
In complex prosthetic knee infections with multiple sinuses and intramedullary involvement, innovative elastic titanium-reinforced antibiotic spacers enable successful infection eradication and functional restoration even in morbidly obese patients with culture-negative infections.
Dr. Rajesh Pareek, Department of Orthopaedics, Teerthanker Mahaveer Medical College and Research Centre, Moradabad, Uttar Pradesh, India. E-mail: rajyeshpareek@gmail.com
Abstract
Introduction: Chronic prosthetic joint infection (PJI) with intramedullary extension presents exceptional management challenges in morbidly obese patients. This case demonstrates novel elastic titanium pin spacer fabrication for complex infection control. To the best of our knowledge, this is the first reported case combining intramedullary infection extending to the mid-diaphyseal level with an innovative spacer design.
Case Report: A 60-year-old morbidly obese male, 110 kg, with a body mass index of 44 kg/m², presented with chronic PJI, multiple draining sinuses, and wound dehiscence 14 months post-primary TKA. Multiple previous debridements failed to control infection. Intraoperative findings revealed extensive intramedullary infection extending to the mid-diaphyseal level without implant-cement interface involvement. Two-stage revision was performed using an innovative elastic titanium pin (Ti-6Al-4V, 2 mm × 200 mm) technique for spacer fabrication and a comprehensive infection management protocol.
Results: Despite culture-negative infections, the staged surgical approach achieved complete infection eradication. Patient achieved full weight-bearing at 1 month with 0–110° range of motion. At more than a year's follow-up, he remains symptom-free with stable prosthetic components and no recurrent infection.
Conclusion : This case demonstrates successful management of complex PJI with intramedullary extension using a novel elastic titanium pin spacer technique. The unique presentation provides valuable insights for managing similar complex cases in high-risk populations.
Keywords: Prosthetic joint infection, intramedullary infection, elastic titanium pin spacer, morbid obesity, two-stage revision.Prosthetic joint infection, intramedullary infection, elastic titanium pin spacer, morbid obesity, two-stage revision.
Prosthetic joint infection (PJI) complicates 12% of primary total knee arthroplasties but represents one of the most devastating complications with significant morbidity [1]. Chronic PJI with multiple draining sinuses indicates established biofilm formation and extensive soft-tissue compromise [2]. The presence of intramedullary infection extending to diaphyseal levels represents an uncommon variant requiring specialised management approaches. Morbid obesity with a body mass index (BMI) of ≥40 kg/m² significantly compounds PJI management complexity through impaired immune response, compromised wound healing, and increased mechanical stresses [3]. Two-stage revision remains the gold standard for chronic PJI management with infection eradication rates of 78–85%, though success rates decrease significantly in morbidly obese patients [4]. This case presents extensive intramedullary infection, innovative elastic titanium pin spacer fabrication, and a successful staged surgical approach following multiple failed interventions.
Patient demographics and history:
A 60-year-old morbidly obese male (weight 110 kg, BMI 44 kg/m²) presented to our tertiary centre with a chronic right knee infection following primary total knee arthroplasty (TKA) performed 14 months previously. The patient had undergone multiple debridement procedures at the index surgery centre, including an unusual transverse medial incision approach, yet infection remained uncontrolled.
Clinical presentation:
The patient presented with complete inability to bear weight, severe persistent pain, and multiple purulent draining sinuses extending proximally to the tibial level. Physical examination revealed extensive wound dehiscence, multiple active sinus tracts with copious pus discharge, surrounding tissue induration, and complete loss of knee function (Fig. 1). The patient was afebrile but showed signs of chronic illness.

Figure 1: Clinical photograph showing multiple draining sinuses with purulent discharge and extensive wound dehiscence around the right knee with tissue involvement extending proximally to the tibial level.
Investigations:
Laboratory investigations demonstrated elevated inflammatory markers: Erythrocyte sedimentation rate (ESR) 94 mm/h, C-reactive protein (CRP) 16.8 mg/L, and leukocytosis 13,200/μL. Multiple pre-operative cultures from sinus drainage showed no bacterial growth. Radiographic evaluation revealed complete loosening of both femoral and tibial components with extensive peri-prosthetic osteolysis (Fig. 2).
