
Combined Mechanical and Biological Salvage of Recalcitrant Subtrochanteric Non-union using Valgus Osteotomy, Blade Plate Fixation, and Endomedullary Fibular Graft
Dr. Roberto Federico Herrera, Hospital Interzonal General de Agudos Dr. Luis Güemes, Haedo, Buenos Aires, Argentina. E-mail: dr.herrera.roberto@gmail.com
Abstract
Introduction: Subtrochanteric femoral non-union after failed fixation is a demanding reconstructive problem because of high mechanical loads on the proximal femur and impaired bone biology following repeated surgery. Persistent varus deformity, loss of medial support, and implant failure frequently lead to recurrent non-union. Valgus correction converts shear forces into compressive forces across the non-union site, and structural fibular grafting can provide additional biological and mechanical support in complex proximal femoral reconstruction.
Case Report: A 62-year-old male presented with recalcitrant subtrochanteric femoral non-union, implant breakage, and progressive varus deformity after three previous failed surgical procedures. He underwent a salvage procedure combining a lateral closing wedge valgus osteotomy, fixed-angle 110° blade plate fixation, and endomedullary structural fibular autografting through the existing cephalomedullary nail tract. The fibular graft restored an intramedullary biological and structural strut opposing residual varus deforming forces. Complete radiographic union was achieved at 9 months, and the patient remained pain-free and fully weight-bearing at 3-year follow-up, with no implant failure or recurrence of non-union.
Conclusion: Combined valgus closing osteotomy, fixed-angle blade plate fixation, and endomedullary structural fibular grafting can provide reliable mechanical stability and biological support, achieving successful salvage of recalcitrant subtrochanteric non-union after multiple failed prior procedures.
Keywords: Subtrochanteric non-union, valgus osteotomy, blade plate, structural fibular graft, revision surgery, proximal femur.
Subtrochanteric femoral non-union remains one of the most demanding reconstructive scenarios in trauma surgery due to the high mechanical stresses acting on the proximal femur and the biological impairment frequently associated with multiple previous procedures [1,2,3,4]. Persistent varus deformity, implant failure, loss of medial support, and compromised bone biology frequently result in recurrent non-union and mechanical failure [5,6,7]. Valgus correction improves the biomechanical environment by converting shear forces into compression forces across the non-union site [4,8]. In addition, structural fibular grafting may provide biological augmentation and increased construct stability in complex proximal femoral reconstruction [9,10,11]. The purpose of this report is to describe a salvage strategy combining valgus osteotomy, blade plate fixation, and endomedullary structural fibular grafting for the treatment of recalcitrant subtrochanteric non-union.
A 62-year-old male was referred to our institution after failure of three previous surgical procedures performed for a subtrochanteric femoral fracture sustained in a motorcycle accident. The patient presented with persistent pain, progressive varus deformity, inability to fully weight-bear, and implant failure following previous cephalomedullary fixation associated with lateral cortical allograft struts (Fig. 1).
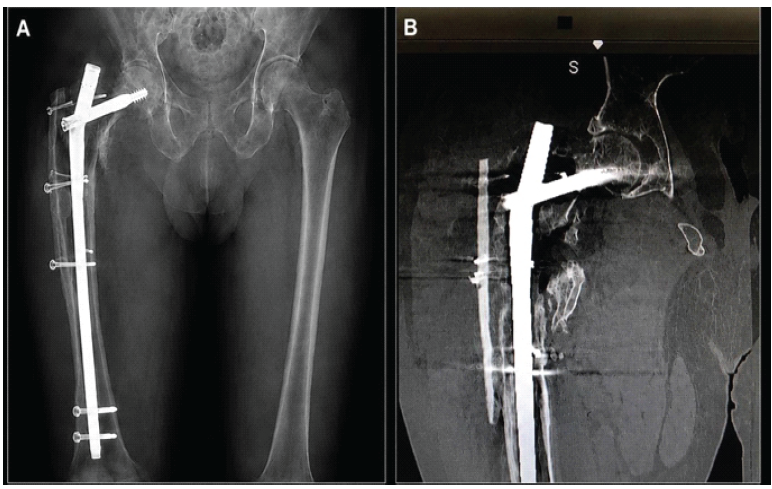
Figure 1: Pre-operative evaluation. (a) Anteroposterior radiographs demonstrating recalcitrant subtrochanteric non-union with previous cephalomedullary fixation failure and varus deformity, (b) Coronal computed tomography scan showing extensive bone loss, cortical discontinuity, sclerosis, and medullary canal obliteration around the non-union site.
