
Oblique Close Wedge versus Modified Step Cut Osteotomy for Cubitus Varus Deformity in Children: A Prospective Non-Randomized Study
Dr Udit Sourav Sahoo, Department of Orthopaedics, SCB Medical College, Cuttack, Odisha, India. E-mail: uditsouravsahoo@gmail.com
Abstract
Introduction: Cubitus varus is a delayed complication of neglected supracondylar humerus fractures in children. Both oblique closing-wedge and modified step-cut osteotomies are widely used corrective techniques, but prospective comparative data are limited.
Materials and Methods: In this prospective non-randomised comparative study, 30 patients with cubitus varus deformity were divided into two groups: Oblique closing-wedge osteotomy (Group 1, n = 15) and modified step-cut osteotomy (Group 2, n = 15). Radiological correction was assessed using carrying angle, and functional outcomes were evaluated using elbow flexion-extension arc, pronation-supination arc, and Mayo elbow performance score (MEPS). Radiological union time was recorded. Statistical analysis was performed using an independent t-test and chi-square test.
Results: The mean age was 14.9 ± 2.7 years, with comparable baseline characteristics between groups (P = 0.741). Both groups showed significant deformity correction, with mean post-operative carrying angles of 13.0° ± 4.9° and 11.5° ± 5.6°, respectively (P = 0.432). The mean MEPS was 88.0 ± 7.8 in Group 1 and 90.0 ± 8.7 in Group 2 (P = 0.511). Elbow flexion extension arc, prono-supination arc, and union time were similar between groups (P > 0.05). Both the osteotomies achieved radiological union. The mean follow-up duration was 14.2 ± 2.8 months.
Conclusion: Both oblique closing-wedge and modified step-cut osteotomies provide effective correction of cubitus varus with comparable radiological and functional outcomes. Both techniques are safe and reliable options in children.
Keywords: Cubitus varus, corrective osteotomy, step-cut osteotomy, closing-wedge osteotomy, pediatric elbow.
Cubitus varus deformity is the most common delayed complication of malunited supracondylar fractures of the humerus in children [1,2]. Conventionally, it is considered a cosmetic deformity, but at the skeletal level, it involves a complex three-dimensional malalignment consisting of varus, internal rotation, and extension deformity [3]. In the long run, cubitus varus leads to functional limitations, tardy ulnar nerve palsy, posterolateral rotatory instability of the elbow, secondary lateral condyle fractures, and psychological distress [4,5,6]. Various types of corrective distal humeral osteotomy are the treatment of choice for symptomatic or cosmetically unacceptable cubitus varus deformity [2,7]. Numerous techniques have been described, including lateral closing-wedge, dome, step-cut, pentolateral, and three-dimensional osteotomies [8,9,10]. Among these, the lateral closing-wedge osteotomy continues to be the most commonly performed technique because relatively simple preoperative planning is required to correct the coronal plane deformity [2,11]. However, conventional lateral closing-wedge osteotomy has certain specific complications such as lateral condylar prominence, loss of fixation, and suboptimal cosmetic outcome [1,11]. Several modifications have been proposed in the literature. Oblique lateral closing-wedge osteotomy is one such technique, which alters the orientation of the osteotomy cut to reduce lateral condyle prominence [12]. The modified step-cut osteotomy is another technique that was developed to improve intrinsic stability by providing an interlocking configuration of bone and also reducing the lateral condyle prominence [13,14]. Most of the existing literature suggests that satisfactory outcomes can be achieved with both these techniques; however, the majority are retrospective case series [10]. There is a lack of comparative studies for the evaluation of these two techniques. This prospective non-randomised comparative study aims to compare the functional, radiological, and cosmetic outcomes of both these techniques.
