
Tranexamic acid can be an effective adjunct in orthopedic trauma for reducing blood loss and transfusion requirements, but its appropriate use still requires careful consideration of indications, timing, dosage, and safety concerns.
Dr. Zakir Ali Shah, Department of Trauma and Orthopedics, Rashid Hospital, Muhammad Bin Rashid Medical University, Dubai, United Arab Emirates. E-mail: drzakiralishah@gmail.com
Abstract
Introduction: The worldwide burden of traumatic injuries is increasing daily due to industrial and mechanical development. Traumatic injuries often lead to hemorrhage, which is a major contributor to illness and death in cases of orthopedic trauma. Trauma induces coagulopathy, fibrinolysis, and hemorrhage, which together increase the demand for blood transfusion. Pelvic fractures are linked with significant blood loss that often requires blood transfusion. Hemorrhage in trauma patients is commonly managed with blood transfusion and blood substitutes. Tranexamic acid (TXA), an agent that prevents fibrinolysis, has been increasingly used to minimize bleeding with high efficacy and safety in major trauma surgeries such as pelvic fractures.
Materials and Methods: We reviewed the literature on certain studies (clinical trials, research studies, and meta-analyses) that evaluated the application of TXA in orthopedic trauma cases. Such as pelvic and hip fractures, long bone fractures, and polytrauma on PubMed, Scopus, and Google Scholar.
Results: Most studies support that TXA effectively decreases blood loss and the necessity for blood transfusions during surgery, especially when used soon after an injury. It has been found safe, as it does not escalate the risk of thromboembolic incidents.
Discussion: The use of TXA is widely accepted; however, there is still debate regarding the dose, timing, and patient selection across hospitals. These inconsistencies highlight the need for clearer guidance and standardized practice.
Conclusion: Transamine is an effective and safe antifibrinolytic agent for reducing blood loss in orthopedic trauma. However, further high quality studies are required to establish standardized protocols for its use across different fracture types and trauma scenarios.
Keywords: Tranexamic acid, orthopedic trauma, blood loss, pelvic fracture, blood transfusion.
Orthopedic trauma is a worldwide health challenge and considered an important cause of morbidity, disability, and hospital admissions as a result of the severity of the injuries and complex fracture patterns [1,2].
All age groups encounter fractures. High-energy fractures such as long bone, pelvic, and hip fractures are seen in young adults with road traffic accidents, and older adults experience fragility fractures with low-energy trauma, such as slips and falls. These injuries are often associated with significant blood loss, which requires blood transfusions, longer hospital stays, and contributes to postoperative complications [2,3]. A key factor that increases bleeding in trauma patients is trauma-induced coagulopathy, a complicated process marked by endothelial dysfunction, platelet impairment, and dysregulated fibrinolysis, which occurs in many patients after injury. In particular, hyperfibrinolysis destabilizes clot formation and can worsen ongoing hemorrhage. Blood loss can be life threatening, and blood transfusion is frequently required. Blood transfusion can have side effects such as immunological/allergic reactions, infection, and cardiovascular complications [3,4].
Tranexamic acid (TXA), a synthetic lysine derivative, prevents the activation of plasminogen, stabilizes hemostasis, and reduces bleeding. Over the past two decades, TXA has been widely used in trauma and orthopedic surgery [4]. Recent evidence suggests that TXA may have biological effects beyond bleeding control, including possible influences on inflammation and skeletal health [5].
Structure of TXA
TXA is synthesized from the amino acid and lysine. Its structural similarity to lysine is the key to its antifibrinolytic activity (Fig. 1). By competitively binding to plasminogen, TXA inhibits its conversion to plasmin and thereby reduces fibrin degradation.
Figure 1: Tranexamic acid (TXA) – chemical structure. Chemical structure of TXA showing the cyclohexane ring with carboxylic acid and aminoethyl substituents.
Mechanism of action of TXA
Early administration of TXA reduces blood loss in patients with significant bleeding, which reduces the risk of mortality. It has been observed that TXA may also have an anti‐inflammatory effect, owing to its inhibition of plasmin. TXA prevents activation of plasminogen to plasmin, thereby preventing fibrin degradation and promoting clot stabilization [4] (Fig. 2).
