
Intraoperative pressure sensors provide objective measurement of compartmental loads, improving the accuracy of ligament balancing during TKA. Functional alignment combined with sensor technology may enhance early clinical outcomes by restoring physiological knee biomechanics.
Dr. Mrudul Kyada, Department of Orthopaedics, GMERS Medical College, Vadnagar, Gujarat, India. E-mail: mrudulkyada@ymail.com
Abstract
Introduction: Even with the present developments of total knee arthroplasty (TKA), a significant percentage of patients are still not satisfied after surgery, mostly because of the presence of pain and instability associated with poor balance of soft tissues. The philosophy of functional alignment has been proposed as a patient-specific philosophy of alignment with the intention to restore native knee kinematics, and intraoperative sensor technology has offered objective, real-time measurement of loads in the mediolateral compartments. There is little evidence on the integrated clinical outcome of functional alignment TKA with intraoperative sensors.
Purpose: To compare clinical, functional, and biomechanical outcomes of functional alignment TKA with sensor guidance intraoperative in patients with primary knee osteoarthritis.
Materials and Methods: A prospective cohort study with 50 patients undergoing primary unilateral TKA using the principles of functional alignment and intraoperative pressure-sensing technology was used. The intraoperative medial and lateral compartment loads were measured as pre- and post-balancing. Clinical outcomes, including Knee Society Score (KSS), Visual Analogue Scale (VAS), range of motion, radiographic alignment, complication rates, and patient satisfaction, were assessed pre-operatively and at 6 months post-operatively. Statistical analysis was performed using a paired t-test and descriptive statistics, with P < 0.05 considered significant.
Findings: Patients had poor knee performance (KSS-knee 42.6 ± 8.9; KSS-function 39.8 ± 9.4) and a high pain level (VAS 7.6 ± 1.1) pre-operatively. Significant mediolateral load imbalance at the start of the procedure (extension: 16.8 ± 6.2 lbs; 90° flexion: 10.9 ± 5.1 lbs) was significantly decreased after sensor-guided adjustments (extension: 2.5 ± 1.6 lbs; 90° flexion: 1.9 ± 1.4 lbs). KSS-knee (86.3 ± 7.4), KSS-function (82.1 ± 8.2), and VAS pain scales (1.8 ± 0.9) recorded significant improvements (P < 0.001) at 6 months post-operatively, and range of motion (118.6 ± 9.8) was improved (P < 0.001). In 88% of patients, acceptable limb positioning within the range of 3° of the neutral position was possible. The overall patient satisfaction was 92, and the rate of complication was low, and no revision was made.
Conclusion: The TKA with intraoperative sensor technology functional alignment led to effective soft-tissue positioning, a strong functional outcome, great pain management, and high patient satisfaction, which appears to be a promising personalised approach for TKA.
Keywords: Functional alignment, intraoperative sensors, patient-reported outcomes, soft-tissue balance, total knee arthroplasty.
Total knee arthroplasty (TKA) is a tried-and-true surgical procedure that has a high success rate in treating advanced knee osteoarthritis, restoring function, and improving quality of life. Despite improvements in imprinting and surgical procedures, 20–30% of patients still have unhappiness after TKA. This is often because of prolonged pain, instability, stiffness, or an altered sensation of the knee [1]. The proper alignment and appropriate tension of soft tissues across the whole range of motion are two of the most important aspects impacting clinical performance and the longevity of implants [2]. The conventional approach to neutral limb alignment is mechanical alignment, which entails fixing the tibial and femoral components at right angles to the mechanical axis [3]. The approach has been shown to be long-lasting, but it doesn’t account for each patient’s specific anatomy and knee kinematics, which might cause functional impairment and patient dissatisfaction [4]. New alignment philosophies, such as functional alignment and kinematic alignment emerged to accommodate individual patients’ anatomy and soft-tissue envelopes in component orientation [5]. To achieve the best possible stability and mobility, functional alignment uses pre-operative planning, intraoperative measurement of soft-tissue tension, and controlled movements in component positioning to restore knee balance, as opposed to strictly adhering to a neutral mechanical alignment [6]. Maintaining consistent and accurate soft-tissue balance during surgery is still difficult when traditional gap-balancing methods and the surgeon’s skill alone are used [7]. Resections of bone, implant placement, and releases of soft tissues may all be guided by the real-time data provided by these sensors [8]. Such wireless pressure sensors allow surgeons to identify asymmetries that could otherwise be missed during physical inspection [9] by tracking the pressures applied by the medial and lateral compartments as the body bends and stretches. Early post-operative instability, sagittal and coronal instability, and intercompartmental load imbalance may be reduced with sensor-guided TKA, according to research [10,11]. Improved early functional outcomes, greater patient satisfaction, and decreased rates of instability and pain-related revision have been linked to a more stable intraoperative environment with sensor support, according to a recent study [12]. To maintain implants in place while retaining natural knee biomechanics, it is best to integrate intraoperative sensors with an efficient alignment strategy. This increases the odds of adjusting implant placement without affecting safe alignment margins. Although there are clear benefits, the clinical outcomes of functional alignment TKA with intraoperative sensors are still not well understood, especially in a standardised outcome assessment prospective cohort trial. Clinical investigations evaluating sensor-guided functional alignment TKA have not adequately assessed alignment parameters, functional scales, patient-reported outcomes, or complication rates. Further investigation into the effects of this combination is necessary to determine the clinical advantages compared to traditional methods and whether or not these advantages are enough to justify the higher cost and more complicated procedures linked with sensor technology. Despite increasing interest in functional alignment and intraoperative sensor-guided balancing during TKA, prospective clinical studies evaluating their combined effect on functional outcomes, alignment accuracy, and patient satisfaction remain limited. Most available studies have evaluated sensor technology or alignment philosophy independently, with limited evidence assessing their integrated clinical performance. We hypothesized that functional alignment TKA assisted by intraoperative pressure sensors would improve soft-tissue balance, post-operative functional outcomes, pain relief, and patient satisfaction while maintaining acceptable alignment parameters.
Study design:
This is a prospective cohort study conducted in the department of orthopaedics of a tertiary care teaching hospital with a high volume of joint replacement surgeries over a period of 18 months. The study aimed to evaluate the clinical outcomes of functional alignment TKA using intraoperative sensor technology. The study protocol was approved by the Institutional Ethics Committee, and written informed consent was obtained from all patients before inclusion in the study.
Participants:
Patients were included for the study if they were scheduled to have primary TKA and had symptoms of knee osteoarthritis.
Inclusion criteria:
Adults: Between 50 and 80 years old.
- Clinical and radiological diagnosed cases of primary knee osteoarthritis
- Patients who are indicated to unilateral primary TKA
- Capability of giving written informed consent.
- Ready to adhere to follow-up procedures
- Kellgren-Lawrence grade III or IV osteoarthritis on radiographic evaluation.
Exclusion criteria:
- Inflammatory arthritis, such as rheumatoid arthritis
- Post-traumatic arthritis that has severe bone loss
- Previous knee surgery to the knee alignment or ligament balance
- Severe extra-articular deformities
- Neuromuscular diseases that involve the gait or knee stability
- Active infection or history of septic arthritis of the knee.
Study sampling:
This study used a successive sampling strategy. We included patients in a sequential fashion until we reached the target sample size if they met the inclusion criteria at any point throughout the research. This strategy produced a more accurate representation of individuals undergoing primary TKA at the study site while also reducing selection bias.
Study sample size:
The sample size was estimated based on previous studies evaluating functional outcomes following sensor-assisted TKA. Considering post-operative knee society score (KSS) improvement as the primary outcome, a confidence interval (CI) of 95% and statistical power of 80% were considered. Due to the limited availability of prior comparable data and the exploratory nature of the study, 50 patients were included as a pilot cohort for preliminary outcome assessment.
Study parameters:
Study variables included demographic characteristics, clinical outcomes, intraoperative sensor measurements, radiological alignment, and post-operative complications. Functional outcome assessed using the KSS was considered the primary outcome measure. Secondary outcomes included pain assessed by visual analogue scale (VAS) score, range of motion, compartment load balance, patient satisfaction, and postoperative complications.