Radiographs demonstrated recalcitrant subtrochanteric non-union with implant breakage, loss of medial support, residual varus alignment, and sclerosis at the non-union site. Pre-operative infection workup included laboratory analysis, aspiration, and cultures, which were all negative. No clinical signs of local infection were identified. Pre-operative planning focused on restoration of the cervicodiaphyseal angle and correction of the persistent varus deformity. The planned strategy combined valgus correction, fixed-angle blade plate fixation, and structural endomedullary fibular grafting using the previous cephalomedullary nail tract as a mechanically favourable intramedullary pathway.
Surgical technique:
The pre-operative surgical plan is illustrated in Fig. 2. The patient was positioned in lateral decubitus on a radiolucent table (Fig. 3).
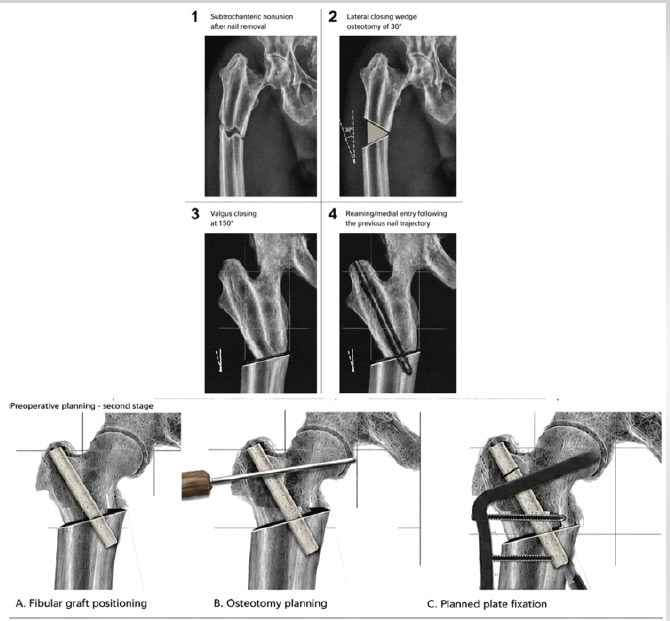
Figure 2: Step-by-step schematic representation of the surgical technique.

Figure 3: Patient positioning on a radiolucent table with pre-operative skin markings.
Across an extended lateral approach using the previous incision, all failed hardware and cortical allograft struts were removed. Extensive debridement and decortication of the non-union site were performed until viable bleeding bone was identified. Simultaneously, a second surgical team harvested an ipsilateral structural fibular autograft using a standard technique. According to pre-operative planning, a lateral closing wedge osteotomy of approximately 30° was performed at the non-union site to restore valgus alignment and increase the cervicodiaphyseal angle to approximately 150°. The osteotomy was progressively closed using pointed reduction clamps, temporary non-locking screws, and Jungbluth reduction forceps until restoration of alignment and correction of the varus deformity were achieved. Subsequently, the previous cephalomedullary nail tract was reamed using a 13-mm trochanteric reamer following the trajectory of the previous implant and creating a linear intramedullary pathway directed toward the distal medial cortex beyond the non-union site.
The structural fibular graft was then impacted into the prepared canal, creating a biological and structural intramedullary support aligned perpendicular to persistent varus deforming forces. The graft was additionally secured using Kirschner wires or screws when required (Fig. 4).
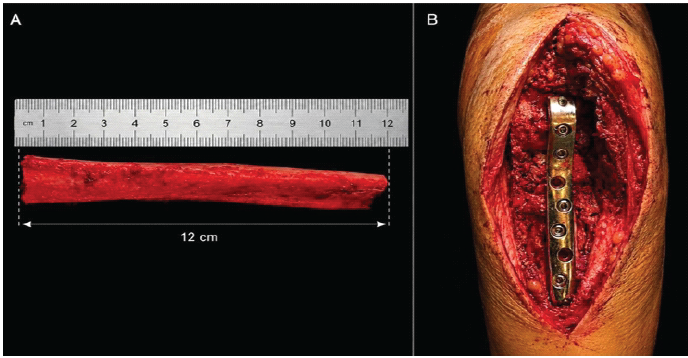
Figure 4: Intraoperative images. (a) Structural fibular autograft, 12 cm in length, (b) Definitive blade plate fixation in situ.
