
Despite the rarity of the association of the injuries presented in this case report, thorough examination has to be done when receiving a trauma patient in order not to miss the diagnosis.
Dr. Abdullah Zaher, Department of Orthopedics and Traumatology, Saint Denis Hospital Center, Delafontaine Hospital, Saint Denis, France. E-mail: abdullah.zaher@ch-stdenis.fr
Abstract
Introduction: Although the Galeazzi fracture-dislocation is an uncommon forearm fracture in adults, scaphoid fracture is not a rare finding. Even though both injuries may result from the same mechanism, there is only one report in the literature describing a simultaneous Galeazzi fracture and ipsilateral scaphoid fracture.
Case Report: We report here the case of a 22-year-old male who presented to our emergency department with bilateral wrist trauma following a road traffic accident on his motorcycle. The patient was diagnosed with a Galeazzi fracture dislocation associated with an ipsilateral scaphoid fracture in addition to a contralateral distal radius fracture. He underwent bilateral open reduction and internal fixation.
Conclusion: It's a rare finding; clinicians must keep in mind the fracture mechanics and accordingly perform the proper examination in order not to miss the diagnosis.
Keywords: Galeazzi fracture-dislocation, scaphoid fracture, wrist trauma, open reduction internal fixation, distal radioulnar joint instability.
The Galeazzi fracture dislocation involves a fracture of the distal third of the radial shaft with the involvement of the distal radioulnar joint (DRUJ). This fracture type accounts for <10% of adult forearm fractures. The most common mechanism of injury typically involves a fall onto an outstretched hand with the wrist in pronation or supination [1,2,3,4]. On the other side, scaphoid fractures are the most common carpal bone fracture (60%); they make up 15% of acute wrist injuries, often occurring after a fall onto an outstretched hand with the wrist in pronation and radial deviation [5,6]. Although both fractures have similar mechanisms of injury, the fact that both fractures occur simultaneously on the same limb has not been previously described except once [7]. The following case report details a case of simultaneous Galeazzi fracture dislocation and ipsilateral scaphoid fracture in a 22-year-old man who underwent surgical treatment.
While driving his motorcycle back home from work at 90 km/h, a previously healthy 22-year-old man was hit by a car that was travelling at 50 km/h. The patient landed on both wrists. He was brought to our emergency department with no history of loss of consciousness or vital life-threatening injuries, yet with deformed wrists. He initially had radiographs showing a pronation-type Galeazzi fracture dislocation classified as type 1 according to the Rettig-Raskin classification, a displaced fracture of the right scaphoid, and a displaced fracture of the left distal radius. Pre-operative evaluation was completed with a computed tomography (CT) scan, which showed a comminuted displaced Mayo type 3 fracture of the right scaphoid besides a comminuted extra-articular fracture of the left distal radius (Figs. 1 and 2).
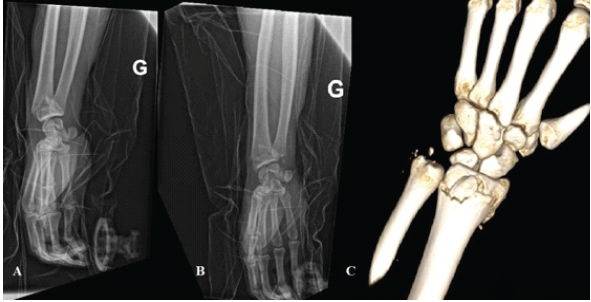
Figure 1: Pre-operative radiography of the left wrist (a) approximate lateral view, (b) approximate anteroposterior view, (c) 3D reconstruction.
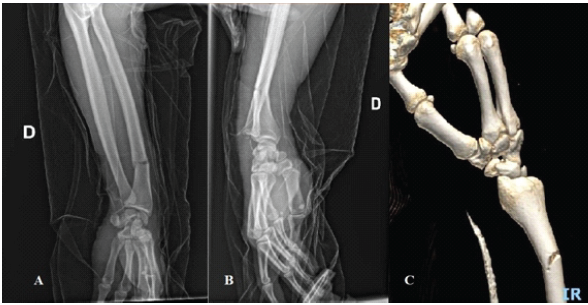
Figure 2: Pre-operative radiography of the right wrist (a) approximate anteroposterior view, (b) lateral view, (c) 3D reconstruction.
