group. Kundu et al. [1] demonstrated a 40% reduction in blood loss with a single dose of TXA. Kumar et al. [15] also reported significant reductions in perioperative blood loss with TXA administration. The timing of TXA administration before tourniquet release is supported by Tanaka et al. [8], who demonstrated that maximum haemostatic effect occurs when TXA is given preoperatively and at tourniquet deflation. Dhillon et al. [13] confirmed the efficacy of TXA in bilateral TKA in the Indian population, reporting significant reductions in haemoglobin drop and transfusion requirements. The transfusion rate in our control group (26.67%) is consistent with reported rates of 18–67% in TKA without TXA [3,4,7]. The 75% reduction in transfusion rate achieved with TXA has significant clinical and economic implications. Blood transfusion is associated with increased risk of post-operative infection, immunomodulation, and longer hospital stay [5,6]. Yang et al. [9], in their meta-analysis of 15 randomised controlled trials, demonstrated that TXA reduces transfusion rates by approximately 50% without increasing thromboembolic complications. Alshryda et al. [10], in their systematic review of 19 trials, reported a risk ratio of 2.56 for reduction in transfusion with TXA use. These findings have been incorporated into contemporary clinical practice guidelines recommending routine TXA use in TKA [17,18]. The safety of TXA regarding thromboembolic complications has been a concern given its antifibrinolytic mechanism. However, our study observed no thromboembolic events in either group. This is consistent with multiple large meta-analyses that have demonstrated no increased risk of deep vein thrombosis or pulmonary embolism with TXA use in TKA [9,10,11,16,17]. Poeran et al. [11], in a large retrospective analysis of over 872,000 patients undergoing joint arthroplasty, found that TXA was associated with decreased odds of blood transfusion and complications without increased thromboembolic risk. The mechanism by which TXA reduces bleeding without increasing thrombosis may be related to its localised action on the fibrinolytic system activated during surgery rather than a systemic prothrombotic effect [8,18]. This study has several limitations, including its single-centre design, relatively small sample size, and lack of long-term follow-up. The study did not compare different doses or routes of TXA administration, which have been evaluated in other studies [16,18]. Hidden blood loss was not calculated, which may underestimate total blood loss. Future studies with larger sample sizes and longer follow-up periods are warranted to further evaluate the safety profile of TXA in the Indian population.
Intravenous TXA administered before tourniquet release significantly reduces perioperative blood loss and transfusion requirements in patients undergoing primary TKA without increasing the risk of thromboembolic complications. These findings support the routine incorporation of TXA into blood conservation protocols for TKA.
Intravenous tranexamic acid administered before tourniquet release is a safe and effective strategy to reduce perioperative blood loss and blood transfusion requirements in primary total knee arthroplasty without increasing thromboembolic complications.
References
- 1. Kundu R, Das A, Basunia SR, Bhattacharyya T, Chattopadhyay S, Mukherjee A. Does a single loading dose of tranexamic acid reduce perioperative blood loss and transfusion requirements after total knee replacement surgery? A randomized, controlled trial. J Nat Sci Biol Med 2015;6:94-9. [Google Scholar] [PubMed]
- 2. Spahn DR. Anemia and patient blood management in hip and knee surgery: A systematic review of the literature. Anesthesiology 2010;113:482-95. [Google Scholar] [PubMed]
- 3. Bierbaum BE, Callaghan JJ, Galante JO, Rubash HE, Tooms RE, Welch RB. An analysis of blood management in patients having a total hip or knee arthroplasty. J Bone Joint Surg Am 1999;81:2-10. [Google Scholar] [PubMed]
- 4. Prasad N, Padmanabhan V, Mullaji A. Blood loss in total knee arthroplasty: An analysis of risk factors. Int Orthop 2007;31:39-44. [Google Scholar] [PubMed]
- 5. Hill GE, Frawley WH, Griffith KE, Forestner JE, Minei JP. Allogeneic blood transfusion increases the risk of postoperative bacterial infection: A meta-analysis. J Trauma 2003;54:908-14. [Google Scholar] [PubMed]
