
Early CT-based fracture assessment and column-specific fixation can achieve excellent functional recovery in complex tibial plateau fractures, despite increasing fracture severity and radiological complexity.
Dr. P Velmurugan, Department of Orthopedic Surgery, Sri Ramachandra Institute of Higher Education and Research, Porur, Chennai - 600116, Tamil Nadu, India. E-mail: velpadha88@yahoo.com
Abstract
Introduction: Complex proximal tibial plateau fractures are challenging injuries with substantial risk of malalignment, joint stiffness, and post-traumatic osteoarthritis. Column-based plating guided by computed tomography-based three-column concepts has been proposed to improve fixation, but the relative influence of fracture classification and plate configuration on outcome remains unclear.
Materials and Methods: In this prospective observational study, 57 adults (20–70 years) with complex proximal tibial plateau fractures treated with column-based plating at a single tertiary centre (January 2023–January 2024) were evaluated. Fractures were classified by Schatzker (IV–VI) and Luo’s three-column system (types 2 and 3). Patients underwent either single-plate or dual-plate fixation based on fracture morphology. Clinical and radiological outcomes were assessed at 1, 6, and 12 months using the modified Rasmussen clinical and radiological scores, the International Knee Documentation Committee (IKDC) score, and the Knee Society Score (KSS). Correlations of fracture classifications and plate number with these outcomes were analysed.
Results: The cohort included 37 males and 20 females; 40 fractures were right-sided. Schatzker types were IV (n = 6), V (n = 27), and VI (n = 24). Luo classification was type 2 (n = 29) and type 3 (n = 28). Dual-plate fixation was used in 38 patients (66.7%), and single-plate fixation in 19 (33.3%). At 1 year, modified Rasmussen clinical scores were excellent in 31 patients (54.4%) and good in 26 (45.6%). Radiologically, 19 patients (33.3%) had excellent, 31 (54.4%) good, and 7 (12.3%) fair results. Schatzker and Luo classifications showed strong and moderate negative correlations, respectively, with radiological scores at all time points, but no significant correlation with clinical scores. Dual plating was associated with slightly higher mean radiological scores than single plating at 1, 6, and 12 months, while clinical scores (Rasmussen, IKDC, KSS) were similar between groups. Complications included one common peroneal nerve palsy requiring tendon transfer, and one superficial surgical site infection was observed.
Conclusion: In complex proximal tibial plateau fractures treated with column-based plating, fracture severity (Schatzker and Luo) strongly influences radiological outcomes but not short-term functional recovery. Dual-plate fixation affords modestly superior radiological restoration compared with single-plate constructs, whereas functional scores at 1 year are comparable. Column-specific preoperative planning and fixation can yield consistently good clinical outcomes even in high-grade fracture patterns.
Keywords: Tibial plateau fracture, proximal tibia, three-column concept, Schatzker, Luo classification, dual plating, Rasmussen score, International Knee Documentation Committee, Knee Society Score.
The bimodal distribution pattern of proximal tibia fractures includes younger men with high-energy trauma and osteoporotic elderly women with low-energy trauma [1]. The treatment of complex tibia fractures caused by high-energy trauma remains a challenge to reconstruct intraoperatively [2]. Several classification systems are in use all over the world [3]. Historically, the Schatzker and AO classification systems are based on radiographic assessment of fracture patterns. A three-column classification system, which is based on computed tomography (CT) imaging, gives more information about the posterior column fractures [4]. The proximal tibia fractures constitute roughly 1% of all fractures. The incidence of complex proximal tibia fractures is 1 in one million all over the world [5]. Complex proximal tibia fractures, often resulting from high-energy trauma, pose significant challenges due to comminution, instability, and associated soft tissue injury. Luo’s three-column classification provides a CT-based framework for surgical planning, and column-based plating has emerged as a biomechanically sound technique [5,6]. A favourable prognosis and appropriate post-operative functioning depend on proper fixation and early post-operative range of motion attainment [7,8,9,10,11]. This case series evaluates functional and radiological outcomes of column-based plating and identifies prognostic factors influencing recovery. To provide a framework for setting reasonable goals resulting in improved patient-reported satisfaction, knowledge of patients’ comprehension concerning post-operative outcomes is essential to direct patient education and shared decision-making [12]. Parallel to this conceptual shift, fixation philosophies have evolved from conservative treatment and limited internal fixation to more stable constructs such as dual buttress plating, hybrid external fixation, periarticular locking plates, and, increasingly, column-based plating. Ankle and knee articular injuries and axial malalignment can raise the risk of post-traumatic osteoarthritis, which can result in an early ankle joint fusion or total knee replacement. As a result, complicated tibial articular fractures may have a major socioeconomic impact on the patient population and lower their quality of life [13]. Surgical alternatives include reduction and osteosynthesis with screws, a single or double plate, or external fixation, depending on the kind of fracture. Restoring the articular surface and limb mechanical axis is the aim of surgery in every situation [14]. The location of the fracture lines and the fracture pattern serve as guidelines for the selection of plate configuration and placement. For instance, medial column plating may be used to repair the medial joint surface and stop varus collapse in cases of medial tibia plateau fractures. Similarly, to restore joint congruity and avoid valgus collapse, lateral column plating may be utilised for fractures impacting the lateral tibia plateau. Dual plating procedures may be used to achieve sufficient stability and alignment in more difficult fractures that include both the medial and lateral columns. Dual plating through separate medial and lateral approaches has shown reliable union and alignment in bicondylar fractures, but the relative contribution of fracture class, column involvement, and plate configuration to functional outcome remains debated.