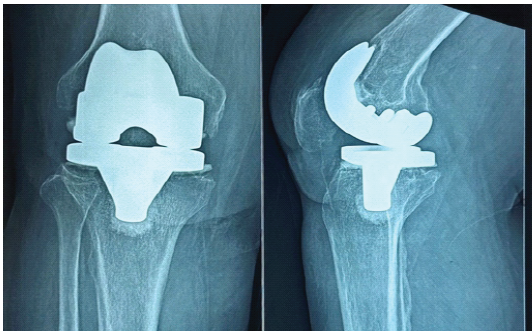
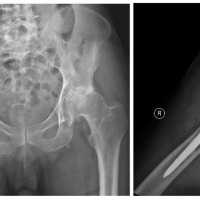
Figure 2: Pre-operative radiographs (AP and lateral views) showing right total knee arthroplasty with complete loosening of prosthetic components and extensive peri-prosthetic osteolysis indicating chronic infection.
First-stage surgical management:
Infected implant removal and debridement:
The patient underwent comprehensive infected implant removal through an extensive approach. During removal, a unique finding was the complete absence of pus at the implant-cement interface and cement-bone interface, contrary to typical PJI presentations. However, extensive intramedullary pus was discovered extending to mid-diaphyseal levels in both femoral and tibial canals, presenting significant challenges for thorough debridement.
Meticulous debridement of all necrotic and fibrous tissue with pus was performed, followed by extensive pulse lavage irrigation. Multiple tissue and bone cultures were obtained but remained negative for bacterial growth.
Innovative spacer fabrication:
An articulated antibiotic cement spacer was fabricated using cement moulds for femoral and tibial components. Uniquely, an elastic titanium pin (Ti-6Al-4V alloy, 2 mm diameter, 200 mm length) was incorporated for the intramedullary cement spacer component in the tibia for enhanced infection control and mechanical stability. The spacer was loaded with vancomycin (4 g), gentamicin (2.4 g), and clindamycin (1.2 g) per 80 g of cement.
Wound management challenges:
The medial transverse wound from previous surgery could not be closed in a tension-free manner, necessitating application of stay sutures with drain placement (Fig. 3). This represented a significant soft-tissue management challenge in the morbidly obese patient with compromised tissue quality.

Figure 3: Clinical photograph showing innovative wound management after first-stage procedure. Retention sutures are strategically placed to reduce tension on the primary suture line, essential for the compromised tissue quality in this morbidly obese patient. A closed-suction drain is positioned subfascially to prevent fluid collection and monitor for residual infection.
Post-operative management, first stage:
Empirical intravenous antibiotics (Clindamycin and Piperacillin-Tazobactam) were administered for 8 weeks while monitoring infection control parameters. Serial inflammatory markers showed progressive improvement with CRP decreasing to 4.2 mg/L and ESR to 38 mm/h. Post-operative radiographs demonstrated appropriate spacer positioning with maintenance of joint space and alignment (Fig. 4).

Figure 4: Post-operative radiographs showing articulating antibiotic cement spacer with molded femoral and tibial components. The spacer features intramedullary stems extending to mid-diaphyseal level, with the tibial component incorporating the novel elastic titanium pin (Ti-6Al-4V, 2 mm × 200 mm) for enhanced stability.
Staged wound closure:
After 8 weeks, on confirming infection control, the medial wound was addressed through a staged approach. Wound margins were refreshed, and fibrous tissue was excised to a bone-deep level, enabling tension-free wound closure.
Second-stage surgical management:
Timing and preparation:
Four weeks following medial wound closure and after confirmation of infection control through normalised inflammatory markers (CRP < 0.5 mg/L, ESR < 25 mm/h), the patient underwent second-stage reimplantation.
Spacer removal challenges:
During second-stage surgery, significant complications were encountered with spacer removal. The femoral spacer component had fragmented into multiple pieces and migrated, while the intramedullary spacer was broken and separated from the tibial base plate spacer near the keel junction. These broken spacer components required specialised removal techniques using osteotomes and careful dissection.
Reimplantation procedure:
All fibrous tissue was meticulously removed, and the dermal layer was mobilised to reduce wound volume, enabling tension-free closure after reimplantation. A progressive constrained kinematics revision TKA with stemmed components was implanted after extensive pulse lavage. Tissue cultures and biopsies were obtained intraoperatively. Immediate post-operative radiographs showed excellent component positioning (Fig. 5).