This prospective non-randomised comparative study was undertaken at a tertiary care level 1 trauma centre from July 2021 to December 2025, after obtaining institutional ethics committee approval (IEC 612, dated June 25, 2021) and informed consent from the participants. Children aged ≤15 years with post-traumatic cubitus varus deformity secondary to malunited supracondylar humeral fractures were included. Children with congenital deformities, previous corrective surgery, neuromuscular disorders, infection, or associated ipsilateral limb fractures were excluded. Patients were allocated into two groups based on the surgical technique used: Group A underwent oblique lateral closing-wedge osteotomy, and Group B underwent modified step-cut osteotomy. Allocation was non-randomised, performed on consecutive children, and largely based on the surgeon’s preference. Pre-operative evaluation included clinical assessment of the carrying angle (humerus–elbow–wrist angle), elbow range of motion, and standard anteroposterior and lateral radiographs of both elbows for deformity assessment and surgical planning. All procedures were performed under general anaesthesia through a posterior approach by a total of five different orthopaedic surgeons. In Group A, an oblique lateral closing-wedge osteotomy was performed with preservation of the medial cortex. In Group B, a modified step-cut osteotomy was carried out. Fixation was achieved using plates for the lateral side and cancellous screws for the medial side. Intraoperative correction was confirmed fluoroscopically. We administered 2 days of intravenous antibiotics and 5 more days of post-operative oral antibiotics. Postoperatively, the limb was immobilised in an above-elbow slab for 3–4 weeks, followed by gradual mobilisation. Physiotherapy protocols were standardised and objectively monitored across all patients by a single team of physiotherapists. Children were followed up at 3-monthly intervals for a minimum duration of 12 months. Outcomes assessed were carrying angle, elbow range of motion, radiological correction, cosmetic appearance, functional outcome, and complications. Evaluation was done by a team of orthopaedic surgeons in addition to the five operating surgeons in the outpatient department. Statistical analysis was performed using the Statistical Package for the Social Sciences software, with P < 0.05 considered statistically significant. Analysis of the results between the two groups was done by the chi-square test for categorical data, the independent t-test for normally distributed data, and the Mann–Whitney test for the parameters where data were not normally distributed. Normality of data distribution was tested using the Shapiro–Wilk test.
A total of 30 children with post-traumatic cubitus varus deformity were included in the study, with 15 patients each in Group 1 (oblique lateral closing-wedge osteotomy) and Group 2 (modified step-cut osteotomy). All patients were available for final analysis with a mean follow-up duration of 14.2 ± 2.8 months (range, 12–20 months). The mean duration of surgery was comparable between Group 1 and Group 2 (62.4 ± 8.6 vs. 64.1 ± 9.2 min; P = 0.618). Similarly, the mean number of fluoroscopy shots required (21.3 ± 2.4 vs. 24.8 ± 2.7; P = 0.594) was not significantly different between the groups. Mean intraoperative blood loss (1–2 blood-soaked medium-sized gauzes in both the groups) and implant-related expenditure were also comparable between the groups. Results are summarised in Table 1.
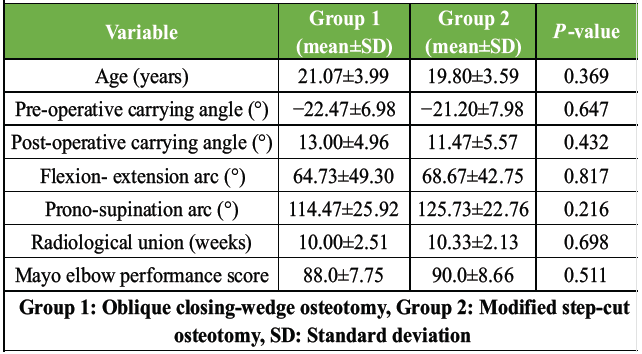
Table 1: Statistical comparison between the groups
Demographic data:
The mean age of the study population was 14.9 ± 2.7 years (range, 11–19 years). The mean age in Group 1 was 14.7 years and in Group 2 was 15.1 years (P = 0.741). There were 19 males (64.5%) and 11 female children in the study. The right side was involved in 20 (67%) of cases, with a similar distribution between the groups. There was no statistically significant difference between the two groups in terms of age (P = 0.741), gender distribution (P = 1.000), or side involved (P = 0.699), indicating that the groups were comparable at the baseline.