Study design and setting: This was a prospective observational study conducted in the Department of Orthopaedic Surgery at a tertiary teaching hospital in Chennai, India, from January 2023 to January 2024. Institutional ethics committee approval was obtained before recruitment, and written informed consent was taken from all participants. The IEC number: CSP/MED/23/JUN/88/132. Date of approval: October 30 October, 2023.
Inclusion criteria:
- Age 18–60 years
- Proximal tibial plateau fractures (involving the articular surface) treated with column-based plating
- Operative fixation within the study period
- Ability and willingness to comply with follow-up at 1, 6, and 12 months.
Exclusion criteria:
- Fractures treated conservatively or by non-column-based methods
- Associated fractures of the ipsilateral lower limb, pelvis, and op spine
- Pathological fractures
- Polytrauma precluding standard rehabilitation.
Patient evaluation and fracture classification:
On admission, all patients underwent standard clinical assessment and radiographic evaluation with anteroposterior and lateral knee radiographs. CT scans with multiplanar reconstruction were routinely obtained either before or after application of temporary knee-spanning external fixation when soft-tissue compromise was present. Each fracture was classified using:
- Schatzker classification (IV-VI for this series)
- Luo’s three-column classification defining involvement of anterior-lateral, anteromedial, and posterior columns based on axial CT sections.
For analytical purposes, fractures were grouped as the following:
- Schatzker IV, V, VI
- Luo two- and three-column injuries.
Surgical strategy:
Initial management in high-energy injuries with significant soft-tissue insult comprised provisional external fixation across the knee with pins placed outside future incision zones. Definitive internal fixation was performed once soft-tissue conditions permitted, typically within 1–7 days (mean 3.5 days). Column-based plating was planned according to pre-operative CT:
- Direct approaches to the involved columns (anterolateral, anteromedial, posteromedial as required)
- Anatomically contoured periarticular locking or buttress plates applied to the affected columns
- Indirect reduction techniques where possible, with particular attention to elevation of depressed articular segments, restoration of condylar width, and correction of varus-valgus malalignment.
The patient was categorised based on plate configuration as
- Single plate (SP): lateral or medial column alone
- Dual plates (DP): Combination of medial and lateral (+/− posterior) plates.
Post-operative protocol and follow-up:
Early ankle and hip mobilisation was encouraged from day 1. Knee range of motion exercises were commenced as tolerated, respecting soft-tissue status and fixation stability. Weight-bearing progression was individualised, generally beginning as partial weight-bearing after radiological evidence of early consolidation, advancing to full weight-bearing over 12–18 weeks. Patient reviewed at 1, 6, and 12 months. At each visit, clinical assessment and radiographs of the knee were obtained.
Outcome measures:
Clinical outcome:
- Modified Rasmussen’s clinical score
- International Knee Documentation Committee (IKDC) subjective score
- Knee Society score (KSS).
Radiological outcome:
Modified Rasmussen radiological score
- Articular depression
- Condylar widening
- Varus/Valgus angulation
- Osteoarthritic changes.
Case presentation:
This prospective observational study was conducted between January 2023 and January 2024, including 57 patients aged 18–60 years with proximal tibia fractures treated by column-based plating.
- Schatzker classification: Type IV (6 patients), Type V (27), Type VI (24)
- Luo’s three-column classification: Type II (29 patients), Type III (28 patients)
- Assessment tools: Rasmussen clinical and radiological scores, IKDC score, Oxford Knee Score
- Follow-up: 1 month, 6 months, and 1 year.
Representative case:
A 42-year-old male sustained a bicondylar proximal tibia fracture (Schatzker VI) following a road traffic accident. CT confirmed medial and lateral column involvement (Luo type III) (Figs. 1, 2, 3). Figs. 1a and b illustrate the management sequence:
- A: Pre-operative X-ray showing bicondylar proximal tibia fracture with articular depression and comminution.
- B: Immediate post-operative X-ray showing anatomical reduction and stable fixation.
- C: Follow-up X-ray at 6 months showing consolidated fracture with maintained alignment and satisfactory functional outcome.

Figure 1: [1.1][VM2.1][VM3.1](a and b) Pre-operative X-ray showing bicondylar proximal tibia fracture with articular depression and comminution and immediate post-operative X-ray showing anatomical reduction and stable fixation.
