
The coronoid process was stabilized with a mini-anchor in a pediatric patient.
Dr. Braulio Henrique Magnani Branco, Cesumar University, Maringa, Parana, Brazil. E-mail: braulio.branco@unicesumar.edu.br
Abstract
Introduction: Coronoid process fractures in children are rare and infrequently reported in the literature; they are typically associated with posterior elbow dislocations.
Case Report: We report a case of an isolated coronoid process fracture in a 7-year-old male child, treated surgically with open reduction and internal fixation of a Regan and Morrey Type II fracture, using a mini-anchor and high-resistance suture cerclage. The patient was followed for 21 months postoperatively.
Conclusion: This therapeutic approach proved to be effective for coronoid process fractures in pediatric patients who have not yet achieved complete ossification.
Keywords: Coronoid process fracture, mini-anchor fixation, pediatric elbow.
The coronoid process of the ulna plays a critical role in elbow stability and serves as the insertion point of the brachialis muscle. In paediatric patients, it is primarily composed of cartilage. Coronoid fractures in children are rare and are typically seen in association with posterior elbow dislocations or as avulsion injuries of the brachialis muscle during elbow hyperextension events [1,2,3,4]. According to Henrikson, coronoid process fractures occur in approximately 3% of elbow dislocations in the paediatric population [5]; the overall incidence of elbow dislocations in this age group is also considered low, estimated at about 6 cases/100,000 children/year [6]. This study presents a case of an isolated fracture of the elbow’s coronoid process. Understanding the treatment approach requires knowledge of the Regan and Morrey classification, which defines coronoid fractures into three types. Type I: Small fragments not involving the articular surface; Type II: Larger fragments involving up to 50% of the process; Type III: fragments involving more than 50%. Type I fractures are generally managed conservatively, while Type II and III fractures usually require internal fixation to preserve elbow flexion [7].
A 7-year-old male patient sustained a fall from standing height, presenting with pain, swelling, and functional impairment of the right elbow. Initial elbow radiography revealed a coronoid process fracture without dislocation (Fig. 1).
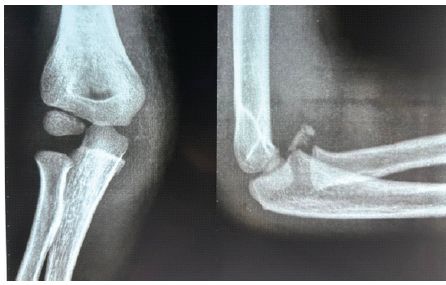
Figure 1: Pre-operative radiograph with anteroposterior and lateral views.
A subsequent tomography scan confirmed the fracture (Fig. 2).

Figure 2: Pre-operative 3D reconstruction computed tomography scan confirming a fracture of the coronoid process.
Surgical treatment was indicated due to the risk of flexion block (Regan and Morrey Type II) [1]. The procedure was performed under general anaesthesia and a right brachial plexus block. An anterior approach to the elbow was employed, using a “boat-race” incision between the brachial artery and median nerve to access the fracture. Intraoperatively, the fragment appeared larger than on radiographs due to its predominantly cartilaginous composition. Minimal fixation was chosen, using a mini-anchor inserted into the ulna and high-resistance suture cerclage to secure the fragment (Fig. 3).
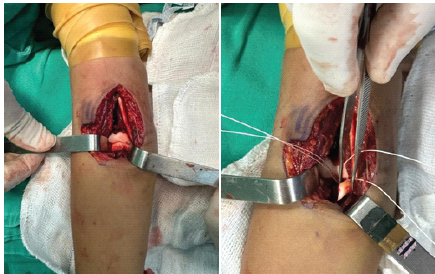
Figure 3: Intraoperative.
Layered closure was performed following meticulous haemostasis. The elbow was immobilised with a brachiopalmar splint. At 1 week postoperatively, wound dressing and a control radiograph were performed. The patient was asymptomatic, and imaging demonstrated adequate reduction and fixation (Fig. 4).
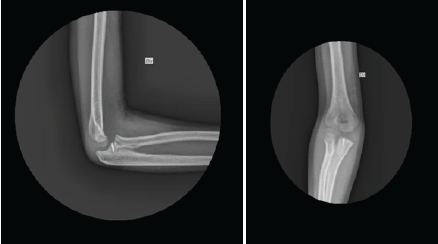
Figure 4: Radiograph at 1 week postoperatively.
No signs of infection were observed. Sutures were removed at 2 weeks, and the splint was maintained for 4 weeks postoperatively. After that, the patient was referred to elbow physiotherapy for range-of-motion recovery. Two months after surgery, the patient had completed eight physiotherapy sessions and remained pain-free. Goniometric assessment showed full extension (0°) and flexion limited to 130° (20° deficit). Imaging confirmed fracture consolidation. At 8 months, the patient returned with full elbow range of motion and normal function, with imaging confirming consolidation and an anatomically reduced joint. At 21 months, follow-up imaging again confirmed complete healing and reduction (Fig. 5), and goniometric evaluation showed a preserved range of motion (−10° extension to 150° flexion) (Fig. 6).