Radiological outcomes:
The mean pre-operative carrying angle for the entire cohort was −21.8° ± 7.4° (range, −35–−10°). There was no statistically significant difference between the two groups in terms of pre-operative carrying angle (P = 0.647). Postoperatively, this improved to a mean of 12.2° ± 5.2° (range, 5–20°), indicating satisfactory correction in both groups. Group 1 showed improvement from −22.5° ± 7.0° pre-operatively to 13.0° ± 5.0° post-operatively, while Group 2 improved from −21.2° ± 8.0° to 11.5° ± 5.6°. The magnitude of correction was comparable between the two groups, with a P = 0.432. Radiological union was achieved in all patients. The mean time to union was 10.2 ± 2.3 weeks overall, with Group 1 uniting at 10.0 ± 2.5 weeks and Group 2 at 10.3 ± 2.1 weeks, with a P = 0.698.
Functional outcomes:
At final follow-up, the mean elbow flexion-extension arc for the entire cohort was 66.7° ± 45.4°. Group 1 demonstrated a mean elbow flexion extension arc of 64.7° ± 49.3°, while Group 2 demonstrated 68.7° ± 42.8°, P = 0.817. Forearm rotation was well preserved in both groups, with a mean prono-supination arc of 120.1° ± 24.6° overall (Group 1: 114.5° ± 25.9°; Group 2: 125.7° ± 22.8°, P = 0.216). The mean Mayo Elbow Performance Score was 88.0 ± 7.8 in Group 1 and 90.0 ± 8.7 in Group 2. The difference between the two groups was not statistically significant (P = 0.511). Figs 1 and 2 represent one case each from group 1 and group 2, respectively.

Figure 1: (a) Pre-operative clinical picture demonstrates cubitus varus (gunstock deformity). (b) Both elbow anteroposterior radiographs. (c) Oblique osteotomy done through the posterior approach to the elbow and provisional fixation with K-wires while the medial cortical hinge is preserved. (d) Post-operative radiography showing lateral column fixation with a locking plate and medial column fixed with 2 number of 4.0 mm CC screw without any undue lateral prominence. (e) Post-operative immobilization on an above-elbow slab, (f) Post-operative correction of coronal alignment. (g) 6-month post-operative radiograph showing union of osteotomy site and corrected coronal alignment.

Figure 2: (a) Pre-operative clinical picture demonstrates cubitus varus (gunstock deformity). (b) Left elbow anteroposterior radiograph. (c) Modified step-cut osteotomy done through posterior approach to the elbow. (d) Intraoperative fluoroscopy image showing provisional fixation with K wires while medial cortical hinge is preserved. (e) Post-operative radiography showing lateral column fixation with a locking plate and medial column fixed with a 3.5 mm cortical screw without any undue lateral prominence. (f) Follow-up X-ray radiograph showing union at 2 months, (g) 3-month follow-up clinical picture showing correction of coronal alignment in the extended elbow. (h) 3-month follow-up clinical picture showing near-normal elbow flexion.
Complications:
A total of 5 cases of heterotopic ossification were seen, 2 in group 1 and 3 in group 2. Patients responded to oral indomethacin. No cases of lateral condyle prominence, non-union, loss of correction, or neurovascular injury were observed in either group. Cosmetic appearance was satisfactory in both groups.