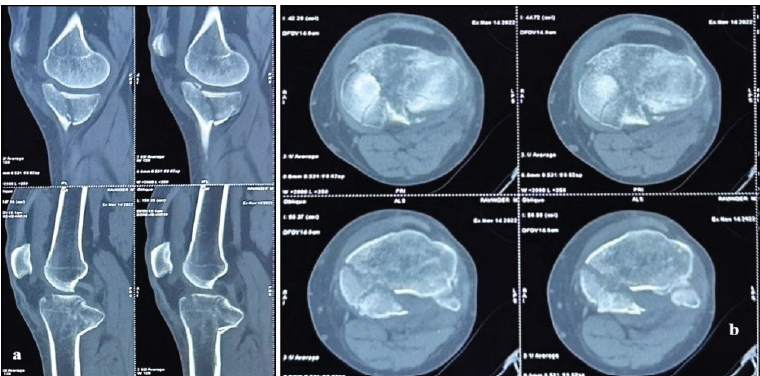
Figure 2: [4.1][VM5.1](a and b) Pre-operative computed tomography image showing bicondylar proximal tibia fracture with posteromedial articular depression and comminution and 2-column involvement appreciated in axial cuts.
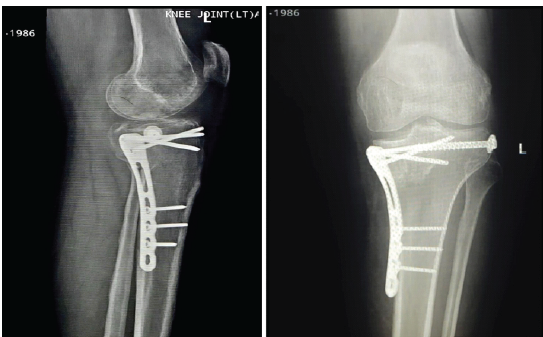
Figure 3: 6-month post-op follow-up X-ray showing complete healing of the fracture.
Functional outcomes (Rasmussen clinical score):
- Excellent: 31 patients (54.3%)
- Good: 26 patients (45.6%).
Radiological outcomes (Rasmussen radiological score):
- Excellent: 19 patients (33.3%)
- Good: 31 patients (54.3%)
- Fair: 7 patients (12.2%).
Complications:
- 1 case of common peroneal nerve injury
- 1 case of surgical site infection.
Dual plating was associated with superior radiological outcomes compared to single plating, though clinical outcomes remained comparable. At 1 month, 6 months, and 1 year after surgical fixation, all patients were assessed using the Rasmussen clinical scoring method. Gradual functional recovery was shown by the total clinical scores, which showed progressive improvement over time. Rasmussen scores at 1 month showed early post-operative functional impairments, ranging from 16 to 21. Scores significantly improved at 6 months, ranging from 24 to 26, indicating a notable improvement in knee function and a decrease in pain. According to the Rasmussen criteria, most patients had scores between 26 and 29 at the 1-year follow-up, suggesting good to excellent functional results. Lower clinical ratings were linked to greater fracture severity, according to an analysis of fracture categorisation. Rasmussen scores were greater in patients with lower Schatzker fracture types than in those with higher Schatzker grades. The Luo three-column classification exhibited a similar pattern, with more complex fractures exhibiting marginally worse functional scores throughout all follow-up intervals. At 1 month, 6 months, and 12 months, patients treated with dual-plate fixation showed somewhat higher mean Rasmussen scores than those treated with single-plate fixation, according to an evaluation of the fixation method. Nonetheless, there was not much of a difference between the two groups, suggesting that both fixation methods produced acceptable clinical results. Overall, the data show that while fracture complexity continued to be a significant predictor of ultimate clinical outcomes, functional outcomes considerably improved over time (Table 1 and Fig. 4, 5, 6, 7).