Study procedure:
Surgeons with expertise in orthopaedics and functional alignment performed all of the procedures. Preoperative planning was based on standard radiography. The objective, regardless of the patient’s unique anatomy, was to achieve balanced flexion and extension gaps by using the principles of functional alignment. Following bone resections and temporary implant installation, intraoperative sensors were implanted VERASENSE™ (OrthoSensor Inc., USA) pressure-sensing technology was used for intraoperative compartment load assessment. To maintain the medial-lateral balance across the whole range of motion, the sensors provide real-time input to selected medial-lateral releases or small component adjustments. Finally, the components were implanted when a sufficient balance had been obtained; an acceptable balance was defined as a mediolateral compartment load difference of less than 15 lbs throughout the range of motion. Physiotherapy was an integral aspect of post-operative recovery for all patients.
Study data collection:
When gathering information, a systematic pro forma was used. Data collected before surgery included patient demographics, medical history, and functional capacity at baseline. Surgical details, sensor load measurements, and configuration settings were all part of the intraoperative data set. Documentation of post-operative data, including results of clinical examination, functional ratings, and radiological evaluation, was done during routine follow-up appointments. The data was meticulously documented by the experienced workers, who ensured its accuracy and consistency.
Data analysis:
Statistical analysis was performed using the Statistical Package for the Social Sciences software version XX (IBM Corp., Armonk, NY, USA). Continuous variables were expressed as mean ± standard deviation (SD), while categorical variables were expressed as frequencies and percentages. Pre- and post-operative continuous variables were compared using paired t-tests. A P < 0.05 was considered statistically significant. Missing data were excluded from the final analysis.
A total of 50 patients undergoing functional alignment TKA with intraoperative sensor guidance were included in the study. The majority of patients belonged to the 60–69 years age group (52%), while 24% each were aged 50–59 years and ≥70 years, with a mean age of 64.2 ± 7.1 years. Female patients constituted 56% of the study population, whereas males accounted for 44%. The mean body mass index of the participants was 28.4 ± 3.6 kg/m2, indicating that most patients were overweight. The right knee was more commonly operated on (54%) compared to the left knee (46%). The mean duration of symptoms before surgery was 6.8 ± 2.1 years, reflecting chronic symptomatic knee osteoarthritis requiring surgical intervention (Fig. 1).
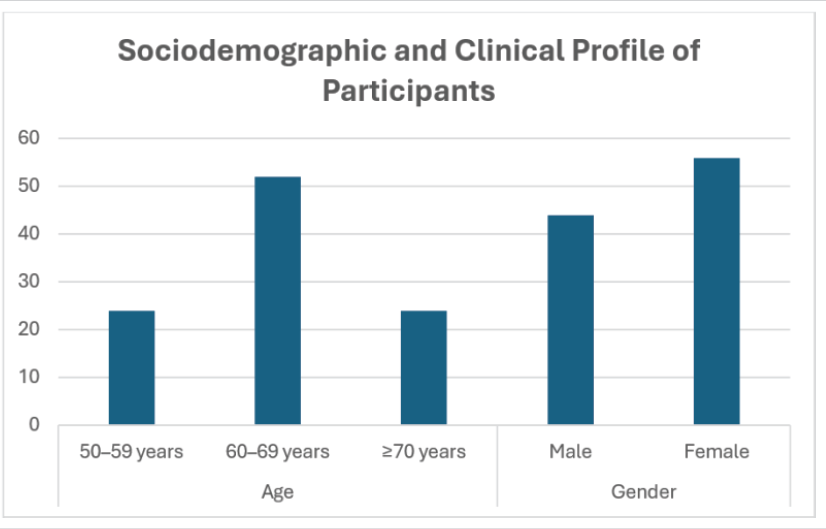
Figure 1: Distribution of age and gender among study participants.
Preoperative functional assessment demonstrated marked impairment in knee function and significant pain among the study participants. The mean KSS for the knee component was 42.6 ± 8.9, while the mean functional component score was 39.8 ± 9.4, indicating poor baseline functional status. Patients also reported severe pain pre-operatively, with a mean VAS score of 7.6 ± 1.1. In addition, the average pre-operative range of motion was restricted to 96.4 ± 12.7°, reflecting substantial limitation in knee mobility associated with advanced osteoarthritis (Table 1 and Fig. 2).