Blade plate osteotomy preparation was subsequently performed according to the standard technique. During blade advancement, the proximal remnant of the fibular graft progressively approximated and mechanically interfered with blade passage. Therefore, the graft was carefully impacted against the proximal femur until a controlled fracture of the proximal fibular remnant occurred, allowing complete blade seating while maintaining distal structural support. Definitive fixation was achieved using a 110° blade plate, restoring alignment, stability, and length.
No intraoperative or post-operative complications occurred. Progressive radiographic healing was observed during follow-up, with complete union achieved at 9 months (Fig. 5). At final follow-up 3 years post-operatively, the patient was pain-free, fully weight-bearing, and demonstrated no evidence of implant failure or recurrent non-union (Fig. 6).
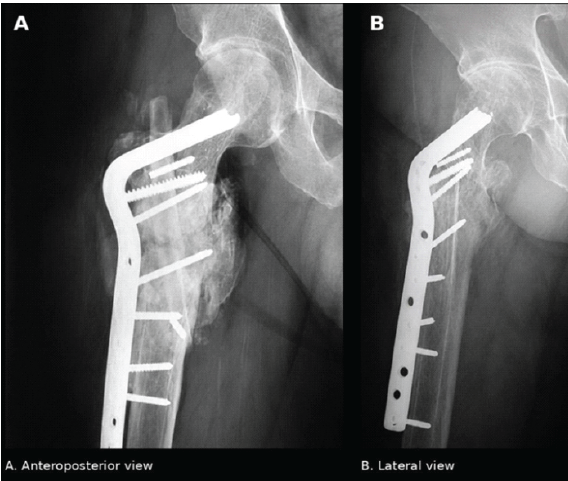
Figure 5: Immediate post-operative control radiographs. (a) Anteroposterior view, (b) Lateral view.
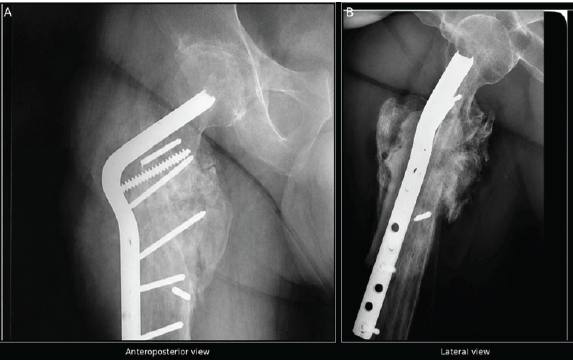
Figure 6: Nine-month post-operative radiographic control showing consolidation, (a) Anteroposterior view, (b) Lateral view.
The management of recalcitrant subtrochanteric non-union remains challenging because of the coexistence of mechanical instability and biological impairment [2,3,4,5,6]. Persistent varus alignment increases shear stress across the non-union site and predisposes to implant failure. In the present case, valgus correction improved the biomechanical environment, while the structural fibular graft provided additional endomedullary support and increased construct stability [8,9,10,11]. The combination of blade plate fixation, valgus osteotomy, and endomedullary fibular support represented the key factor for successful healing. This technique may represent a valuable salvage option in selected proximal femoral non-union cases following multiple failed procedures. Successful treatment of complex proximal femoral non-union requires simultaneous restoration of mechanical alignment and biological environment rather than isolated implant revision. The limitation of this report is that it represents a single case; however, the technique may be useful in selected salvage scenarios. The previous cephalomedullary nail tract was strategically reused to create a mechanically favourable intramedullary pathway for fibular graft impaction, allowing the graft to function as a structural biological strut opposing persistent varus deforming forces. Rather than serving solely as a biological augmentation, the fibular graft acted as a load-sharing intramedullary support integrated with the valgus correction.
Valgus closing osteotomy associated with fixed-angle blade plate fixation and endomedullary structural fibular grafting provided successful salvage of a recalcitrant subtrochanteric non-union after multiple failed surgeries. This strategy may represent a reproducible alternative in complex proximal femoral reconstruction.
Recalcitrant subtrochanteric non-union after failed fixation should be addressed by simultaneously correcting mechanical alignment and restoring biological support, rather than by isolated hardware revision. Converting varus deformity to valgus through a closing wedge osteotomy transforms shear into compressive forces at the non-union site, while fixed-angle blade plate fixation provides a stable mechanical construct independent of medial cortical contact. Reusing the existing cephalomedullary nail tract as a guide for endomedullary structural fibular grafting offers a practical, reproducible pathway for delivering a load-sharing biological strut without the need for additional bone stock. When approached together, these three elements – mechanical realignment, rigid fixation, and structural biological augmentation – offer a viable salvage strategy even after multiple prior failed procedures.