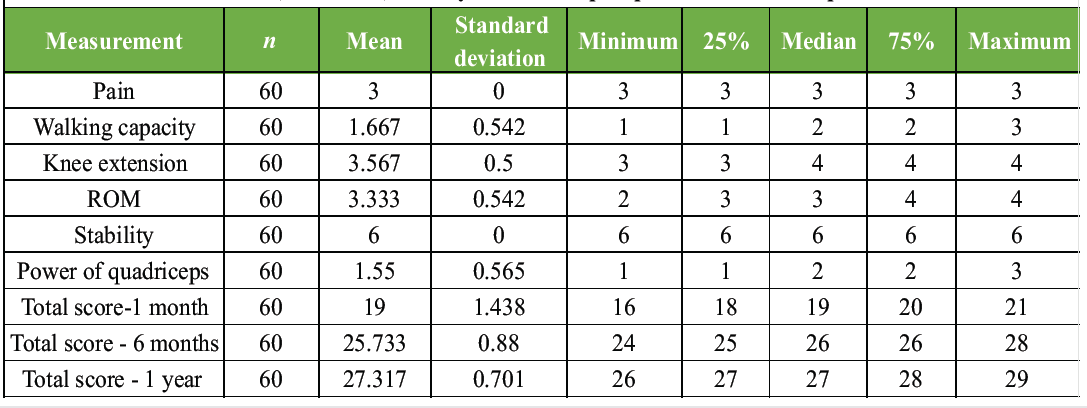
Table 1: Descriptive statistics of individual components of the Rasmussen clinical scoring system and total scores at 1 month, 6 months, and 1-year follow-up in patients with tibial plateau fractures
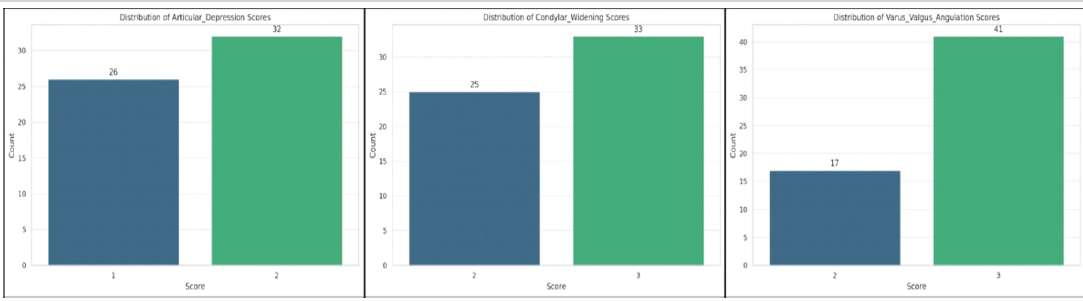
Figure 4: Bar charts showing the distribution of individual radiological components of the Rasmussen score, including articular depression, condylar widening, and varus/valgus angulation. The graphs demonstrate the number of patients in each scoring category, with a greater proportion of patients achieving higher scores, indicating better restoration of articular congruity, condylar alignment, and mechanical axis following surgical fixation.
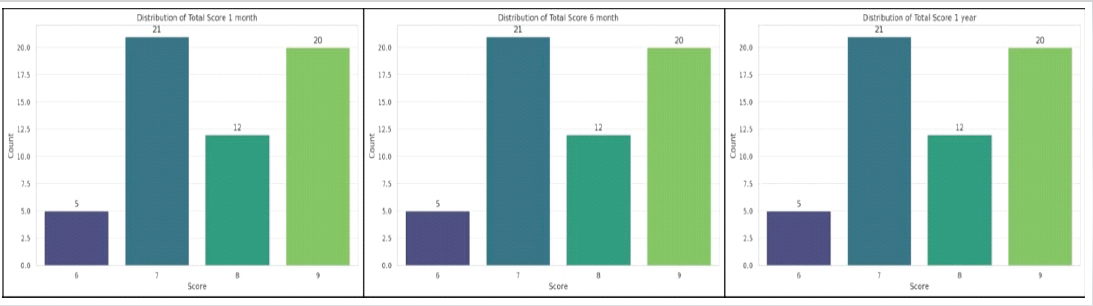
Figure 5: Bar charts illustrating the distribution of Rasmussen clinical scores at 1 month, 6 months, and 1-year follow-up after surgical management of tibial plateau fractures. The graphs show the number of patients achieving each score category, demonstrating a predominance of higher Rasmussen scores (7–9) across all follow-up intervals, indicating generally good to excellent functional outcomes in most patients.