The patient’s fractures were stabilised with posterior splints, and he was admitted to our ward to prepare him for the operating room the next day. The next morning the patient was taken to the operating room, where he had general anaesthesia and was given prophylactic antibiotics. The patient underwent simultaneous surgeries on both upper limbs by two teams. Simple open reduction and internal fixation of the left distal radius with a locking plate and screws were done (Fig. 3).

Figure 3: Final intraoperative radiographic image of left wrist.
On the right side, the fracture site was exposed through a standard Henry anterior approach. The reduction did not cause any particular difficulties as it was maintained with a reduction clamp before the insertion of a T-shaped compression plate fixed with three screws on each side of the fracture site. The dynamic testing of the stability of the DRUJ revealed instability, for which DRUJ fixation was performed using an 18-mm pin. Then, a palmar scaphoid approach was done with proximal extension toward the radial diaphysis. Dissection was made to the level of the radiocarpal ligaments, which were incised in a triangular fashion and marked with a tagging suture. After its identification, the fracture site was curetted after placing two vertical pins on each side to facilitate their separation. A reduction with a joystick was performed, followed by fixation of the reduction with a temporary pin. A trans-scaphoid guide pin was then inserted, and a 20 mm cannulated screw was placed to fix the fracture (Fig. 4).
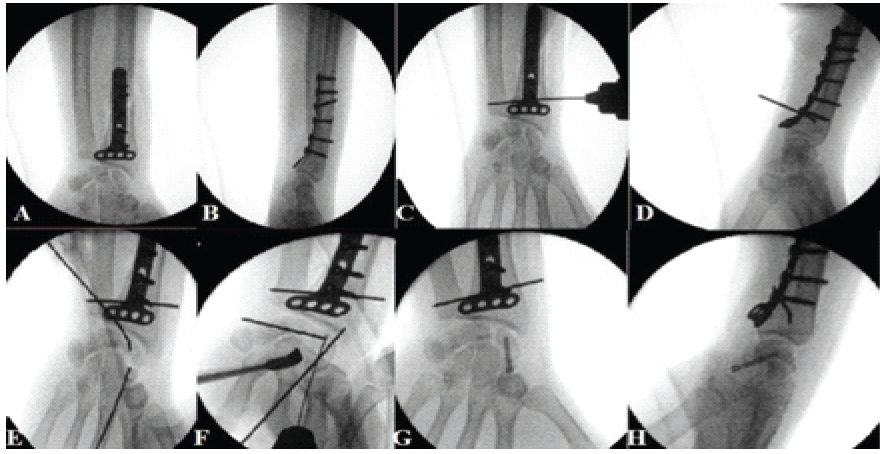
Figure 4: Intraoperative radiographic images of the right wrist (a) Anteroposterior view with radial fracture fixed by a plate, (b) Lateral view with radial fracture fixed by a plate, (c) Anteroposterior view with the introduction of radioulnar pin fixing the DRUJ, (d) Lateral view with the radioulnar pin fixing the DRUJ, (e) Anteroposterior view showing joysticking to reduce scaphoid fracture, (f) Temporary fixation of scaphoid using a pin, (g) Anteroposterior view showing a screw fixing the scaphoid fracture, (h) Lateral view showing a screw fixing the scaphoid fracture. DRUJ: Distal radioulnar joint.
Ligament reattachment was then performed. The left side was immobilised with a splint, and the right side was cast in a long cast (Figs. 5 and 6).
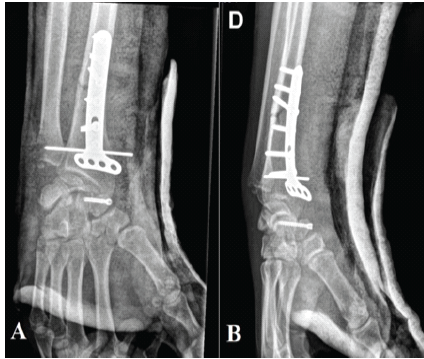
Figure 5: One-month post-operative X-rays of the right wrist.