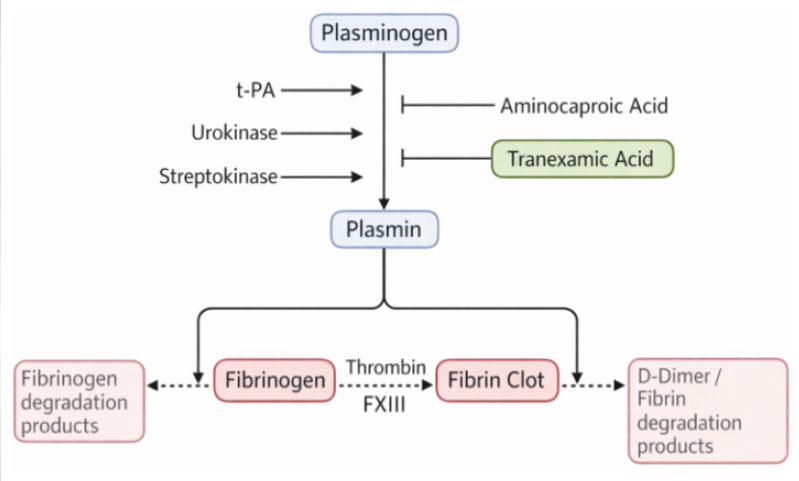
Figure 2: Mechanism of action of tranexamic acid. Schematic illustration showing the mechanism of action of tranexamic acid in fibrinolysis. Plasminogen is converted to plasmin by tissue plasminogen activator (t-PA), urokinase, and streptokinase. Tranexamic acid, similar to aminocaproic acid, inhibits plasminogen activation and plasmin activity, thereby reducing fibrin and fibrinogen degradation and limiting the formation of D-dimer and fibrin degradation products.
Large multicenter trials have demonstrated that early TXA administration, especially within the first 3 h after injury, reduces mortality in trauma patients with significant bleeding [6,7].
TXA has repeatedly demonstrated a reduction in perioperative blood loss and the requirement for blood transfusions, particularly in operations such as total hip and knee arthroplasty and complex fracture surgery [8,9]. Several studies have evaluated the use of TXA in hip fractures, pelvic injuries, and long bone fractures and have reported promising results [10]. Despite these positive results, TXA use in orthopedic trauma cases is still not routine and there is ongoing debate about the dose, timing of administration, and selection of patients in complex scenarios [11]. To better understand the current evidence and clarify these uncertainties, we conducted a comprehensive review of the literature on TXA use in orthopedic trauma..
A thorough literature review was performed using PubMed, Scopus, and Google Scholar to discover studies evaluating the use of TXA in orthopedic trauma. The search included publications from January 2000 to January 2025. Combinations of keywords were used, including: TXA, orthopedic trauma, pelvic and hip fractures, long bone fracture, acetabular fracture, polytrauma, blood loss, and transfusion. All the titles and abstracts that were obtained underwent a screening process. Articles in full text were evaluated for eligibility according to established criteria.
Inclusion criteria
1. Human studies
2. Orthopedic trauma cases
3. TXA administered by any route
4. Reported clinical outcomes such as blood loss, transfusion requirements, complications, or mortality.
Exclusion criteria
1. Non-orthopedic trauma studies
2. Case reports
3. Review articles without original data
4. Animal studies
5. Conference abstracts without full text.
Exclusion criteria
- Non-orthopedic trauma studies
- Case reports
- Review articles without original data
- Animal studies
- Conference abstracts without full text.