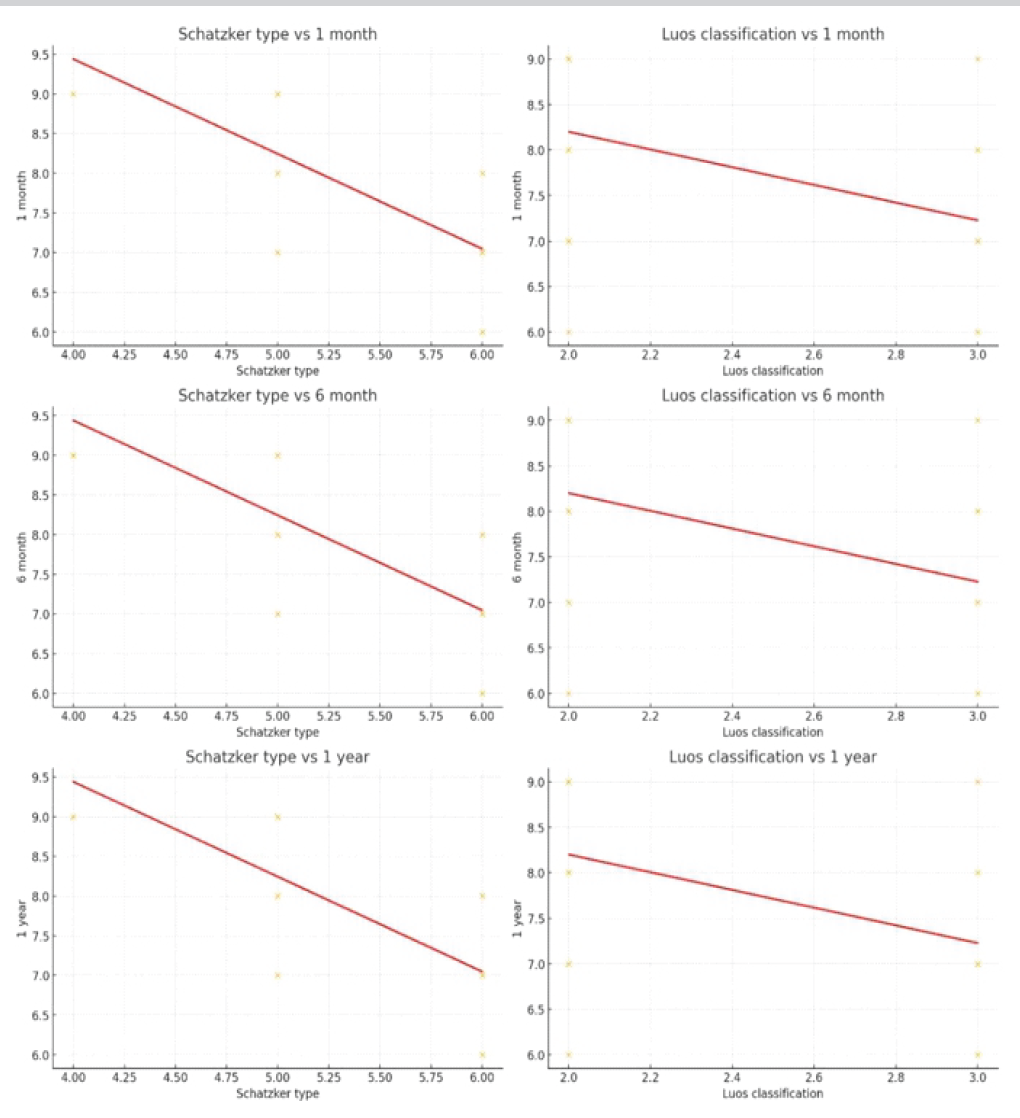
Figure 6: Scatter plots demonstrating the relationship between fracture classification and Rasmussen clinical scores at 1 month, 6 months, and 1-year follow-up. The left column shows the association between Schatzker fracture types (IV–VI) and Rasmussen scores, while the right column shows the association between the Luo three-column classification (Types II–III) and Rasmussen scores. The regression lines demonstrate a negative correlation between increasing fracture severity and clinical scores, indicating relatively lower functional outcomes in higher-grade fracture patterns across all follow-up periods.
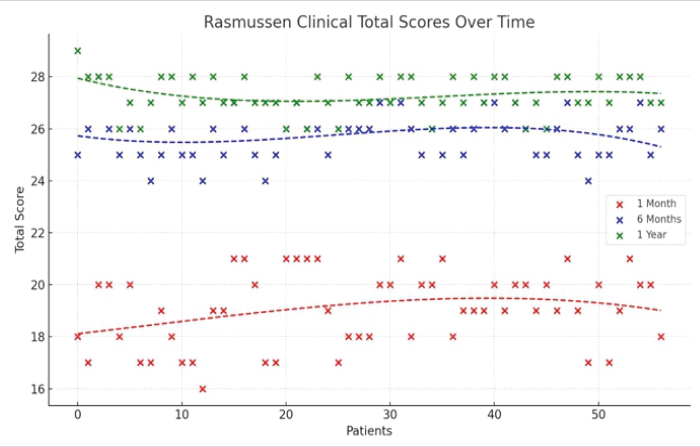
Figure 7: Scatter plot illustrating Rasmussen clinical total scores of patients at 1 month, 6 months, and 1 year after surgery. The plot demonstrates progressive improvement in clinical scores over time, indicating gradual functional recovery following fixation of tibial plateau fractures. Regression Charts-Rasmussen radiological scores with Schatzker and Luo’s classifications.