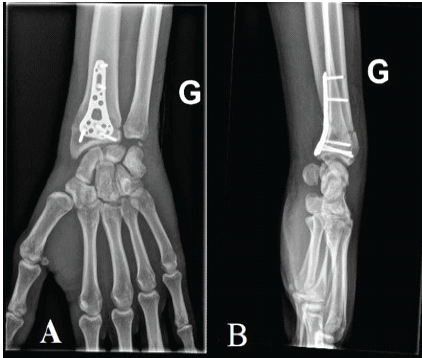
Figure 6: One-month post-operative X-rays of the left wrist.
The patient underwent reoperation 6 weeks later to remove the DRUJ pin. The post-operative course was uneventful, with no complications observed. The patient underwent several progressive physical therapy sessions, beginning with passive range of motion exercises and gradually progressing to active range of motion exercises. During the follow-up period, the patient showed satisfactory healing and a progressive increase in wrist mobility and strength on both sides, ultimately reaching a functional range of motion suitable for daily activities. The functional results were similar to those generally seen in patients who have undergone surgical intervention for Galeazzi fractures, with no signs of pain, instability, or delayed healing. A post-operative follow-up was performed over a span of 4 months, after which the continuity of care was handed over due to the patient’s relocation to another country. At 4 months postoperatively, he was pain-free and had regained a full range of motion in both wrists.
The Galeazzi fracture is considered a rare injury; therefore, the Galeazzi fracture and the ipsilateral scaphoid fracture are even rarer. The coexistence of an ipsilateral scaphoid fracture with a Galeazzi fracture represents an exceedingly rare injury pattern. While both Galeazzi fractures and isolated scaphoid fractures are well-documented, their occurrence together suggests a complex mechanism at play. To our knowledge, there has been only one recorded case of this kind in the literature, underscoring the uniqueness of this presentation. Stahl and Frieman mentioned this case of a Galeazzi fracture associated with an ipsilateral scaphoid fracture in 1999 [7]. The rarity may also be due to underdiagnosis, particularly of the scaphoid component, which might be ignored in the presence of a clear forearm deformity. The mechanism of injury of the Galeazzi typically involves direct dorsolateral trauma to the wrist or, more commonly, a fall onto an outstretched arm with the wrist pronated or supinated. It is reported that the forces pass through the radioulnar joint, producing displacement and shortening of the radial shaft. As the displacement continues, dislocation of the ulnar head occurs with tearing of the triangular fibrocartilage, which then loses its stabilising influence on the wrist [3]. In addition, these forces can be transmitted further into the wrist, causing associated injuries. Taylor and Shakespeare in 1998 reported a trapezoid dislocation and a Galeazzi fracture in a 28-year-old man who was treated surgically [8]. On the other hand, the transmission of forces and trauma energy can go proximally. In 2018, Lee et al. described a combined ipsilateral humeral shaft and Galeazzi fracture producing a floating elbow [9]. Previously, Sarup and Bryant described the mechanism of injury in an ipsilateral humeral shaft fracture and a Galeazzi fracture with elbow dislocation. They reported that the extreme axial load exerted by an outstretched hand with the elbow fully extended and the forearm pronated, with the patient’s body weight, can result in a Galeazzi fracture. The collapse of the radial pillar will cause this force to be transmitted through the soft tissues and ulna to the extended elbow, resulting in elbow dislocation [10]. Further collapse and hyperextension caused by the body weight will fracture the humerus [9]. Regarding scaphoid fractures, these are the second most common type of wrist fractures after the distal radius fractures; their most common mechanism of injury is a fall on an extended or hyperextended wrist, which is also often radially displaced [6]. Simultaneous fractures of the distal radius and scaphoid are rare. This is a very small group of upper extremity injuries. Publications on these combined injuries are rare. The reported incidence ranges from 0.7% to 6.5% of all distal radius fractures. The mechanism of injury follows the same principle of energy transfer [6]. Therefore, the likely mechanism of injury in the case presented was a high-velocity fall onto an outstretched hand combined with a hyperpronated forearm and a fully extended wrist. The extreme axial load from the impact with the ground could have caused a scaphoid fracture with the wrist extended and the forearm pronated, resulting in a dislocation of the DRUJ and, successively, a radius fracture. Other than the article by Stahl and Freiman [7], there have been no previous reports of a Galeazzi fracture and an ipsilateral scaphoid fracture. From a surgical perspective, this specific combination of injuries poses distinct challenges during the operation. A key hurdle is balancing