
Intraosseous hydatid disease can masquerade as infected non-union, and early suspicion with staged management is crucial for optimal outcomes.
Dr. Sujeet Kumar Chaudhary, Department of Orthopaedics, King George’s Medical University, Lucknow, Uttar Pradesh, India. E-mail: skchaudhary404@gmail.com
Abstract
Introduction: Infected non-union of the subtrochanteric femur is commonly attributed to bacterial infection and mechanical instability; however, rare aetiologies may mimic this presentation and delay appropriate management. Hydatid disease involving bone is an uncommon manifestation and is often overlooked due to its non-specific clinical and radiological features. Reports of intraosseous hydatid cyst presenting as infected non-union are exceedingly rare, making this case clinically significant.
Case Report: A 32-year-old female of Indian origin presented with pain, inability to bear weight, and a discharging sinus over the proximal thigh 9 months following fixation of a subtrochanteric femur fracture. Clinical and radiological findings were suggestive of an infected non-union. During surgical debridement, multiple cystic structures were encountered within the bone, raising suspicion of an unusual pathology. Further evaluation revealed hydatid disease involving the liver. The patient was managed with a staged approach including debridement, stabilisation, antiparasitic therapy, and subsequent definitive reconstruction with total hip replacement. At follow-up, the patient showed good functional recovery without recurrence.
Conclusion: This case highlights a rare presentation of hydatid disease mimicking infected non-union, emphasising the importance of considering atypical aetiologies in endemic regions. It adds to the limited orthopaedic literature on osseous hydatidosis presenting as implant failure and underscores the role of intraoperative vigilance and multidisciplinary management. This report broadens the understanding of disease presentation and reinforces the need for tailored treatment strategies in complex non-unions.
Keywords: Hydatid cyst, osseous hydatidosis, femur, infected non-union, echinococcus granulosus.
Subtrochanteric femur fractures are biomechanically demanding injuries and are frequently complicated by delayed union or non-union, particularly in the presence of infection, poor fixation, or compromised biology. Infected non-union typically presents with pain, instability, and a discharging sinus and is most commonly attributed to bacterial osteomyelitis following prior surgical intervention [1]. However, atypical aetiologies may occasionally mimic this clinical picture, posing a diagnostic challenge and delaying definitive treatment. Hydatid disease, caused by Echinococcus granulosus, is an endemic parasitic infestation in many parts of the world, including India. It most commonly involves the liver (50–70%) and lungs (20–30%), while osseous involvement is rare, accounting for only 0.5–2% of cases [2,3]. Unlike soft-tissue hydatid cysts, osseous hydatidosis lacks a pericyst, allowing the parasite to proliferate along trabecular bone, leading to a slow, infiltrative pattern of destruction. Clinically, it often remains silent until advanced stages, presenting with pain, pathological fracture, or, rarely, features resembling chronic osteomyelitis [4]. A review of the literature reveals that intraosseous hydatid disease of the femur is exceedingly uncommon and frequently misdiagnosed preoperatively due to its non-specific clinical and radiological features [5,6]. Reports describing its presentation as infected non-union are particularly scarce. We report a rare case of subtrochanteric femoral non-union with sinus formation, where intraoperative findings and subsequent evaluation revealed underlying hydatid disease. This case emphasises the necessity of taking into account rare parasitic infections in the differential diagnosis of atypical non-unions, especially in endemic regions.
A 32-year-old female presented with complaints of persistent pain in the right hip and thigh, difficulty in weight-bearing, and a discharging sinus over the lateral aspect of the proximal thigh for the past 4 months. She had a history of trauma 9 months prior, for which she underwent closed reduction and internal fixation with Ender’s nails at another centre. The post-operative period was complicated by persistent pain and the gradual development of a sinus with seropurulent discharge. The patient had no history of fever, weight loss, or known comorbidities. On examination, there was tenderness over the proximal femur, abnormal mobility at the fracture site, and a discharging sinus over the lateral aspect of the thigh. Radiographs revealed a subtrochanteric femur fracture with features suggestive of infected non-union, along with an implant in situ and significant osteopenia. Laboratory investigations showed mildly elevated erythrocyte sedimentation rate and C-reactive protein levels. A staged surgical approach was planned. During the first stage, implant removal and thorough debridement were performed. Intraoperatively, multiple small cystic structures followed by a larger cystic sac were noted within the bone cavity, raising suspicion of an unusual pathology. The fracture was stabilised using an antibiotic-coated intramedullary nail. Further evaluation was undertaken. Ultrasonography of the abdomen revealed multiloculated cystic lesions in the right lobe of the liver with daughter cysts, suggestive of hydatid disease, which was confirmed on a contrast-enhanced computed tomography scan. The patient was started on oral albendazole (400 mg twice daily) for 3 weeks in consultation with general surgery. Following infection control and normalisation of inflammatory markers, the patient underwent definitive management after 6 months in the form of a cemented total hip replacement. At the 3-year follow-up, the patient was pain-free and ambulatory and showed no evidence of recurrence or infection (Fig. 1).