One of the most often used fixing techniques for high-energy tibial plateau fractures is still open reduction with internal fixation. The most frequent challenges that surgeons encounter when treating intra-articular proximal tibial fractures are poor bone quality and comminuted fracture patterns that make it difficult to achieve stable fixation, as well as compromised skin and soft tissue envelopes that invite a high rate of complications after attempted open reduction and internal fixation [15,16,17,18,19,20]. The CT-based three-column concept provides a more nuanced framework for planning fixation in these high-energy fractures, particularly for posterior and posteromedial fragments that are poorly described by plain radiograph-based systems. Our data confirm that higher Schatzker types and greater column involvement (Luo type 3) are associated with inferior radiological scores, mirroring previous work showing that more complex patterns are harder to fully restore [4,7,8,9,10,11,21]. However, the lack of a strong correlation with clinical scores suggests that, at least within the 1st post-operative year, good function can still be achieved despite some residual radiological imperfection when appropriate fixation and rehabilitation strategies are employed. This case series demonstrates that while Schatzker’s and Luo’s classifications are valuable for pre-operative planning and radiological assessment, they do not significantly alter clinical outcomes. Dual plating provides enhanced stability and better radiological alignment, particularly in bicondylar and comminuted fractures. Column-specific fixation facilitates early mobilisation and rehabilitation, underscoring its biomechanical advantage. In addition to fracture union and functional outcomes, studies have also evaluated the complication rates associated with column-based plating techniques. Smith et al. (2017) reported a complication rate of 15% in their cohort of patients treated with medial column plating, with the most common complications being hardware irritation and wound dehiscence. Similarly, Johnson et al. (2018) found a complication rate of 12% in patients treated with lateral column plating, with most complications being related to hardware failure and infection. This prospective series of 57 complex proximal tibial plateau fractures treated with column-based plating demonstrates that:
- Fracture complexity strongly influences radiological restoration but not short-term clinical outcomes
- DP fixation achieves modestly better radiological alignment than SP constructs, while functional scores at 1 year are comparable.
However, the lack of a strong correlation with clinical scores suggests that, at least within the 1st post-operative year, good function can still be achieved despite some residual radiological imperfection when appropriate fixation and rehabilitation strategies are employed. According to the Rasmussen clinical scoring system, the current study shows a steady improvement in functional outcomes after surgical treatment of tibial plateau fractures. The findings demonstrate a distinct pattern of rising Rasmussen scores between 1 month and 6 months, as well as additional improvement at 1 year, suggesting a gradual restoration of knee function over time. Due to pain, soft tissue healing, and limited mobility, early post-operative scores were comparatively lower; nevertheless, as rehabilitation advanced, significant improvement was noted during successive follow-ups. The link between fracture severity and functional result is a significant discovery in this study. In comparison to patients with lower fracture grades, those with greater Schatzker fracture types had comparatively lower Rasmussen ratings at all follow-up periods. This finding lends credence to the generally held belief that increased fracture complexity is linked to more articular disruption, soft tissue damage, and difficulties in attaining anatomical reduction, all of which may have a negative impact on functional recovery. Similarly, in more intricate patterns including several columns, fractures categorised using the Luo three-column classification displayed somewhat lower results. This emphasises how crucial it is to comprehend fracture morphology for surgical planning and prognosis. Patients treated with dual-plate fixation showed somewhat higher Rasmussen scores than those treated with single-plate fixation, according to the fixation methods study [22]. In bicondylar fractures in particular, dual plating improves biomechanical stability, enabling better reduction maintenance and quicker mobilisation. Nonetheless, the clinical scores of the two groups in this study differed very little, indicating that, when paired with careful surgical technique and organised rehabilitation, suitable fracture-specific fixation – regardless of the number of plates used – can produce satisfactory clinical outcomes. Overall, the results of this study highlight that while fracture severity continues to be a significant predictor of prognosis, functional recovery following tibial plateau fracture repair improves dramatically over time. To maximise post-operative knee function, a thorough pre-operative evaluation of the fracture pattern and a suitable repair technique are crucial.
Plate configuration: Single versus dual:
Our cohort’s twin plate designs offered more reliable radiological alignment in bicondylar patterns than single lateral plating, which is consistent with earlier biomechanical and clinical research. The slight but steady change in mean radiological scores over time suggests that DP structures have a long-lasting stability advantage, especially in high-grade injuries. Functionally, the convergence of clinical, IKDC, and KSS scores between the SP and DP groups after a year indicates that both approaches can produce good short-term results with proper case selection (less severe patterns in SP, more complicated in DP). These results confirm earlier findings that, even while single and dual plating differ radiologically, they nonetheless produce comparable functional outcomes, especially when alignment is within allowable bounds.
Limitations of the study:
- The results of this study may not be as applicable to other institutions because it was only carried out at one tertiary care teaching hospital.
- Due to the small sample size, a thorough subgroup analysis across fracture types and fixation structures was not possible.
- The 1-year follow-up period precluded the evaluation of long-term issues such as late implant failure and post-traumatic osteoarthritis.
- Patients were not randomised into fixation groups, introducing potential treatment allocation bias.
- Dual plating was preferred for treating more serious fractures, which could complicate direct comparisons between fixing techniques.
- The results of other fixation techniques, such as external fixation or minimally invasive procedures, were not compared in this study.
- Rasmussen radiological scoring may introduce observer variability since it involves subjective interpretation.
- Functional outcomes may have been influenced by variability in rehabilitation adherence, physiotherapy participation, and patient motivation.