fixation priorities without jeopardising the alignment of either fracture. The instability associated with the DRUJ in Galeazzi fractures requires meticulous restoration of radial length, alignment, and rotation, whereas the scaphoid fracture requires precise reduction to reduce the chances of non-union or avascular necrosis. Another challenge is the possibility of conflicting biomechanical requirements during fixation. Radial stabilisation may have an indirect effect on carpal alignment, whereas manipulating for scaphoid fixation may have an impact on DRUJ stability. As a result, intraoperative examination of wrist and forearm stability at each step is crucial. Fluoroscopic guidance is critical in ensuring appropriate reduction and hardware placement for both fractures, as well as monitoring DRUJ congruency after fixation. A methodical, stepwise surgical strategy can effectively tackle these challenges. Initially, comprehensive pre-operative planning and imaging analysis should be conducted to understand the fracture’s characteristics; in our case, a CT scan with 3D reconstruction was utilised. Next, the patient had to be positioned to allow simultaneous access to the wrist and forearm; in our situation, the concurrent positioning of the other wrist, which was being operated on by a different team simultaneously, was crucial for minimising operation time. Subsequently, the fixation of the radial shaft fracture was carried out first to restore the radial anatomy. Then, intraoperative evaluation of the DRUJ’s stability revealed instability, prompting temporary fixation by pinning. Afterward, utilising the extension of the Henry approach to access the scaphoid, the fracture was aligned and secured with a cannulated compression screw under fluoroscopic guidance. Finally, a reassessment of wrist motion, scaphoid alignment, and DRUJ stability was performed before closure.
When evaluating a patient with a Galeazzi fracture, associated injuries, whether bony or soft tissue, should not be overlooked. Therefore, careful history taking and physical examination should be realised before requesting directed paraclinical examinations. We report here a very rare case of ipsilateral scaphoid and Galeazzi fracture. This unusual atypical association has not been described in the literature because of its rarity. The combination of Galeazzi and ipsilateral scaphoid fracture is probably the result of a high-energy trauma causing a compression load on the forearm and wrist during the fall on the outstretched hand. Further biomechanical studies are needed to determine the exact energy transmission mechanism responsible for this type of simultaneous fracture. Awareness of potential intraoperative challenges and adherence to a stepwise approach are crucial to achieving optimal functional outcomes and minimising complications.
References
- 1. Nanno M, Sawaizumi T, Takai S. A case of bilateral Galeazzi fractures associated with dislocation of the right elbow. J Nippon Med Sch 2011;78:384-7. [Google Scholar] [PubMed]
- 2. Zaher A, Marzak I, Sekkach N. Bilateral pronation type Galeazzi fracture dislocation. Cureus 2024;16:e64552. [Google Scholar] [PubMed]
- 3. Garg R, Mudgal C. Galeazzi injuries. Hand Clin 2020;36:455-62. [Google Scholar] [PubMed]
- 4. Giannoulis FS, Sotereanos DG. Galeazzi fractures and dislocations. Hand Clin 2007;23:153-63. [Google Scholar] [PubMed]
- 5. Berdia S, Wolfe SW. Effects of scaphoid fractures on the biomechanics of the wrist. Hand Clin 2001;17:533-40, vii-viii. [Google Scholar] [PubMed]
- 6. Slutsky D, Osterman L. Fractures and injuries of the distal radius and carpus. In: The Cutting Edge. 1st ed. Netherlands: Saunders Elsevier Publication; 2009. [Google Scholar] [PubMed]
- 7. Stahl S, Freiman S. Simultaneous scaphoid and Galeazzi fractures. Hand Surg 1999;4:185-8. [Google Scholar] [PubMed]
- 8. Taylor M, Shakespeare D. Trapezoid dislocation with a Galeazzi fracture. Acta Orthop Belg 1998;64:328-30. [Google Scholar] [PubMed]
- 9. Lee P, Piatek AZ, DeRogatis MJ, Issack PS. Combined ipsilateral humeral shaft and galeazzi fractures creating a floating elbow variant. Case Rep Orthop 2018;2018:7430297. [Google Scholar] [PubMed]
- 10. Sarup S, Bryant PA. Ipsilateral humeral shaft and Galeazzi fractures with a posterolateral dislocation of the elbow: A variant of the “floating dislocated elbow”. J Trauma 1997;43:349-52. [Google Scholar] [PubMed]
This rare injury pattern requires a high index of suspicion. Thorough examination, careful surgical planning, and a structured operative sequence are essential for the proper management of a trauma patient with multiple fractures. Even in the case of rare conditions, proper examination will help prevent missing diagnoses.