References
- 1. Rollo G, Tartaglia N, Falzarano G, Pichierri P, Stasi A, Medici A, et al. The challenge of non-union in subtrochanteric fractures with breakage of intramedullary nails: How to prevent and treat it? Injury 2017;48 Suppl 3:S27-33. [Google Scholar] [PubMed]
- 2. Vicenti G, Solarino G, Bizzoca D, Simone F, Maccagnano G, Zavattini G, et al. Use of the 95-degree angled blade plate with biological and mechanical augmentation to treat proximal femoral non-unions: A case series. J Orthop Surg Res 2022;17:72. [Google Scholar] [PubMed]
- 3. Lotzien S, Rausch V, Schildhauer TA, Gessmann J. Revision of subtrochanteric femoral nonunions after intramedullary nailing with dynamic condylar screw. BMC Musculoskelet Disord 2018;19:448. [Google Scholar] [PubMed]
- 4. El-Alfy B, Abououf A, Darweash A, Fawzy S. The effect of valgus reduction on resistant subtrochanteric nonunion. Eur J Orthop Surg Traumatol 2024;34:1021-9. [Google Scholar] [PubMed]
- 5. Lawrenz JM, Marshall DC, Patterson BM. The utility of the angled blade plate in hip fracture nonunion treatment. Strategies Trauma Limb Reconstr 2019;14:93-8. [Google Scholar] [PubMed]
- 6. Haidukewych GJ, Berry DJ. Salvage of failed internal fixation of intertrochanteric hip fractures. J Am Acad Orthop Surg 2005;13:101-9. [Google Scholar] [PubMed]
- 7. De Vries JS, Kloen P, Borens O, Marti RK, Helfet DL. Treatment of subtrochanteric nonunions. Injury 2006;37:203-11. [Google Scholar] [PubMed]
- 8. Fard SB, Jamshidi SMM, Hoveidaei AH, Razzaghof M, Mortazavi SMJ. Nonunion following valgus subtrochanteric osteotomy for neglected femoral neck fracture. Trauma Mon 2023;28:e131820. [Google Scholar] [PubMed]
- 9. Padhye KP, Kulkarni VS, Kulkarni GS, Kulkarni MG, Kulkarni S, Kulkarni R, et al. Plating, nailing, external fixation, and fibular strut grafting for nonunions. Indian J Orthop 2013;47:117-25. [Google Scholar] [PubMed]
- 10. Balasubramanian N, Babu G, Prakasam S. Treatment of nonunions of subtrochanteric fractures using valgus osteotomy and angle blade plate. J Clin Diagn Res 2016;10:RC01-4. [Google Scholar] [PubMed]
- 11. Rehme-Röhrl J, Brand A, Dolt A, Grünewald D, Hoffmann R, Stuby F, et al. Functional and radiological results following revision surgery for trochanteric and subtrochanteric nonunion. Arch Orthop Trauma Surg 2024;144:2211-20. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Functional Outcomes of Valgus Osteotomy in Young Patients of Intracapsular Neck of Femur Fracture: A Case Series
August 1, 2026 Functional Outcomes of Valgus Osteotomy in Young Patients of Intracapsular Neck of Femur Fracture: A Case Series July 1, 2026 Large Posterior Proximal Femur Osteochondroma Presenting in Adulthood – Diagnostic Challenges and Management Strategy: A Case Report
July 1, 2026 Large Posterior Proximal Femur Osteochondroma Presenting in Adulthood – Diagnostic Challenges and Management Strategy: A Case Report May 1, 2026 Removal of Hartshill Rectangle and Wires with Revision Pedicle Screw Fixation: Technical Challenges, Safety Considerations, and Clinical Outcomes in Complex Spinal Reconstruction – A Case Report
May 1, 2026 Removal of Hartshill Rectangle and Wires with Revision Pedicle Screw Fixation: Technical Challenges, Safety Considerations, and Clinical Outcomes in Complex Spinal Reconstruction – A Case Report April 1, 2026 A Rare and Interesting Case of Sciatic Nerve Compression Due to Proximal Femoral Osteochondroma in a Young Adult – A Case Report
April 1, 2026 A Rare and Interesting Case of Sciatic Nerve Compression Due to Proximal Femoral Osteochondroma in a Young Adult – A Case Report