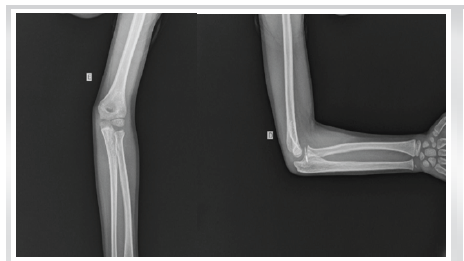
Figure 5: Radiograph at 21 months postoperatively.

Figure 6: Full range of motion at 21 months postoperatively.
Coronoid process fractures in children are rarely encountered due to their cartilaginous structure, often resulting in misdiagnosis or missed diagnosis [7,8]. Intraoperatively, the fracture fragment was noted to be much larger than radiographically evident, owing to the cartilaginous nature of the epiphyseal coronoid process [2]. In our case, the patient presented with an isolated coronoid process fracture following a fall onto an outstretched hand. Surgical treatment with minimal fixation was performed, and the patient was followed for 18 months, demonstrating complete healing, full range of motion (ROM), and preserved elbow function. In the case reported by Khodnapur et al., a 9-year-old male sustained a Regan and Morrey Type III fracture after a similar mechanism of injury. The patient underwent open reduction and internal fixation with Herbert screws, and a 1-year follow-up showed full ROM and a stable elbow joint [7]. Gadgil et al. described a case of a 40-month-old female with a Type II coronoid fracture in which the anterior band of the medial collateral ligament avulsed the coronoid fragment. The patient underwent surgical repair using non-absorbable periosteal sutures and fully recovered elbow motion and stability [9,10].
Based on our case outcome and a review of the literature, open reduction and internal fixation appear to be an effective approach for paediatric type II coronoid process fractures, supporting the conclusions of Regan and Morrey, Selesnick et al., and Hanks and Kottmeier. No postoperative joint instability or neurovascular complications were observed.
Early diagnosis, appropriate physical examination, open fixation treatment, and long-term postoperative follow-up are critical for the successful management of paediatric type II coronoid process fractures.
References
- 1. Regan W, Morrey BF. Classification and treatment of coronoid process fractures. Orthopedics 1992;15:845-8. [Google Scholar] [PubMed]
- 2. Chambers H, Garza JF, O’Brien E, Price CT, Stanley E, Wilkins KE. Fractures of the radius and ulna. In: Rockwood CA Jr., Wilkins KE, Beaty JH, editors. Rockwood and Green’s Fractures in Children. 4th ed. Philadelphia, PA: Lippincott-Raven; 1996. [Google Scholar] [PubMed]
- 3. Selesnick FH, Dolitsky B, Haskell SS. Fracture of the coronoid process requiring open reduction with internal fixation. A case report. J Bone Joint Surg Am 1984;66:1304-6. [Google Scholar] [PubMed]
- 4. Lamberti AG, Lőrincz A, Molnár T, Kassai T, Nudelman H, Józsa G. Surgical management of pediatric coronoid process fractures: A report of two cases. Life (Basel) 2025;15:614. [Google Scholar] [PubMed]
- 5. Henrikson B. Supracondylar fracture of the humerus in children. A late review of end-results with special reference to the cause of deformity, disability and complications. Acta Chir Scand Suppl 1966;369:1-72. [Google Scholar] [PubMed]
- 6. Hyvönen H, Korhonen L, Hannonen J, Serlo W, Sinikumpu JJ. Recent trends in children’s elbow dislocation with or without a concomitant fracture. BMC Musculoskelet Disord 2019;20:294. [Google Scholar] [PubMed]
- 7. Khodnapur G, Desai N, Khatri R. Isolated coronoid fracture in a 9-year old child – a case report. J Orthop Case Rep 2023;13:5-8. [Google Scholar] [PubMed]
- 8. Syn CJ, Aziz AA, Raghunandanan S, Kamaludin NA, Mohd Termizi NS. Pediatric olecranon fracture with coronoid process osteochondral flap fracture: A rare and challenging case. J Southeast Asian Orthop 2024;48:36-9. [Google Scholar] [PubMed]
- 9. Gadgil A, Roach R, Neal N, Maffulli N. Fracture avulsion isolée de l’apophyse coronoïde de l’ulna imposant une réduction à ciel ouvert chez l’enfant. Acta Orthop Belg 2002;68:396-8. [Google Scholar] [PubMed]
- 10. Hanks GA, Kottmeier SA. Isolated fracture of the coronoid process of the ulna: A case report and review of the literature. J Orthop Trauma 1990;4:193-6. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Oblique Close Wedge versus Modified Step Cut Osteotomy for Cubitus Varus Deformity in Children: A Prospective Non-Randomized Study
June 1, 2026 Oblique Close Wedge versus Modified Step Cut Osteotomy for Cubitus Varus Deformity in Children: A Prospective Non-Randomized Study December 1, 2024 Displaced Jeffery Type 2 Radial Neck Fracture Managed by a Modified Métaizeau Technique: A Case Report
December 1, 2024 Displaced Jeffery Type 2 Radial Neck Fracture Managed by a Modified Métaizeau Technique: A Case Report October 1, 2024 Terrible Triad Injuries around the Elbow: It is Still a Puzzle? Prospective Study
October 1, 2024 Terrible Triad Injuries around the Elbow: It is Still a Puzzle? Prospective Study March 10, 2024 Discoid Double-layered Lateral Meniscus: A Case Report
March 10, 2024 Discoid Double-layered Lateral Meniscus: A Case Report