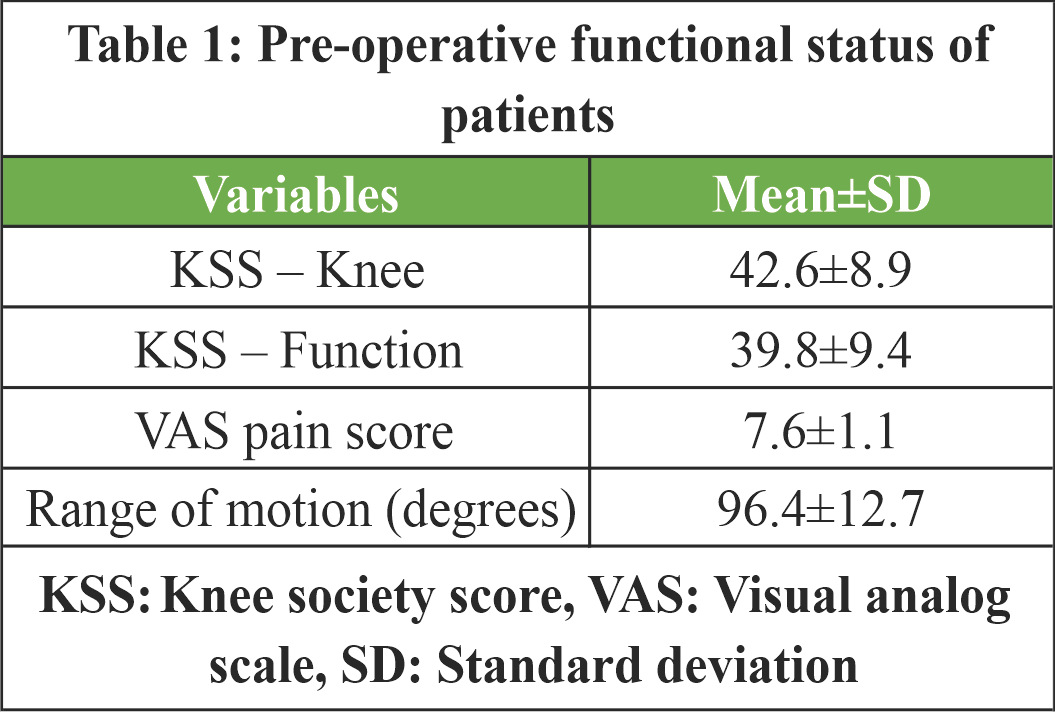
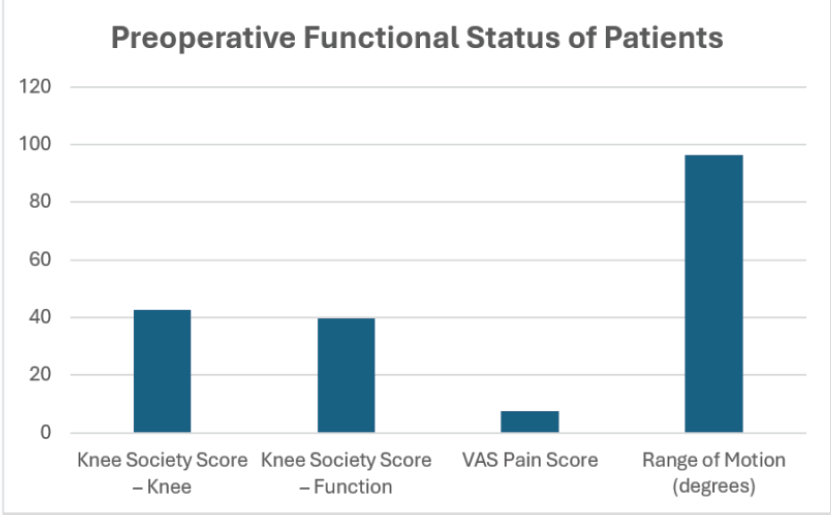
Figure 2: Preoperative functional status of patients undergoing functional alignment total knee arthroplasty.
Intraoperative sensor assessment demonstrated significant mediolateral load imbalance before soft-tissue balancing, particularly in extension, where the mean load difference was 16.8 ± 6.2 lb. Following sensor-guided balancing, compartmental load differences were markedly reduced to 2.5 ± 1.6 lbs in extension and 1.9 ± 1.4 lbs at 90° flexion, indicating successful restoration of soft-tissue balance throughout the range of motion (Table 2 and Fig. 3).