- Variability in fracture morphology and injury severity was introduced by the inclusion of several Schatzker and Luo fracture types.
- Associated soft tissue injuries were not systematically graded or analysed.
- Routine postoperative CT evaluation was not performed to assess subtle residual articular incongruity.
- Weight-bearing progression and rehabilitation protocols were individualised, which may have affected recovery patterns.
- The influence of surgeon experience and technical expertise on outcomes was not assessed. Broader patient-reported quality-of-life measures such as SF-36 or EQ-5D were not included.
- It is possible that late problems such as implant prominence, secondary collapse, and degenerative alterations were missed over the study period.
Complex proximal tibial plateau fractures can be effectively managed using column-based plating that is guided by a combination of Schatzker’s and Luo’s three-column categorisation. When column-specific repair and rehabilitation are improved, fracture severity – represented by higher Schatzker and Luo types – predicts worse radiological restoration but does not always jeopardise 1-year functional outcomes. While functional findings converge over time, DP structures offer a slight but steady advantage over SP in radiological alignment in intricate patterns. To achieve dependable, high-quality results in these difficult situations, surgeons should give priority to early, structured rehabilitation; proper plate configuration; and three-dimensional pre-operative planning. In difficult proximal tibia fractures, column-based plating, guided by Luo’s three-column classification, provides dependable fixation and positive results. While functional recovery is consistently strong across fixation procedures, dual plating produces better radiological findings.
Rasmussen clinical scores gradually improved from 1 month to 1 year after surgical treatment of tibial plateau fractures, indicating a successful functional recovery with suitable stabilisation and rehabilitation. Schatzker and Luo’s classifications of fracture severity demonstrated a negative connection with clinical outcomes, suggesting comparatively lower functional scores in more complex fracture patterns. When used based on fracture morphology, both fixation procedures produced satisfactory clinical results, despite dual-plate fixation showing marginally higher Rasmussen ratings than single-plate fixation. For tibial plateau fractures to have good functional results, careful preoperative fracture assessment, anatomical reduction, and stable fixation are still crucial.
Column-based plating is a biomechanically superior method for complex proximal tibia fractures. Dual plating enhances radiological outcomes, while functional recovery remains satisfactory across fixation strategies.
References
- 1. Wenger D, Petersson K, Rogmark C. Patient-related outcomes after proximal tibial fractures. Int Orthop 2018;42:2925-31. [Google Scholar] [PubMed]
- 2. Ozkaya U, Parmaksizoglu AS. Dual locked plating of unstable bicondylar tibial plateau fractures. Injury 2015;46 Suppl 2:S9-13. [Google Scholar] [PubMed]
- 3. Luo CF, Sun H, Zhang B, Zeng BF. Three-column fixation for complex tibial plateau fractures. J Orthop Trauma 2010;24:683-92. [Google Scholar] [PubMed]
- 4. Wang Y, Luo C, Zhu Y, Zhai Q, Zhan Y, Qiu W, et al. Updated three-column concept in surgical treatment for tibial plateau fractures – a prospective cohort study of 287 patients. Injury 2016;47:1488-96. [Google Scholar] [PubMed]
- 5. Ahearn N, Oppy A, Halliday R, Rowett-Harris J, Morris SA, Chesser TJ, et al. The outcome following fixation of bicondylar tibial plateau fractures. Bone Joint J 2014;96-B:956-62. [Google Scholar] [PubMed]
- 6. Tarng YW, Lin KC. Combined prone and supine approaches for complex three-column tibial plateau fracture with posterolateral articular injury. Injury 2019;50:1756-63. [Google Scholar] [PubMed]
- 7. Lin W, Su Y, Lin CS, Guo WZ, Wu JQ, Wang YY, et al. The application of a three-column internal fixation system with anatomical locking plates on comminuted fractures of the tibial plateau. Int Orthop 2016;40:1509-14. [Google Scholar] [PubMed]
- 8. Krause M, Frosch KH. Change in the treatment of tibial plateau fractures. Unfallchirurgie (Heidelb) 2022;125:527-34. [Google Scholar] [PubMed]
- 9. Yao J, Wang H, Quan S, Feng W, Cai L, Yang M. Posterior popliteal fossa S-shaped incision with double-window approach in treating posterior column of tibial plateau fractures. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 2020;34:574-8. [Google Scholar] [PubMed]
- 10. Wu J, Wang Y, Zhou F, Yang L, Tang J. Trans-articular Kirschner wire fixation in treating complex tibial plateau fractures complicated by multiple ligament injuries: A case report and literature review. Injury 2018;49:382-5. [Google Scholar] [PubMed]