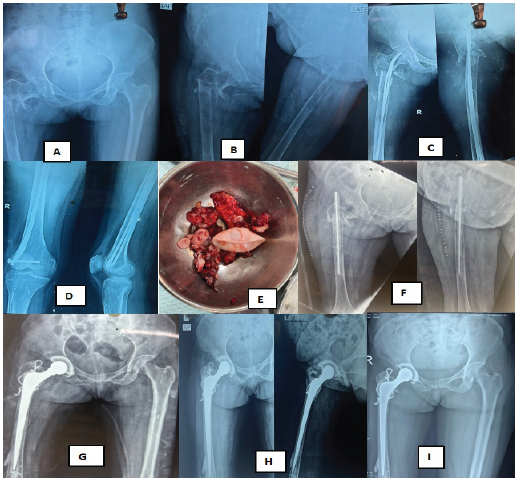
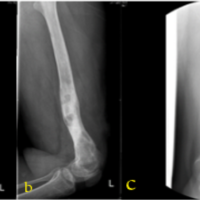
Figure 1: (a) Pre-operative radiograph showing subtrochanteric fracture of the right femur. (b) Follow-up radiograph demonstrating features of non-union with implant in situ. (c) Radiograph showing failed fixation with Ender’s nails and persistent fracture gap. (d) Distal femur radiograph depicting osteopenia and implant status. (e) Intraoperative photograph showing multiple cystic structures and membranous material suggestive of hydatid cyst retrieved from the bone cavity. (f) Immediate post-operative radiograph after first-stage procedure with antibiotic-coated intramedullary nail fixation. (g) Radiograph after second-stage surgery showing cemented total hip replacement at 9-month follow-up. (h) Follow-up radiographs demonstrating stable implant position with no evidence of loosening or recurrence at 2 years. (i) Follow-up radiographs demonstrating stable implant position with no evidence of loosening or recurrence at 3 years.
Osseous hydatid disease is a rare manifestation of Echinococcus granulosus infection and continues to pose a significant diagnostic and therapeutic challenge for orthopaedic surgeons. While hydatid disease predominantly involves the liver and lungs, skeletal involvement accounts for only 0.5–3% of all cases, with the femur being an uncommon site [2,3]. The rarity of bone involvement, combined with its indolent progression, often leads to delayed diagnosis and misinterpretation as chronic osteomyelitis, tumours, or infected non-union. Unlike soft-tissue hydatid cysts, osseous hydatidosis lacks a true pericyst, allowing the parasite to spread along trabecular channels in a diffuse and infiltrative pattern. This results in progressive bone destruction, cortical thinning, and eventual pathological fracture [7]. Radiological findings are non-specific, typically demonstrating multiloculated osteolytic lesions with a “honeycomb” appearance, which further contributes to diagnostic confusion. Consequently, diagnosis is frequently made intraoperatively or on histopathological examination, as seen in our case [8]. A review of the literature reveals that intraosseous hydatid disease of the femur is extremely rare, with only isolated case reports and small series available. Zlitni et al. reported the diagnostic difficulties and high recurrence rates associated with bone hydatidosis [6]. Similarly, Sapkas et al. emphasised its tendency to mimic chronic infections and delay definitive management [5]. Cases presenting with sinus formation and features resembling osteomyelitis have also been described, further highlighting its deceptive nature [9]. However, presentation as an infected non-union following prior fixation is exceedingly uncommon, making our case unique. Management of osseous hydatidosis remains challenging due to its infiltrative nature and difficulty in achieving complete eradication. A combined approach involving aggressive surgical debridement or resection along with antihelminthic therapy (albendazole or mebendazole) is recommended [10]. In advanced cases with extensive bone destruction, reconstructive procedures such as arthroplasty may be required. Despite adequate treatment, recurrence rates remain high, necessitating long-term follow-up. The peculiarity of our case lies in its presentation as an infected non-union with sinus formation following prior internal fixation, closely mimicking a routine orthopaedic complication. The intraoperative discovery of multiple cystic sacs was pivotal in establishing the diagnosis. In addition, the presence of concomitant hepatic hydatid disease highlights the importance of systemic evaluation in such atypical cases.
Take-home message:
Hydatid disease of bone, though rare, should be considered in the differential diagnosis of atypical infected non-unions, especially in endemic regions. A high index of suspicion and thorough evaluation can prevent misdiagnosis and guide appropriate staged management.