Data extracted from eligible studies included study design, sample size, fracture type, TXA dose and route, timing of administration, and primary clinical outcomes. Disagreements during screening or extraction were resolved through discussion among the reviewers. A total of 312 records were taken from database search (PubMed, n = 142; Scopus, n = 108; Google Scholar, n = 62). After duplicate removal, 198 records remained for screening. Of these, 124 records were excluded for not involving orthopedic trauma, not including a TXA intervention, being review articles without original data, or being non-clinical or animal studies. Out of the 74 full-text articles reviewed for eligibility, 42 were excluded because they either lacked clinical outcomes, were categorized as case reports or small series, contained incomplete data, or were merely conference abstracts. Finally, 16 studies were included that satisfied the inclusion criteria. The process of selecting studies is shown in a flowchart following the Preferred Reporting Items for Systematic reviews and Meta-Analyses flow diagram (Fig. 3).
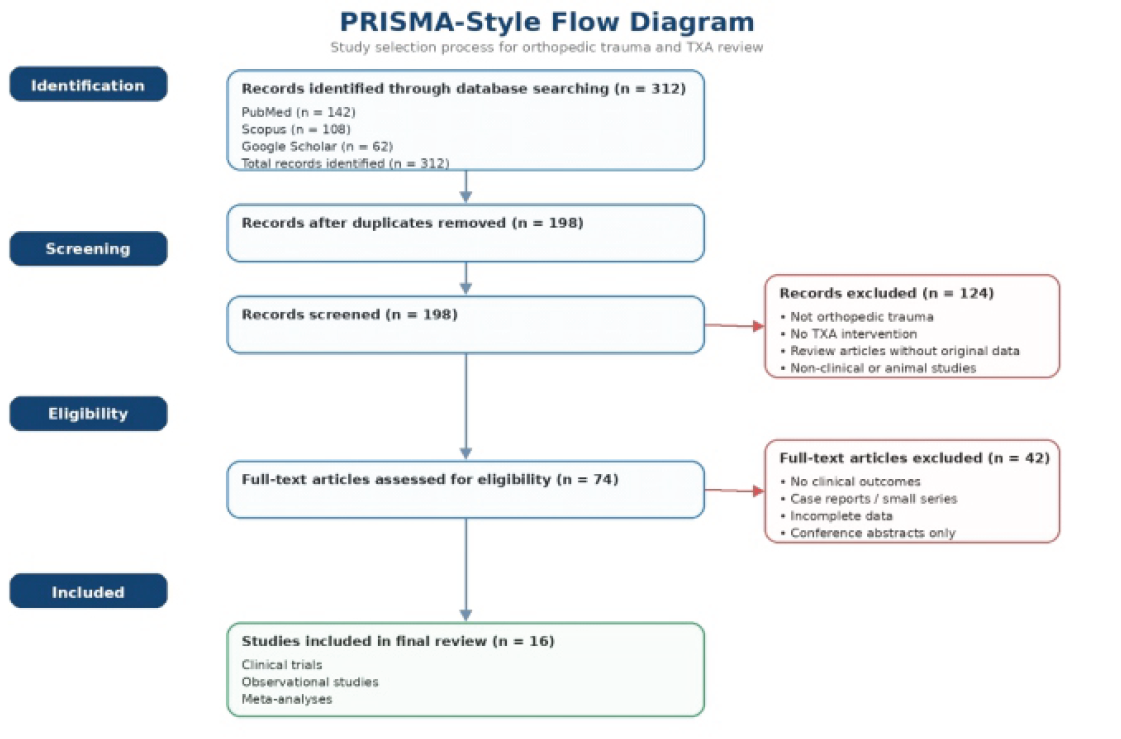
Figure 3: Preferred Reporting Items for Systematic Reviews and Meta-Analyses format flow diagram showing the procedure for selecting studies.
Sixteen studies that satisfied the inclusion criteria were incorporated into the final analysis. These studies included randomized controlled trials, observational cohort studies, and meta-analyses that evaluated the efficacy and safety of TXA in orthopedic trauma cases.
Study characteristics
The included studies covered a broad spectrum of orthopedic trauma conditions, including hip fractures, pelvic and acetabular injuries, long bone fractures, and polytrauma. Sample sizes ranged from 60 to over 20,000 participants, with TXA administered through intravenous (IV), topical, or mixed routes. Dosing regimens varied widely, from fixed 1 g boluses to weight-based protocols (10–25 mg/kg). Most studies evaluated perioperative blood loss, transfusion requirements, and thromboembolic complications.