- 11. Liu J, Zhang Y, Zheng Z. Research progress on biomechanics for internal fixation in tibial plateau fracture. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 2024;38:113-8. [Google Scholar] [PubMed]
- 12. Vidović D, Matejčić A, Ivica M, Jurišić D, Elabjer E, Bakota B. Minimally-invasive plate osteosynthesis in distal tibial fractures: Results and complications. Injury 2015;46:S96-9. [Google Scholar] [PubMed]
- 13. Keppler L, Keppler AM, Ihle C, Minzlaff P, Fürmetz J, Beck M, et al. Patients with complex proximal tibial fractures overestimate the prognosis of their injury. Eur J Trauma Emerg Surg 2022;48:1479-86. [Google Scholar] [PubMed]
- 14. Elsoe R, Larsen P, Petruskevicius J, Kold S. Complex tibial fractures are associated with lower social classes and predict early exit from employment and worse patient-reported QOL: A prospective observational study of 46 complex tibial fractures treated with a ring fixator. Strategies Trauma Limb Reconstr 2018;13:25-33. [Google Scholar] [PubMed]
- 15. Menghi A, Mazzitelli G, Marzetti E, Barberio F, D’Angelo E, Maccauro G. Complex tibial plateau fractures: A retrospective study and proposal of treatment algorithm. Injury 2017;48:S1-6. [Google Scholar] [PubMed]
- 16. Subramanyam KN, Tammanaiah M, Mundargi AV, Bhoskar RN, Reddy PS. Outcome of complex tibial plateau fractures with Ilizarov external fixation with or without minimal internal fixation. Chin J Traumatol 2019;22:166-71. [Google Scholar] [PubMed]
- 17. Chang H, Zhu Y, Zheng Z, Chen W, Zhao S, Zhang Y, et al. A meta-analysis shows that highly comminuted bicondylar tibial plateau fractures treated by a single lateral locking plate give similar outcomes to dual-plate fixation. Int Orthop 2016;40:2129-41. [Google Scholar] [PubMed]
- 18. Weaver MJ, Harris MB, Strom AC, Smith RM, Lhowe D, Zurakowski D, et al. Fracture pattern and fixation type related to loss of reduction in bicondylar tibial plateau fractures. Injury 2012;43:864-9. [Google Scholar] [PubMed]
- 19. Jiang R, Luo CF, Wang MC, Yang TY, Zeng BF. A comparative study of the Less Invasive Stabilisation System (LISS) fixation and two-incision double plating for the treatment of bicondylar tibial plateau fractures. Knee 2008;15:139-43. [Google Scholar] [PubMed]
- 20. Yao Y, Lv H, Zan J, Li J, Zhu N, Jing J. Functional outcomes of bicondylar tibial plateau fractures treated with dual buttress plates and risk factors: A case series. Injury 2014;45:1980-4. [Google Scholar] [PubMed]
- 21. Zhang Y, Fan DG, Ma BA, Sun SG. Treatment of complicated tibial plateau fractures with dual plating via a 2-incision technique. Orthopaedics 2012;35:e359-64. [Google Scholar] [PubMed]
- 22. Yi Z, Hui S, Binbin Z, Jianfei T, Huipeng S, Jiong M, et al. A new strategy to fix posterolateral depression in tibial plateau fractures: Introduction of a new modified Frosch approach and a “barrel hoop plate” technique. Injury 2020;51:723-34. [Google Scholar] [PubMed]
- 23. Lin W, Su Y, Lin CS, Guo WZ, Wu JQ, Wang YY, et al. The application of a three-column internal fixation system with anatomical locking plates on comminuted fractures of the tibial plateau. Int Orthop 2016;40:1509-14. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Column Involvement as a Predictor of Early Functional Outcome and Complications in Proximal Tibia Fractures: A Prospective Study
June 1, 2026 Column Involvement as a Predictor of Early Functional Outcome and Complications in Proximal Tibia Fractures: A Prospective Study December 1, 2025 A Prospective Study Comparing the Functional Outcomes of Complex Tibial Plateau Fractures Using Computed Tomography-based Three-column Theory Versus X-Ray-based Schatzker Classification Treated with Open Reduction with Locking Compression Plates
December 1, 2025 A Prospective Study Comparing the Functional Outcomes of Complex Tibial Plateau Fractures Using Computed Tomography-based Three-column Theory Versus X-Ray-based Schatzker Classification Treated with Open Reduction with Locking Compression Plates August 1, 2026 Recurrent Midshaft Clavicle Nonunion with a Large Segmental Bone Defect Treated with Autologous Iliac Crest Bone Graft and Dual Plating: A Case Report
August 1, 2026 Recurrent Midshaft Clavicle Nonunion with a Large Segmental Bone Defect Treated with Autologous Iliac Crest Bone Graft and Dual Plating: A Case Report August 1, 2026 Why the Ilizarov Ring Fixator Remains the Preferred Technique for Knee Arthrodesis in Complex Knee Conditions: A Case Series
August 1, 2026 Why the Ilizarov Ring Fixator Remains the Preferred Technique for Knee Arthrodesis in Complex Knee Conditions: A Case Series