This case highlights a rare and deceptive presentation of intraosseous hydatid disease manifesting as an infected non-union of a subtrochanteric femur fracture following prior fixation. The clinical picture closely mimicked a routine orthopaedic complication, leading to an initial diagnostic dilemma. The intraoperative finding of multiple cystic sacs proved to be the key to diagnosis, later confirmed with systemic evaluation revealing concomitant hepatic involvement. The importance of this case lies in emphasising that not all infected non-unions are purely bacterial in origin, especially in endemic regions. It underlines the need for a high index of suspicion and careful intraoperative assessment when findings are atypical. Early recognition of such rare aetiologies can significantly alter management, necessitating a multidisciplinary approach combining surgical debridement, staged reconstruction, and anti-helminthic therapy. From an orthopaedic perspective, this case contributes to the limited literature on osseous hydatidosis presenting as implant failure and non-union, thereby expanding the differential diagnosis in complex cases. It also reinforces the role of staged management and definitive reconstruction in achieving favourable outcomes. Overall, this report has relevance not only to orthopaedic surgeons but also to general surgeons and infectious disease specialists, as it highlights the systemic nature of hydatid disease and its potential to masquerade as common musculoskeletal conditions.
Not all infected non-unions are bacterial – rare aetiologies like hydatid disease should be considered, especially in endemic regions or when intraoperative findings are atypical. Early suspicion and a multidisciplinary, staged approach can significantly alter management and improve outcomes.
References
- 1. Calori GM, Phillips M, Jeetle S, Tagliabue L, Giannoudis PV. Classification of non-union: Need for a new scoring system? Injury 2008;39 Suppl 2:S59-63. [Google Scholar] [PubMed]
- 2. Eckert J, Deplazes P. Biological, epidemiological, and clinical aspects of echinococcosis, a zoonosis of increasing concern. Clin Microbiol Rev 2004;17:107-35. [Google Scholar] [PubMed]
- 3. Turgut M. Hydatid disease of the spine: A survey study from Turkey. Infection 1997;25:221-6. [Google Scholar] [PubMed]
- 4. Neumayr A, Tamarozzi F, Goblirsch S, Blum J, Brunetti E. Spinal cystic echinococcosis – a systematic analysis and review of the literature: Part 1. Epidemiology and anatomy. PLoS Negl Trop Dis 2013;7:e2450. [Google Scholar] [PubMed]
- 5. Sapkas G, Stathakopoulos DP, Babis GC, Tsarouchas JK. Hydatid disease of bones and joints. Acta Orthop Belg 1998;64:223-9. [Google Scholar] [PubMed]
- 6. Zlitni M, Ezzaouia K, Lebib H, Karray M, Kooli M, Mestiri M. Hydatid cyst of bone: Diagnosis and treatment. World J Surg 2001;25:75-82. [Google Scholar] [PubMed]
- 7. Neumayr A, Tamarozzi F, Goblirsch S, Blum J, Brunetti E. Spinal cystic echinococcosis–a systematic analysis and review of the literature: Part 2. Treatment, follow-up and outcome. PLoS Negl Trop Dis. 2013;7:e2458. [Google Scholar] [PubMed]
- 8. García-Díez AI, Ros Mendoza LH, Villacampa VM, Cozar M, Fuertes MI. MRI evaluation of soft tissue hydatid disease. Eur Radiol 2000;10:462-6. [Google Scholar] [PubMed]
- 9. Dziri C, Haouet K, Fingerhut A. Treatment of hydatid cyst of the liver: Where is the evidence? World J Surg 2004;28:731-6. [Google Scholar] [PubMed]
- 10. Pedrosa I, Saíz A, Arrazola J, Ferreirós J, Pedrosa CS. Hydatid disease: Radiologic and pathologic features and complications. Radiographics 2000;20:795-817. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 June 10, 2022 Chronic Osteomyelitis Secondary to Hydatid Disease of Bone – A Case Report
June 10, 2022 Chronic Osteomyelitis Secondary to Hydatid Disease of Bone – A Case Report August 1, 2026 Management of Infected Non-union of Long Bones Using Antibiotic Cement-Coated Intramedullary Nails: A Prospective Case Series
August 1, 2026 Management of Infected Non-union of Long Bones Using Antibiotic Cement-Coated Intramedullary Nails: A Prospective Case Series May 1, 2026 Solitary Diaphyseal Langerhans Cell Histiocytosis of Femur in an Infant – A Case Report
May 1, 2026 Solitary Diaphyseal Langerhans Cell Histiocytosis of Femur in an Infant – A Case Report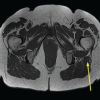 April 1, 2026 Incidental Intramedullary Lipoma of the Proximal Femur Detected Following Trauma: A Case Report
April 1, 2026 Incidental Intramedullary Lipoma of the Proximal Femur Detected Following Trauma: A Case Report