Table 2: Intraoperative sensor load distribution before and after balancing
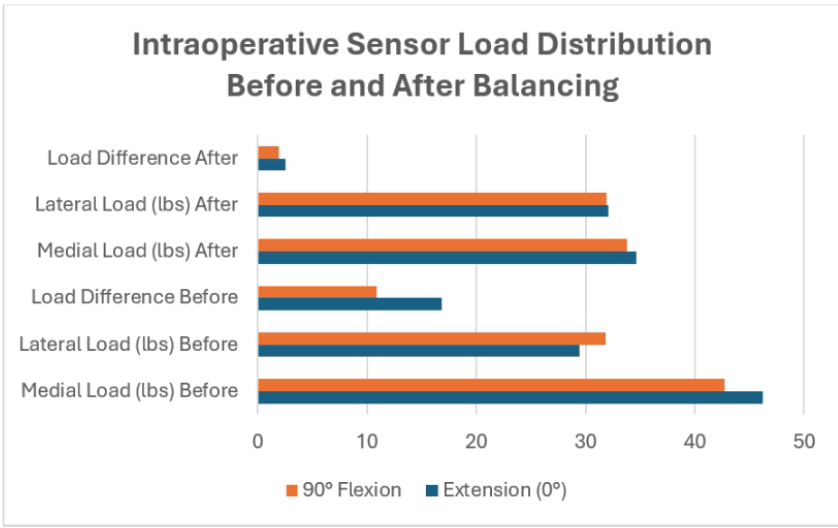
Figure 3: Intraoperative compartment load distribution before and after balancing.
Post-operative evaluation demonstrated significant improvement in clinical and functional outcomes following functional alignment TKA with intraoperative sensor guidance. The mean KSS for the knee component improved from 42.6 ± 8.9 pre-operatively to 86.3 ± 7.4 post-operatively, while the functional score increased from 39.8 ± 9.4 to 82.1 ± 8.2. Mean VAS pain score decreased markedly from 7.6 ± 1.1 to 1.8 ± 0.9, indicating substantial pain relief. Range of motion also improved from 96.4° pre-operatively to 118.6° at 6 months’ follow-up. Acceptable limb alignment within ±3° was achieved in 88% of patients. Post-operative complications were minimal, including knee stiffness in 6%, superficial infection in 4%, and instability in 2% of patients, while no revision surgeries were required. Patient satisfaction was high, with 64% reporting being very satisfied and 28% satisfied with the surgical outcome (Table 3).
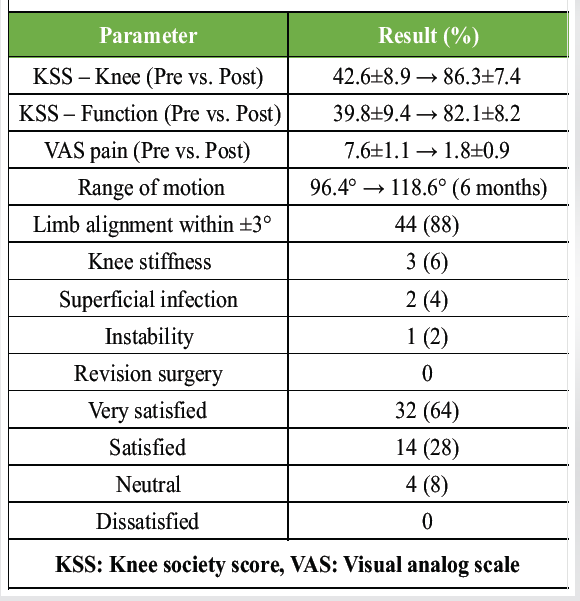
Table 3: Post-operative clinical and radiological outcomes
The present prospective cohort study demonstrated that functional alignment TKA assisted by intraoperative pressure sensors achieved effective mediolateral soft-tissue balancing with significant improvement in post-operative pain, knee function, range of motion, and patient satisfaction. In the present group of 50 patients, with an average age of 64.2 ± 7.1 years and 56% being female, there was a noticeable functional impairment before surgery. The average KSSs were 42.6 ± 8.9 for the knee component and 39.8 ± 9.4 for the function. In addition, the average VAS pain was large at 7.6 ± 1.1, and the range of motion was limited at 96.4 ± 12.7°. Within the operating room, pre-balancing sensor readings revealed a significant disparity between the medial and lateral load differences, averaging 16.8 ± 6.2 lbs in extension and 10.9 ± 5.1 lbs at 90° flexion. This finding highlights the drawbacks of subjective balancing techniques. This disparity was reduced to 2.5 ± 1.6 lbs in extension and 1.9 ± 1.4 lbs in flexion after the extremity was functionally aligned with the help of sensors. This indicates that the symmetrical tension of soft tissues across the range of motion was successfully restored. This finding is in good agreement with the prospective study conducted by Chang et al. [13], which examined 30 patients who underwent robotic-assisted functional alignment TKA with sensor guidance intraoperatively. The study indicated that at 10°, 45°, and 90° of flexion, there were balanced compartment pressures in the medial and lateral compartments, with no significant statistical differences between the compartments (P = 0.140, 0.510, and 0.800, respectively), and a low mean intercompartmental gap. This study further supports the biomechanical rationale for functional alignment by showing that, similar to Chang et al., it is always possible to achieve balanced tension in the soft tissues during the knee flexion step with the help of objective intraoperative sensor feedback. In this study, we found that there was a significant improvement in clinical outcomes, including pain levels (VAS 1.8 ± 0.9; P < 0.001), range of motion (118.6 ± 9.8 o), and overall health. At 6 months, the mean KSS-knee score was 86.3 ± 7.4, and at the end of the follow-up period, it was 82.1 ± 8.2. Hazratwala et al. found that in 165 computer-navigated functional alignment TKAs, patients reported the best post-operative outcomes. Range of motion was stable, going from 118.6 at 2 years to 120.1 at 1 year. Despite a shorter post-operative period in the present study, the functional score and motion improvement magnitude and direction were highly similar to the initial course of progressions in the CAS (Computer-Assisted