Effects of TXA on blood loss
Across the included studies, TXA consistently demonstrated a reduction in perioperative blood loss, with randomized controlled trials in hip fracture surgery reporting decreases of roughly 20–40%, meta-analyses of orthopedic trauma procedures showing significant reductions in total blood loss compared with controls, and studies in pelvic and acetabular trauma also finding meaningful decreases in intraoperative bleeding; overall, these findings indicate that TXA provides a clinically relevant improvement in hemostasis across multiple fracture types.
Transfusion requirements
Most studies reported a substantial decrease in the requirement of blood transfusion among patients receiving TXA, with hip fracture trials showing 30–50% reductions in transfusion rates, observational studies in long bone fractures finding fewer units transfused per patient, and meta-analyses confirming that TXA significantly lowers transfusion risk across orthopedic trauma populations; this reduction is especially important in elderly and polytrauma patients, in whom transfusion-related complications are more common.
Safety outcomes
TXA demonstrated a favorable safety profile in the included studies, with randomized controlled trials and large cohort studies showing no significant increase in deep vein thrombosis or pulmonary embolism, meta-analyses likewise finding no elevated risk of thromboembolic events, and only infrequent, self-limiting minor adverse effects such as nausea or transient hypotension being reported; importantly, none of the included orthopedic trauma studies reported seizure events, which have been described only in high-dose cardiac surgery settings. Subgroup findings
Subgroup findings
Subgroup analyses across different fracture types revealed consistent benefits of TXA. In geriatric hip fracture surgery, TXA reduced blood loss and transfusion requirements, with early administration in the emergency department or before incision associated with improved perioperative stability and shorter hospital stays. In pelvic and acetabular trauma, although the evidence base is smaller, available studies support reductions in intraoperative bleeding and transfusion needs, though the optimal dosing strategy remains uncertain. In long bone fractures, including femoral and tibial surgeries, TXA was associated with lower perioperative blood loss, fewer transfusions in observational studies, and no increase in thromboembolic complications. The CRASH-2 trial demonstrated that administering TXA within 3 h of injury in polytrauma cases notably decreased mortality among patients with bleeding trauma, although the best dosing approach in cases involving concurrent head injury or massive transfusion protocols still requires further study.