Cubitus varus deformity following supracondylar humeral fractures is a three-dimensional deformity, and the corrective surgery is challenging in the paediatric population [3,4]. Previously, it was regarded as a benign cosmetic condition; however, subsequent studies have revealed that it might lead to elbow instability, ulnar nerve palsy, and late functional impairment, emphasising the need for accurate deformity correction [4,5,6]. The present study focused on a comparative analysis between oblique lateral closing-wedge osteotomy and modified step-cut osteotomy, which suggested that both techniques are equally effective for improvement in carrying angle, satisfactory elbow function, and predictable bony union. These findings are consistent with previous studies that have reported good outcomes with corrective osteotomy [2,7,11]. Lateral closing-wedge osteotomy remains the most frequently reported corrective procedure in the literature [2,11]. Bellemore et al. and French have demonstrated predictable angular correction using this technique but noted lateral condylar prominence as the cosmetic concern amongst parents of the children [1,11]. Oblique modification of the closing-wedge osteotomy was introduced to minimise this lateral prominence. This obliquity of the osteotomy plane produces a controlled translation along with rotation of the distal fragment in the coronal plane, thus reducing lateral prominence [12]. There are a few reports of improved cosmetic outcomes and maintained stability with this modification, findings that are supported by the satisfactory results in our study [12,15]. The modified step-cut osteotomy has also been advocated as an alternative technique. The idea is to further improve cosmetic appearance and fixation stability. This technique increases the surface area of bone contact and creates an interlocking osteotomy geometry, which gives inherent stability and reduces the risk of loss of angular correction and lateral prominence [13,14]. Bali et al. and Kim et al. reported high rates of excellent and good outcomes with minimal complications using the step-cut osteotomy technique, findings of which are comparable to our study [13,14]. Solfelt et al. in their systematic review have analysed more than 900 paediatric cases of cubitus varus with the conclusion that no single osteotomy technique showed any clear superiority and that results were more driven by the surgical planning and execution rather than by the specific osteotomy design [10]. This observation aligns with our results, where both oblique closing-wedge and modified step-cut osteotomies produced comparable functional and radiological outcomes. The limitations of this study include its non-randomised design, possible selection bias and relatively smaller sample size of only 30 patients, which may limit the statistical strength and generalisability of the findings. A total of 5 different orthopaedic surgeons performed the procedures, and differences in surgical expertise and technical execution might have influenced the outcome. Rotational and sagittal plane deformity corrections were not quantitatively assessed, and only the degree of coronal plane deformity correction was considered. Follow-up duration was relatively short, with a mean follow-up of 14.2 months, which may not be sufficient to detect long-term complications like recurrence of deformity or tardy ulnar nerve palsy and rare complications like avascular necrosis or osteoarthritis. Nevertheless, the prospective design and direct comparison of the two most commonly employed techniques provide clinically relevant data for further research to guide surgical decision-making. A multi-centre randomised controlled study comparing both the techniques with a larger sample size is required to consolidate our findings and increase the applicability of the results to other healthcare settings and populations.
Both oblique lateral closing-wedge osteotomy and modified step-cut osteotomy provided reliable correction of cubitus varus deformity with comparable radiological union and functional outcomes in our study.
Both osteotomy techniques were clinically safe, achieved predictable union and corrected alignment, allowing surgeons to choose based on familiarity and intraoperative feasibility. Emphasis should be placed on accurate pre-operative planning, stable fixation, and early pain-free mobilisation to optimise functional recovery and cosmetic outcome.