Surgery)-assisted functional alignment cohort. Since 88% of patients would agree within 3° of neutral, the results of post-operative alignment used in this research also proved that functional alignment did not compromise the safety of alignment. In a study conducted by Chang et al., it was found that the average post-operative limb positioning was 2.2° varus (SD 1.0°). However, the researchers found that the pressures in both compartments were balanced, lending credence to the idea that minimal constitutional positioning can be maintained without compromising balance. Remarkably, the present study had a low complication rate; no subjects required revisions, and only 2% of subjects experienced post-operative instability. This is in line with the tolerable short-term revision and complication rates reported by Hazratwala et al. [14], who discovered that functional alignment TKA was predictable and reproducible, with releases on soft tissues occurring in just 14.5% of cases. On the flip side, when looking at the larger body of research on sensor-assisted balance, it is important to consider that sensors are not always linked to better clinical outcomes. This data should be considered with the results of the present study. Despite a considerably greater proportion of balancing procedures in the sensor group (55.9 vs. 16.9), MacDessi et al. [15] discovered no statistically significant difference in the mean change in the aggregate of Knee Injury and Osteoarthritis Outcome Score (KOOS)4 scores at 2 years (41.5 vs. 42.4; P = 0.62). The study included a large comparative cohort of 222 sensor-balanced and 207 manually balanced TKAs, respectively. Similarly, in Tran et al. [16], a meta-analysis of four randomised controlled trials found no significant difference in functional scores (standardised mean difference 0.10; 95% CI −0.15–0.34), complication rates (odds ratio 0.84; 95% CI 0.46–1.54), or range of motion (mean difference 1.20°; 95% CI −0.26–2.65) when comparing sensor-guided balancing to manual techniques. Therefore, this research suggests that sensor technology’s clinical utility is best assessed by looking at its role in surgical philosophy rather than its use alone. Also, it’s important to note that whereas MacDessi et al. [15] and Tran et al. [16] only examined sensors in mechanically aligned or typical balancing setups, the present work used sensors in addition to functional alignment, which may explain the favourable findings. Here, Wakelin et al. [17], showed that superior 2-year pain outcomes after TKA were associated with intraoperatively assessed joint laxity and balance rather than component alignment alone. For knees that fulfilled all of the specified laxity and balance windows, Wakelin et al. [17] discovered a statistically significant difference in KOOS pain scores (100.0 vs. 94.4; P < 0.0001) and a higher rate of reaching the patient-acceptable symptom state (93% vs. 71%; P = 0.0009). However, no optimal alignment windows were found to be associated with pain outcomes. Even though there were small variations in alignment, the present investigation found that sensor-guided balancing was successful and associated with considerable pain reduction and patient satisfaction (92% happy or extremely satisfied). The available information suggests that intraoperative sensors are best used to optimise soft-tissue balance within a functional alignment paradigm, rather than as a standalone tool in the conventional alignment concept.” This is because they are specifically designed for this purpose. While there is a lack of a control group and the follow-up is rather short, the present study’s alignment safety, positive early functional outcome, and consistency of intraoperative balance correction are in line with new evidence on the primacy of balance over mechanical alignment. While more research into the durability and efficacy of sensor-assisted functional