Summary of studies
We can summarize that our review of the literature has determined that TXA reduces blood loss during surgery and transfusion requirements in orthopedic trauma cases. The effects or clinical results of TXA in orthopedic trauma are summarized in Table 1. Clinical studies supporting TXA use in orthopedic trauma are mentioned in Table 2.
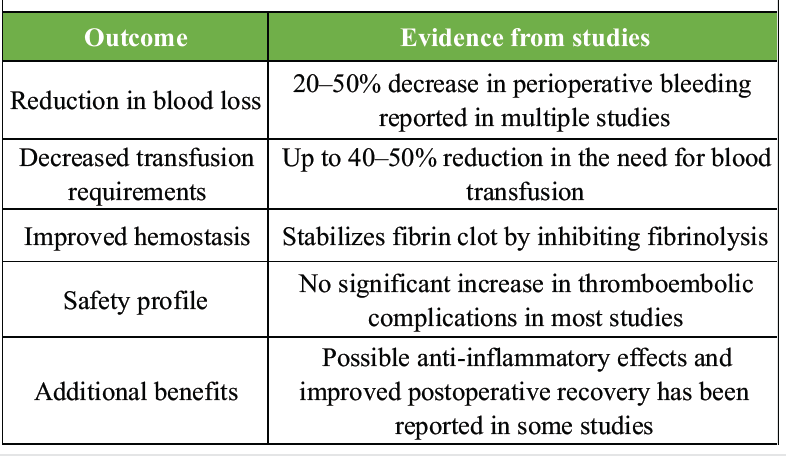
Table 1: Effects and outcomes of tranexamic acid in orthopedic trauma
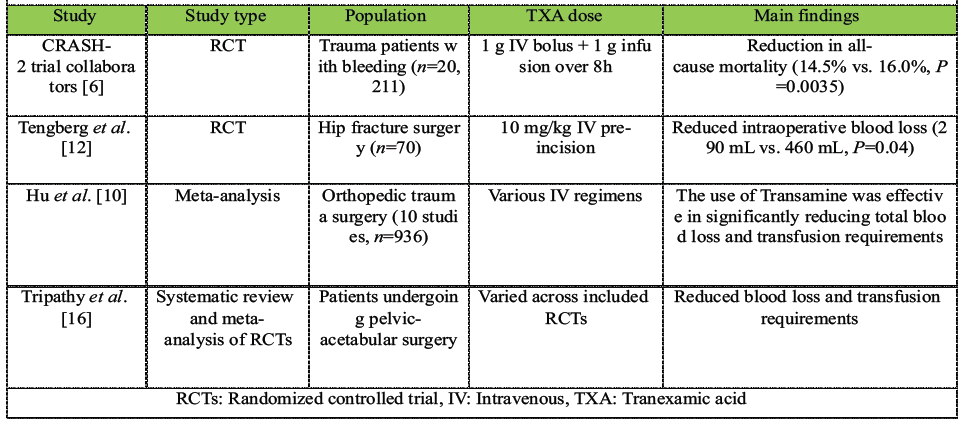
Table 2: Tranexamic acid in orthopedic trauma and clinical studies
These findings provide an important foundation for interpreting the clinical role of TXA in orthopedic trauma, which is explored in the following discussion.
This review evaluates the current studies on the use of TXA in orthopedic trauma and demonstrates a clear trend toward improved hemostatic control without an associated increase in thromboembolic complications. Based on this evidence, the practical use of TXA across different orthopedic trauma scenarios can be examined in greater detail.
TXA – clinical applications in orthopedic trauma
The use of TXA has been studied in numerous orthopedic trauma cases, such as hip fractures, pelvic and acetabular injuries, long bone fractures, and polytrauma cases [10,11]. Illustration summarizes a visual overview of TXA in orthopedic trauma, which is discussed in detail below (Fig. 4).
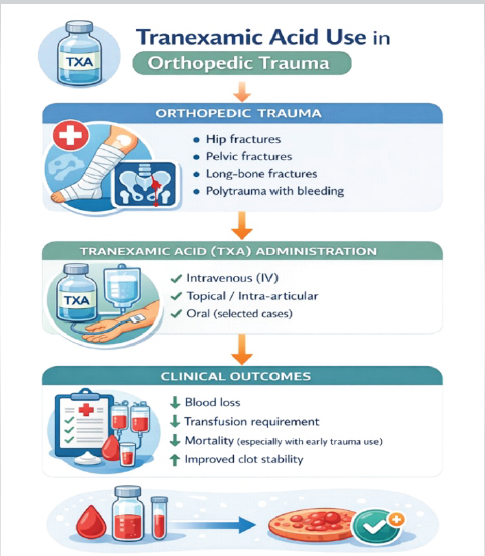
Figure 4: Tranexamic acid – Clinical application in orthopedic trauma.
Geriatric hip fractures
Geriatric hip fractures often require surgical fixation and are considered a major cause of morbidity. These patients frequently require blood transfusions because of perioperative blood loss. Numerous studies have been conducted on geriatric fractures in relation to TXA. Older patients are vulnerable to blood loss as they mostly have comorbid conditions such as anemia and cardiovascular diseases [12]. Multiple studies, such as randomized trials and meta analyses, show that TXA reduces perioperative blood loss and decreases transfusion requirements, often by 30–50%, in older adults undergoing hip fracture surgery [12,13]. Early administration of TXA in older patients in the emergency department or immediately before surgery has been documented with fewer post-operative complications and shorter hospital stays [14,15].
Pelvic and acetabular fractures Pelvic fractures are often caused by high-impact trauma such as road traffic accidents and falls from height, commonly present with retroperitoneal hemorrhage or pelvic collection which can be life threatening. The use of TXA in pelvic fractures has shown a decrease in intraoperative bleeding and blood transfusion requirements [16].