References
- 1. French PR. Varus deformity of the elbow following supracondylar fractures of the humerus in children. Lancet 1959;2:439-41. [Google Scholar] [PubMed]
- 2. Amspacher JC, Messenbaugh JK. Supracondylar osteotomy of the humerus for correction of cubitus varus. J Bone Joint Surg Am 1964;46:1245-58. [Google Scholar] [PubMed]
- 3. Takeyasu Y, Murase T, Miyake J, Oka K, Arimitsu S, Moritomo H, Sugamoto K, Yoshikawa H. Three-dimensional analysis of cubitus varus deformity after supracondylar fractures of the humerus. J Shoulder Elbow Surg. 2011 Apr;20(3):440-8. [Google Scholar] [PubMed]
- 4. Jeon IH, Oh CW, Kyung HS, Park IH, Kim PT. Tardy ulnar nerve palsy in cubitus varus deformity associated with ulnar nerve dislocation in adults. J Shoulder Elbow Surg. 2006 Jul-Aug;15(4):474-8. [Google Scholar] [PubMed]
- 5. Abe M, Ishizu T, Shirai H, Okamoto M, Onomura T. Tardy ulnar nerve palsy caused by cubitus varus deformity. J Hand Surg Br 1995;20:5-9. [Google Scholar] [PubMed]
- 6. Oppenheim WL, Clader TJ, Smith C, Bayer M. Supracondylar humeral osteotomy for traumatic childhood cubitus varus deformity. Clin Orthop Relat Res 1984;188:34-9. [Google Scholar] [PubMed]
- 7. DeRosa GP, Graziano GP. A new osteotomy for cubitus varus. Clin Orthop Relat Res 1988;236:160-5. [Google Scholar] [PubMed]
- 8. Laupattarakasem W, Mahaisavariya B, Kowsuwon W, Saengnipanthkul S. Pentalateral osteotomy for cubitus varus. Clinical experiences of a new technique. J Bone Joint Surg Br 1989;71:667-70. [Google Scholar] [PubMed]
- 9. Chung MS, Baek GH. Three-dimensional corrective osteotomy for cubitus varus. Clin Orthop Relat Res 2003;416:191-7. [Google Scholar] [PubMed]
- 10. Solfelt DA, Hill BW, Anderson CP, Cole PA. Surgical correction of cubitus varus: A systematic review. J Pediatr Orthop 2014;34:697-703. [Google Scholar] [PubMed]
- 11. Bellemore MC, Barrett IR, Middleton RW, Scougall JS, Whiteway DW. Supracondylar osteotomy of the humerus for correction of cubitus varus. J Bone Joint Surg Br 1984;66:566-72. [Google Scholar] [PubMed]
- 12. Greenhill DA, Kozin SH, Kwon M, Herman MJ. Oblique Lateral Closing-Wedge Osteotomy for Cubitus Varus in Skeletally Immature Patients. JBJS Essent Surg Tech. 2019 Nov 1;9(4):e40.1-8. [Google Scholar] [PubMed]
- 13. Bali K, Sudesh P, Krishnan V, Sharma A, Manoharan SR, Mootha AK. Modified step-cut osteotomy for post-traumatic cubitus varus: our experience with 14 children. Orthop Traumatol Surg Res. 2011 Nov;97(7):741-9. [Google Scholar] [PubMed]
- 14. Kim HT, Lee JS, Yoo CI. Management of cubitus varus deformity by step-cut osteotomy. Clin Orthop Relat Res 2005;434:166-72. [Google Scholar] [PubMed]
- 15. Su Y, Xie Y & Nan G. A novel method of lateral closing wedge osteotomy for cubitus varus deformity in children. BMC Surg 2022;22:408. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2025 Evaluating Outcomes of Step-Cut Osteotomy for Pediatric Cubitus Deformities
January 1, 2025 Evaluating Outcomes of Step-Cut Osteotomy for Pediatric Cubitus Deformities June 1, 2026 Isolated Coronoid Process Fracture in a 7-Year-Old Child – A Case Report
June 1, 2026 Isolated Coronoid Process Fracture in a 7-Year-Old Child – A Case Report May 1, 2026 Oblique Lateral Closing-Wedge Osteotomy for Cubitus Varus in Skeletally Immature Children: A Case Series
May 1, 2026 Oblique Lateral Closing-Wedge Osteotomy for Cubitus Varus in Skeletally Immature Children: A Case Series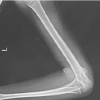 January 1, 2026 A Case Report: Post-traumatic Windswept Deformity of the Elbow – Rare but Possible
January 1, 2026 A Case Report: Post-traumatic Windswept Deformity of the Elbow – Rare but Possible