alignment as an alternative to contemporary TKA is required, the present study does provide important information regarding the potential benefits of this technique. The strengths of the present study include its prospective design, objective intraoperative sensor measurements, standardised surgical protocol, and comprehensive functional assessment. However, certain limitations should be acknowledged. The strengths of this study include its prospective design, objective intraoperative sensor measurements, standardised surgical technique, and comprehensive evaluation of clinical, functional, and radiological outcomes. However, several limitations should be noted. The small sample size (n = 50) and single-centre design may limit statistical power and generalisability. The absence of a control group and the non-randomised design preclude direct comparison with conventional techniques and introduce the potential for selection bias and confounding. The 6-month follow-up period does not permit assessment of long-term implant survival, wear, loosening, or revision rates; therefore, the findings should be considered exploratory. Only one alignment strategy and implant philosophy were evaluated, limiting applicability to other approaches. All surgeries were performed by experienced arthroplasty surgeons, which may reduce generalisability to lower-volume centres. Lack of blinding may have introduced observer and reporting bias, while patient-reported outcomes (KSS, VAS, and satisfaction scores) remain subject to patient expectations. Radiological assessment was limited to overall alignment without detailed analysis of component rotation or three-dimensional positioning. In addition, the learning curve associated with sensor-guided functional alignment and the cost-effectiveness of this technology were not evaluated. Finally, exclusion of complex cases may limit the applicability of these findings to the broader TKA population.
Functional alignment TKA assisted by intraoperative pressure sensors appears to provide favorable short-term clinical and functional outcomes in patients with primary knee osteoarthritis. The technique demonstrated effective soft-tissue balancing, improved post-operative knee function, and high patient satisfaction while maintaining acceptable alignment parameters. However, larger comparative studies with long-term follow-up are necessary to validate these findings and determine long-term implant survivorship.
Sensor-guided functional alignment in total knee arthroplasty may improve intraoperative soft-tissue balancing and post-operative functional recovery in selected patients when performed by experienced surgeons.
[refernces_numbered]1. Goldsack JC, Coravos A, Bakker JP, Bent B, Dowling AV, Fitzer-Attas C, et al. Verification, analytical validation, and clinical validation (V3): The foundation of determining fit-for-purpose for biometric monitoring technologies (BioMeTs). NPJ Digit Med 2020;3:55.
2. Zheng G, Tian W, Zhuang X, editors. Intelligent orthopaedics – artificial intelligence and smart image-guided technology for orthopaedics. In: Advances in Experimental Medicine and Biology. Vol. 1093. Berlin: Springer; 2018. p. 1-335.
3. Gustke KA, Golladay GJ, Roche MW, Elson LC, Anderson CR. A new method for defining balance: Promising short-term clinical outcomes of sensor-guided TKA. J Arthroplast 2014;29:955-60.
4. Ledet EH, Liddle B, Kradinova K, Harper S. Smart implants in orthopedic surgery, improving patient outcomes: A review. Innov Entrep Health 2018;5:41-51.
5. D’Lima DD, Fregly BJ, Colwell CW Jr. Implantable sensor technology: Measuring bone and joint biomechanics of daily life in vivo. Arthritis Res Ther 2013;15:203.
6. Safiri S, Kolahi AA, Smith E, Hill C, Bettampadi D, Mansournia MA, et al. Global, regional and national burden of osteoarthritis 1990-2017: A systematic analysis of the global burden of disease study. Ann Rheum Dis 2017;2020:819-28.