References
- 1. Nanno M, Sawaizumi T, Takai S. A case of bilateral Galeazzi fractures associated with dislocation of the right elbow. J Nippon Med Sch 2011;78:384-7. [Google Scholar] [PubMed]
- 2. Zaher A, Marzak I, Sekkach N. Bilateral pronation type Galeazzi fracture dislocation. Cureus 2024;16:e64552. [Google Scholar] [PubMed]
- 3. Garg R, Mudgal C. Galeazzi injuries. Hand Clin 2020;36:455-62. [Google Scholar] [PubMed]
- 4. Giannoulis FS, Sotereanos DG. Galeazzi fractures and dislocations. Hand Clin 2007;23:153-63. [Google Scholar] [PubMed]
- 5. Berdia S, Wolfe SW. Effects of scaphoid fractures on the biomechanics of the wrist. Hand Clin 2001;17:533-40, vii-viii. [Google Scholar] [PubMed]
- 6. Slutsky D, Osterman L. Fractures and injuries of the distal radius and carpus. In: The Cutting Edge. 1st ed. Netherlands: Saunders Elsevier Publication; 2009. [Google Scholar] [PubMed]
- 7. Stahl S, Freiman S. Simultaneous scaphoid and Galeazzi fractures. Hand Surg 1999;4:185-8. [Google Scholar] [PubMed]
- 8. Taylor M, Shakespeare D. Trapezoid dislocation with a Galeazzi fracture. Acta Orthop Belg 1998;64:328-30. [Google Scholar] [PubMed]
- 9. Lee P, Piatek AZ, DeRogatis MJ, Issack PS. Combined ipsilateral humeral shaft and galeazzi fractures creating a floating elbow variant. Case Rep Orthop 2018;2018:7430297. [Google Scholar] [PubMed]
- 10. Sarup S, Bryant PA. Ipsilateral humeral shaft and Galeazzi fractures with a posterolateral dislocation of the elbow: A variant of the “floating dislocated elbow”. J Trauma 1997;43:349-52. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Acute Capitellum Fracture with Distal Radio-ulnar Joint Disruption: An Atypical Variant of an Essex Lopresti Injury – Case Report
June 1, 2026 Acute Capitellum Fracture with Distal Radio-ulnar Joint Disruption: An Atypical Variant of an Essex Lopresti Injury – Case Report April 1, 2026 Modified Posterior Approach for Scapular Body Non-union: A Case Report
April 1, 2026 Modified Posterior Approach for Scapular Body Non-union: A Case Report October 1, 2025 Surgical Treatment of a Non-union of Medial End Clavicle Fracture with Dual Plating and its Clinical Outcome – A Case Report
October 1, 2025 Surgical Treatment of a Non-union of Medial End Clavicle Fracture with Dual Plating and its Clinical Outcome – A Case Report June 1, 2025 Successful Management of Atypical Bilateral Galeazzi Fractures with Unique Dorsal Displacement: A Case Report
June 1, 2025 Successful Management of Atypical Bilateral Galeazzi Fractures with Unique Dorsal Displacement: A Case Report