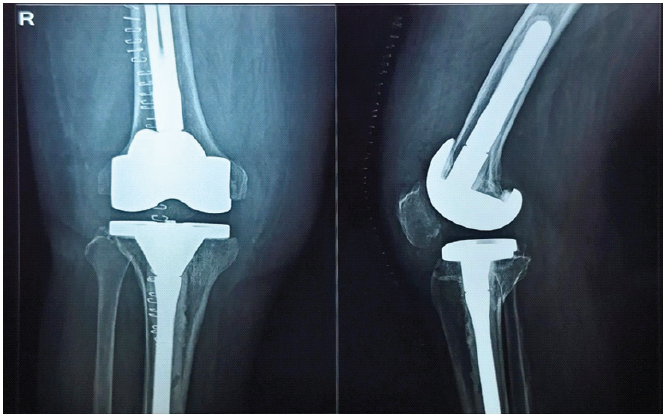
Figure 5: Post-operative radiographs following second-stage reimplantation showing well-positioned revision total knee arthroplasty with stemmed components, restored joint line, and proper alignment.
Post-operative course, second stage:
The patient received empirical intravenous antibiotics for 2 weeks. The perioperative period was complicated by fever and urinary tract infection with Escherichia coli, requiring adjustment of antibiotic therapy based on culture sensitivity reports. Wound healing progressed satisfactorily with suture removal at 2 weeks.
Rehabilitation and outcome:
The patient became symptom-free at 1 month and achieved full weight-bearing after 1 month of physiotherapy. At more than a year’s follow-up, he remains completely symptom-free with the ability to perform activities of daily living independently. Range of motion (ROM) achieved was 0–120°, and radiographs showed stable prosthetic components with excellent bone-implant integration and no evidence of recurrent infection (Fig. 6).
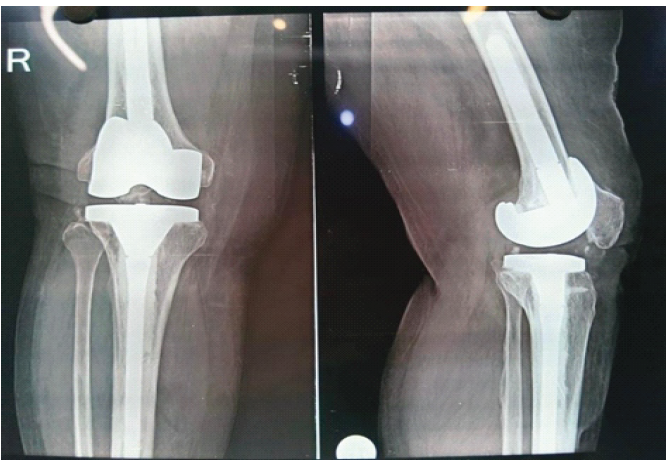
Figure 6: Follow-up radiographs at >1 year showing stable prosthetic components with excellent bone-implant integration, maintained joint alignment, intact cement mantles, and no evidence of component loosening, osteolysis, or radiographic signs of recurrent infection. Additional figures as per journal discretion – Separate AP and lateral view pictures post 1-year follow-up.
Intramedullary infection presentation:
The unusual presentation of extensive intramedullary pus extending to mid-diaphyseal levels without involvement of the implant-cement interface represents a rare variant of chronic PJI [5]. This finding suggests haematogenous seeding or retrograde infection through medullary canals, requiring specialised debridement techniques to prevent contamination spread.
Innovative spacer fabrication:
Conventional antibiotic cement spacers have reported failure rates of 10–20% in modern series [6]. The incorporation of elastic titanium pins represents a novel approach for managing intramedullary infection [7]. This technique provides mechanical reinforcement while maintaining antibiotic delivery capacity. The elastic properties of titanium pins reduce stress concentration and fracture risk compared to rigid reinforcement methods, while their superior magnetic resonance imaging compatibility enables artefact-free imaging for infection monitoring.
Staged wound management approach:
The innovative staged approach to wound closure in this morbidly obese patient demonstrates the importance of tissue quality optimisation before definitive closure [8]. The 8-week interval allowed for infection control and tissue conditioning, enabling tension-free closure and preventing wound dehiscence complications common in obese patients.
Management of culture-negative PJI:
Despite multiple culture attempts, all specimens remained negative for bacterial growth. This occurs in 7–39% of PJI cases and requires empirical broad-spectrum antibiotic coverage based on clinical presentation [9]. The presence of multiple draining sinuses provided a definitive diagnosis according to musculoskeletal infection society criteria.
Literature comparison:
The success rate achieved in this case aligns with reported two-stage revision outcomes of 78–85% infection eradication, despite the high-risk patient profile and complex presentation [10]. The functional outcome (0–120° ROM) compares favourably with literature reports showing significant improvements in knee function following successful two-stage revision.