Long bone fractures Long bone fractures such as the femur and tibia are often associated with significant blood loss. Numerous studies support the use of TXA in isolated long bone trauma, with a decrease in perioperative blood loss and transfusion needs [1].
Polytrauma patients
Patients with polytrauma frequently present with multiple injuries and are hemodynamically unstable. TXA has been shown to decrease surgical bleeding and control traumainduced coagulopathy in these patients. In addition, the CRASH-2 trial has demonstrated the evidence that if TXA is administered within 3 h of injury, it significantly reduces mortality [6]. However, the optimal dosing in polytrauma, interactions with massive transfusion protocols, and its role in patients with concomitant traumatic brain injury remain uncertain and require further study [18]. While these clinical applications highlight the therapeutic value of TXA, its effectiveness also depends on appropriate dosing and route of administration.
Dosing strategies and routes of administration
TXA can be given through IV, topical, or oral routes. The preferred method of TXA administration in trauma patients is IV due to its rapid onset. In an actively bleeding patient, the CRASH-2 protocol, 1 g IV bolus followed by a 1 g infusion over 8 h, is widely accepted and used [6,7]. In orthopedic trauma surgery, there are significant variations in dosing practices across hospitals. Many hospitals prefer to practice weight based regimens ranging from 10 to 25 mg/kg, while others prefer fixed doses of 1–2 g for simplicity to reduce dosing errors. TXA may be administered as a single pre incision bolus, repeated intraoperatively, or given in multiple perioperative doses depending on defined hospital protocols. Unfortunately, despite widespread use, no consensus has been made on the optimal dose, timing, or route of administration for orthopedic trauma cases. Table 3 summarizes commonly practiced regimens [10,11].
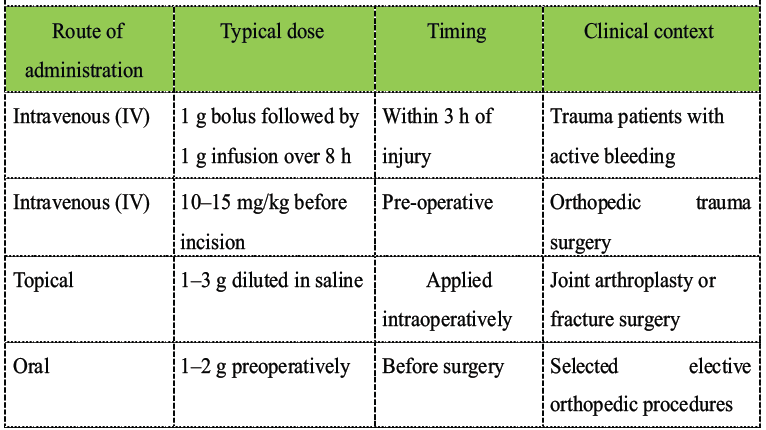
Table 3: Dosing strategies and routes of administration
In addition to dosing considerations, the safety profile of TXA remains a critical factor in determining its suitability for trauma patients.
Safety and complications
Overall, TXA has demonstrated a favorable safety profile across various surgical specialties [3,9]. Most clinical studies, including those in orthopedic trauma, have not reported a significant increase in thromboembolic incidents such as deep vein thrombosis or pulmonary embolism [10,11,13]. Common side effects such as nausea, vomiting, or transient hypotension with rapid IV injection may occur. Rare complications, such as seizures, have been reported with higher doses used in cardiac surgery than in orthopedic trauma [18]. Despite its generally favorable safety profile, several important uncertainties remain regarding the optimal use of TXA in orthopedic trauma.
Controversies, gaps, and future directions
Despite growing evidence in orthopedic trauma, several important questions remain, warranting further investigations [10].