- 6. Banerjee S, Kapadia BH, Issa K, McElroy MJ, Khanuja HS, Harwin SF, et al. Postoperative blood loss prevention in total knee arthroplasty. J Knee Surg 2013;26:395-400. [Google Scholar] [PubMed]
- 7. Lemaire R. Strategies for blood management in orthopaedic and trauma surgery. J Bone Joint Surg Br 2008;90:1128-36. [Google Scholar] [PubMed]
- 8. Tanaka N, Sakahashi H, Sato E, Hirose K, Ishima T, Ishii S. Timing of the administration of tranexamic acid for maximum reduction in blood loss in arthroplasty of the knee. J Bone Joint Surg Br 2001;83:702-5. [Google Scholar] [PubMed]
- 9. Yang ZG, Chen WP, Wu LD. Effectiveness and safety of tranexamic acid in reducing blood loss in total knee arthroplasty: A meta-analysis. J Bone Joint Surg Am 2012;94:1153-9. [Google Scholar] [PubMed]
- 10. Alshryda S, Sarda P, Sukeik M, Nargol A, Blenkinsopp J, Mason JM. Tranexamic acid in total knee replacement: A systematic review and meta-analysis. J Bone Joint Surg Br 2011;93:1577-85. [Google Scholar] [PubMed]
- 11. Poeran J, Rasul R, Suzuki S, Danninger T, Mazumdar M, Opperer M, et al. Tranexamic acid use and postoperative outcomes in patients undergoing total hip or knee arthroplasty in the United States: Retrospective analysis of effectiveness and safety. BMJ 2014;349:g4829. [Google Scholar] [PubMed]
- 12. Gautam PL, Katyal S, Yamin M, Singh A. Effect of tranexamic acid on blood loss and transfusion requirement in total knee replacement in the Indian population: A case series. Indian J Anaesth 2011;55:590-3. [Google Scholar] [PubMed]
- 13. Dhillon MS, Bali K, Prabhakar S. Tranexamic acid for control of blood loss in bilateral total knee replacement in a single stage. Indian J Orthop 2011;45:148-52. [Google Scholar] [PubMed]
- 14. Falck-Ytter Y, Francis CW, Johanson NA, Curley C, Dahl OE, Schulman S, et al. Prevention of VTE in orthopedic surgery patients: Antithrombotic therapy and prevention of thrombosis, 9th ed: American college of chest physicians evidence-based clinical practice guidelines. Chest 2012;141 2 Suppl:e278S-325. [Google Scholar] [PubMed]
- 15. Kumar D, Sharma A, Sharma G, Trivedi A. A comparative study of blood loss with and without infusion of tranexamic acid in total knee replacement. Cureus 2022;14:e27737. [Google Scholar] [PubMed]
- 16. Zhang H, Chen J, Chen F, Que W. The effect of tranexamic acid on blood loss and use of blood products in total knee arthroplasty: A meta-analysis. Knee Surg Sports Traumatol Arthrosc 2012;20:1742-52. [Google Scholar] [PubMed]
- 17. Fillingham YA, Ramkumar DB, Jevsevar DS, Yates AJ, Bini SA, Clarke HD, et al. Tranexamic acid in total joint arthroplasty: The endorsed clinical practice guides of the American association of hip and knee surgeons, American society of regional anesthesia and pain medicine, American academy of orthopaedic surgeons, hip society, and knee society. Reg Anesth Pain Med 2019;44:7-11. [Google Scholar] [PubMed]
- 18. Prakash J, Seon JK, Song EK, Lee DH, Yang HY, Jin C. Is combined administration of tranexamic acid better than both intravenous and topical regimes for total loss, hidden loss and post-operative swelling? A randomized control trial. Indian J Orthop 2018;52:117-23. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2025 Does Multiple Intravenous Tranexamic Acid Doses in Patients Undergoing Total Knee Arthroplasty using Kinematic Alignment without Tourniquet Application show any Difference in Blood Loss, Transfusion Requirements and Hospital Stays: A Randomized Controlled Study
March 1, 2025 Does Multiple Intravenous Tranexamic Acid Doses in Patients Undergoing Total Knee Arthroplasty using Kinematic Alignment without Tourniquet Application show any Difference in Blood Loss, Transfusion Requirements and Hospital Stays: A Randomized Controlled Study April 10, 2024 Evaluating the Efficacy and Safety of Combined Administration of Systemic and Topical Tranexamic Acid in Total Knee Arthroplasty
April 10, 2024 Evaluating the Efficacy and Safety of Combined Administration of Systemic and Topical Tranexamic Acid in Total Knee Arthroplasty June 1, 2026 Role of Tranexamic Acid in Orthopedic Trauma: Current Evidence, Clinical Applications, and Ongoing Controversies
June 1, 2026 Role of Tranexamic Acid in Orthopedic Trauma: Current Evidence, Clinical Applications, and Ongoing Controversies June 1, 2025 Evaluation of Efficacy of Tranexamic Acid on Blood Loss in Surgically Managed Intertrochanteric Fractures
June 1, 2025 Evaluation of Efficacy of Tranexamic Acid on Blood Loss in Surgically Managed Intertrochanteric Fractures