Limitations:
This single-case report has inherent limitations, including short-term follow-up (approximately 13 months), inability to provide comparative data with conventional spacers, and need for larger cohort validation of the elastic titanium pin technique. Long-term durability and cost-effectiveness analysis require further investigation and biomechanical studies.
This case demonstrates successful management of an exceptionally complex chronic PJI with intramedullary extension using innovative surgical techniques in a morbidly obese patient. Key success factors included recognition of unusual infection patterns, innovative elastic titanium pin spacer fabrication, a staged wound management approach, comprehensive infection control protocols, and management of spacer-related complications. The case contributes novel insights to orthopaedic literature: the first description of extensive intramedullary PJI management using the elastic titanium pin spacer technique, demonstration of a successful staged wound closure approach in morbidly obese patients, and a comprehensive management protocol for complex PJI cases following multiple failed interventions.
Complex prosthetic joint infections with intramedullary extension can be successfully managed using innovative spacer fabrication techniques and staged surgical approaches, even in morbidly obese patients following multiple failed treatments.
References
- 1. Tande AJ, Patel R. Prosthetic joint infection. Clin Microbiol Rev 2014;27:302-45. [Google Scholar] [PubMed]
- 2. Jung J, Schmid NV, Kelm J, Schmitt E, Anagnostakos K. Complications after spacer implantation in the treatment of hip joint infections. Int J Med Sci 2009;6:265-73. [Google Scholar] [PubMed]
- 3. Boyce L, et al. [TPS1.1]. The outcomes of total knee arthroplasty in morbidly obese patients. Bone Joint J 2019;101-B:126-35. [Google Scholar] [PubMed]
- 4. Mahmud T, Lyons MC, Naudie DD, Macdonald SJ, McCalden RW. Assessing the gold standard: A review of 253 two-stage revisions for infected TKA. Clin Orthop Relat Res 2012;470:2730-6. [Google Scholar] [PubMed]
- 5. Davis B, et al[TPS2.1]. Management of periprosthetic hip and knee joint infections with sinus tracts. J Arthroplasty 2021;36:2055-9. [Google Scholar] [PubMed]
- 6. Citak M, et al. [TPS3.1]. Dynamic versus static cement spacer in periprosthetic knee infection: A meta-analysis. Arch Orthop Trauma Surg 2015;135:695-707. [Google Scholar] [PubMed]
- 7. Chou DT, et al. [TPS4.1]. A method of fabricating an antibiotic cement spacer using an elastic nail for the treatment of intramedullary osteomyelitis. Open Orthop J 2015;9:60-2. [Google Scholar] [PubMed]
- 8. Rajani AM, Thakkar CJ, Shah UA, Punamiya M. Retention stitches: A concept of wound closure of knee arthroplasty in obese patients. Indian J Orthop 2022;56:1048-52. [Google Scholar] [PubMed]
- 9. Ayoade F, Kumar A. Periprosthetic joint infection. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2023. [Google Scholar] [PubMed]
- 10. Bourgonjen YP, et al. [TPS5.1]. Long-term outcome of two-stage revision surgery after hip and knee prosthetic joint infection. Bone Joint J 2021;103-B:1537-45. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 October 10, 2023 Two-stage Partial Component Retention and Interim Cemented Liner for Infected Total Hip Arthroplasty: A Case Report
October 10, 2023 Two-stage Partial Component Retention and Interim Cemented Liner for Infected Total Hip Arthroplasty: A Case Report July 1, 2026 Bone Morphogenetic Proteins-2–Augmented Acetabular Bone Stock Restoration During Two-stage Revision for Periprosthetic Joint Infection: A Case Report
July 1, 2026 Bone Morphogenetic Proteins-2–Augmented Acetabular Bone Stock Restoration During Two-stage Revision for Periprosthetic Joint Infection: A Case Report June 1, 2026 Revision of a Dislocated Articulating Antibiotic Hip Spacer as an Alternative to Girdlestone Arthroplasty: A Case Report
June 1, 2026 Revision of a Dislocated Articulating Antibiotic Hip Spacer as an Alternative to Girdlestone Arthroplasty: A Case Report June 1, 2026 A Rare Case of Salmonella Typhimurium Prosthetic Joint Infection in Total Hip Arthroplasty in a Young Patient with Long-term Corticosteroid Therapy
June 1, 2026 A Rare Case of Salmonella Typhimurium Prosthetic Joint Infection in Total Hip Arthroplasty in a Young Patient with Long-term Corticosteroid Therapy