• Dosing variability: Studies differ widely in dose, number of doses, and timing. Whether single dose or multi dose regimens are superior remains unclear. Current protocols vary widely, with studies reporting IV doses ranging from 10 to 25 mg/kg (as a single bolus or multiple doses) to fixed doses of 1–2 g. The optimal regimen whether a single pre-operative bolus is sufficient or a multi-dose protocol provides additional benefit remains unclear [9,10,11].
• Timing: Early administration is beneficial in bleeding trauma patients, but many orthopedic procedures occur hours or days after injury. The benefit of late dosing in trauma surgeries requires further study [15].
• High-risk populations: High-risk patients with prior venous thromboembolism, severe head injury, or those requiring massive transfusion are often excluded from trials. More inclusive studies are needed.
• Biological effects: Recent studies suggest that TXA may have anti inflammatory properties and potential effects on bone metabolism [5,11].
• Economic impact: TXA is inexpensive, and reductions in transfusion requirements may contribute to significant cost savings.
Recent studies have shown that TXA is safe and effective in reducing perioperative blood loss in orthopedic trauma cases. Its appropriate use can decrease the blood transfusion requirement in trauma patients and may be cost effective accordingly. Considerable variation remains in dosing strategies, timing of administration, and patient selection across different trauma settings. Additional high-quality, trauma specific studies are required to establish standardized protocols.
TXA is a safe and cost-effective adjunct that significantly reduces perioperative blood loss and transfusion requirements in orthopedic trauma surgeries. Early and appropriate use can improve patient outcomes across hip, pelvic, and long bone fractures, but standardized dosing and timing protocols are still needed.
References
- 1. Patil N, Saket R, Diwakar R, Reddy GH, Kumar KA, Sathe AM. Orthopedic trauma management: A comprehensive review of surgical interventions, rehabilitation, and patient outcomes. Cureus 2026;18:e104429. [Google Scholar] [PubMed]
- 2. Omondi MP. Epidemiology of orthopedic injuries among inpatients admitted at a tertiary teaching and referral hospital in Kenya: A retrospective cross-sectional study. BMC Musculoskelet Disord 2024;25:670. [Google Scholar] [PubMed]
- 3. Wang M, Zheng XF, Jiang LS. Efficacy and safety of antifibrinolytic agents in reducing perioperative blood loss and transfusion requirements in scoliosis surgery: A systematic review and meta-analysis. PLoS One 2015;10:e0137886. [Google Scholar] [PubMed]
- 4. Roberts I, Perel P, Prieto-Merino D, Shakur H, Coats T, Hunt BJ, et al. Effect of tranexamic acid on mortality in patients with traumatic bleeding: Prespecified analysis of data from randomised controlled trial. BMJ 2012;345:e5839. [Google Scholar] [PubMed]
- 5. Xie W, Donat A, Jiang S, Baranowsky A, Keller J. The emerging role of tranexamic acid and its principal target, plasminogen, in skeletal health. Acta Pharm Sin B 2024;14:2869-84. [Google Scholar] [PubMed]
- 6. CRASH-2 Trial Collaborators, Shakur H, Roberts I, Bautista R, Caballero J, Coats T, et al. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2): A randomised, placebo-controlled trial. Lancet 2010;376:23-32. [Google Scholar] [PubMed]
- 7. CRASH-2 Trial Collaborators, Roberts I, Shakur H, Afolabi A, Brohi K, Coats T, et al. The importance of early treatment with tranexamic acid in bleeding trauma patients: An exploratory analysis of the CRASH-2 randomised controlled trial. Lancet 2011;377:1096-101, 1101-e1-2. [Google Scholar] [PubMed]