7. Murphy L, Schwartz TA, Helmick CG, Renner JB, Tudor G, Koch G, et al. Lifetime risk of symptomatic knee osteoarthritis. Arthritis Rheum 2008;59:1207-13.
8. Burn E, Murray DW, Hawker GA, Pinedo-Villanueva R, Prieto-Alhambra D. Lifetime risk of knee and hip replacement following a GP diagnosis of osteoarthritis: A real-world cohort study. Osteoarthritis Cartilage 2019;27:1627-35.
9. Culliford DJ, Maskell J, Kiran A, Judge A, Javaid MK, Cooper C, et al. The lifetime risk of total hip and knee arthroplasty: Results from the UK general practice research database. Osteoarthritis Cartilage 2012;20:519-24.
10. Scott CE, Howie CR, MacDonald D, Biant LC. Predicting dissatisfaction following total knee replacement: A prospective study of 1217 patients. J Bone Joint Surg Br 2010;92:1253-8.
11. Clement ND, Bardgett M, Weir D, Holland J, Gerrand C, Deehan DJ. Three groups of dissatisfied patients exist after total knee arthroplasty: Early, persistent, and late. Bone Joint J 2018;100B:161-9.
12. Yapp LZ, Clement ND, Macdonald DJ, Howie CR, Scott CE. Changes in expectation fulfillment following total knee arthroplasty: A 10-year follow-up study. J Arthroplast 2020;35:1826-32.
13. Chang JS, Kayani B, Wallace C, Haddad FS. Functional alignment achieves soft-tissue balance in total knee arthroplasty as measured with quantitative sensor-guided technology. Bone Joint J 2021;103:507-14.
14. Hazratwala K, Gouk C, Wilkinson MP, O’Callaghan WB. Navigated functional alignment total knee arthroplasty achieves reliable, reproducible and accurate results with high patient satisfaction. Knee Surg Sports Traumatol Arthrosc 2023;31:3861-70.
15. MacDessi SJ, Cohen DA, Wood JA, Diwan AD, Harris IA. Does the use of intraoperative pressure sensors for knee balancing in total knee arthroplasty improve clinical outcomes? A comparative study with a minimum two-year follow-up. J Arthroplasty 2021;36:514-9.
16. Tran JY, Lee JW, Wong CK, Lam GY, Choi TL, Mak WF, et al. A comparison on the clinical outcomes of using intraoperative load sensors versus manual balancing in total knee arthroplasty: A systematic review and meta-analysis. J Orthop Surg Res 2025;20:970.
17. Wakelin EA, Ponder CE, Randall AL, Koenig JA, Plaskos C, DeClaire JH, et al. Intra-operative laxity and balance impact 2-year pain outcomes in TKA: A prospective cohort study. Knee Surg Sports Traumatol Arthrosc 2023;31:5535-45.[/refernces_numbered]






Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 The Boba Tea Sign: A Novel Magnetic Resonance Imaging Finding in Synovial Chondromatosis of the Knee – A Case Report
August 1, 2026 The Boba Tea Sign: A Novel Magnetic Resonance Imaging Finding in Synovial Chondromatosis of the Knee – A Case Report August 1, 2026 Intrawound Vancomycin and Povidone-Iodine Treatment to Reduce Infection Rates in Arthroplasty
August 1, 2026 Intrawound Vancomycin and Povidone-Iodine Treatment to Reduce Infection Rates in Arthroplasty July 1, 2026 Lipoma Arborescens of the Knee: An Intraoperative Mimicker of Pigmented Villonodular Synovitis in Bilateral Knee Osteoarthritis – A Case Report
July 1, 2026 Lipoma Arborescens of the Knee: An Intraoperative Mimicker of Pigmented Villonodular Synovitis in Bilateral Knee Osteoarthritis – A Case Report July 1, 2026 Megaprosthetic Total Knee Arthroplasty for Supracondylar Refracture in a Post-traumatic Osteoarthritic Knee: A Case Report
July 1, 2026 Megaprosthetic Total Knee Arthroplasty for Supracondylar Refracture in a Post-traumatic Osteoarthritic Knee: A Case Report