- 8. Khan MW, Sahito B, Ali A, Siddiqui AA, Ahmed S, Ali T, et al. Safety and efficacy of tranexamic acid in hip hemiarthroplasty: A retrospective review of perioperative outcome. Medicine (Baltimore) 2025;104:e42711. [Google Scholar] [PubMed]
- 9. Borsinger TM, Chandi SK, Puri S, Debbi EM, Gausden EB, Chalmers BP. The efficacy and safety of tranexamic acid in total hip and knee arthroplasty: A literature review. HSS J 2024;20:10-7. [Google Scholar] [PubMed]
- 10. Hu M, Liu ZB, Bi G. Efficacy and safety of tranexamic acid in orthopaedic trauma surgery: A meta-analysis. Eur Rev Med Pharmacol Sci 2019;23:11025-31. [Google Scholar] [PubMed]
- 11. Gausden EB, Qudsi R, Boone MD, O’Gara B, Ruzbarsky JJ, Lorich DG. Tranexamic acid in orthopaedic trauma surgery: A meta-analysis. J Orthop Trauma 2017;31:513-9. [Google Scholar] [PubMed]
- 12. Tengberg PT, Foss NB, Palm H, Kallemose T, Troelsen A. Tranexamic acid reduces blood loss in patients with extracapsular fractures of the hip: Results of a randomised controlled trial. Bone Joint J 2016;98-B:747-53. [Google Scholar] [PubMed]
- 13. Zufferey PJ, Miquet M, Quenet S, Martin P, Adam P, Albaladejo P, et al. Tranexamic acid in hip fracture surgery: A randomized controlled trial. Br J Anaesth 2010;104:23-30. [Google Scholar] [PubMed]
- 14. Shah FA, Naeemullah, Ali MA, Iqbal MJ. Efficacy of preoperative tranexamic acid in patients undergoing intertrochanteric hip fracture surgery: A randomized placebo controlled trial. Pak J Med Sci 2023;39:1601-5. [Google Scholar] [PubMed]
- 15. Cheung ZB, Anthony SG, Forsh DA, Podolnick J, Zubizarreta N, Galatz LM, et al. Utilization, effectiveness, and safety of tranexamic acid use in hip fracture surgery: A population-based study. J Orthop 2020;20:167-72. [Google Scholar] [PubMed]
- 16. Tripathy SK, Khan S, Varghese P, Patel H, Mishra N, Jain M. Safety and efficacy of tranexamic acid in pelvi-acetabular trauma surgery: A systematic review and meta-analysis of randomized controlled trials. Eur J Orthop Surg Traumatol 2025;35:387. [Google Scholar] [PubMed]
- 17. Haghighi M, Ettehad H, Mardani-Kivi M, Mirbolook A, Nabi BN, Moghaddam R, et al. Does tranexamic acid reduce bleeding during femoral fracture operation? Arch Bone Jt Surg 2017;5:103-8. [Google Scholar] [PubMed]
- 18. Jennings JD, Solarz MK, Haydel C. Application of tranexamic acid in trauma and orthopedic surgery. Orthop Clin North Am 2016;47:137-43. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Efficacy of Tranexamic Acid in Reducing Blood Loss and Transfusion Requirements in Primary Total Knee Arthroplasty: A Prospective Comparative Study
June 1, 2026 Efficacy of Tranexamic Acid in Reducing Blood Loss and Transfusion Requirements in Primary Total Knee Arthroplasty: A Prospective Comparative Study June 1, 2025 Evaluation of Efficacy of Tranexamic Acid on Blood Loss in Surgically Managed Intertrochanteric Fractures
June 1, 2025 Evaluation of Efficacy of Tranexamic Acid on Blood Loss in Surgically Managed Intertrochanteric Fractures March 1, 2025 Does Multiple Intravenous Tranexamic Acid Doses in Patients Undergoing Total Knee Arthroplasty using Kinematic Alignment without Tourniquet Application show any Difference in Blood Loss, Transfusion Requirements and Hospital Stays: A Randomized Controlled Study
March 1, 2025 Does Multiple Intravenous Tranexamic Acid Doses in Patients Undergoing Total Knee Arthroplasty using Kinematic Alignment without Tourniquet Application show any Difference in Blood Loss, Transfusion Requirements and Hospital Stays: A Randomized Controlled Study April 10, 2024 Evaluating the Efficacy and Safety of Combined Administration of Systemic and Topical Tranexamic Acid in Total Knee Arthroplasty
April 10, 2024 Evaluating the Efficacy and Safety of Combined Administration of Systemic and Topical Tranexamic Acid in Total Knee Arthroplasty