
Thorough diagnostic evaluations and a multidisciplinary approach are essential for accurately diagnosing and effectively treating angiofibroma of soft tissue, especially in atypical presentations.
Dr Madhan Jeyaraman, Department of Orthopaedics, ACS Medical College and Hospital, Dr MGR Educational and Research Institute, Chennai, Tamil Nadu, India. E-mail: madhanjeyaraman@gmail.com
Abstract
Introduction: Angiofibroma of soft tissue (AFST) is a rare benign neoplasm characterised by distinctive histopathological and genetic features. It commonly arises in the lower extremities but can present in atypical locations, complicating diagnosis.
Case Report: A 77-year-old male with a 10-year history of bilateral knee pain and 6-month history of right knee swelling was examined. Physical assessment revealed bilateral knee varus deformity and a palpable, variable-consistency mass in the anteromedial aspect of the right knee. Radiographs indicated severe osteoarthritis and soft-tissue swelling. Magnetic resonance imaging showed cystic collections consistent with a ganglion cyst. Surgical excision exposed a superficial cystic mass and a deeper firm mass, confirmed histopathologically as a ganglion cyst and AFST, respectively. Immunohistochemical tests were negative for epithelial membrane antigen, S-100, and Vimentin. The patient is under regular follow-up with no recurrence in the last 12 months.
Conclusion: AFST should be included in the differential diagnosis of soft-tissue masses. Comprehensive diagnostic evaluations, including detailed imaging and histopathological analysis, are crucial for accurate diagnosis. Surgical excision is effective, with a favourable prognosis and low recurrence risk.
Keywords: Angiofibroma, knee, ganglion cyst.
Angiofibroma of soft tissue (AFST) is an infrequent benign neoplasm with distinctive histological and genetic characteristics [1]. Initially characterised by Mariño-Enríquez and Fletcher in 2012, AFST predominantly arises in the deep soft tissues of the lower extremities, displaying a predilection for middle-aged adults with a slight female predominance [2]. Despite its benign nature, AFST’s clinical and radiological presentations can often mimic other benign and low-grade malignant soft-tissue tumours, necessitating thorough diagnostic scrutiny [3]. The characteristic histopathological features of AFST include a proliferation of uniform spindle cells within a myxoid to collagenous stroma, accompanied by a prominent vascular network [4,5]. Cytogenetically, AFST frequently exhibits a balanced t(5;8) (p15;q13) translocation, resulting in the fusion of the aryl hydrocarbon receptor repressor and nuclear receptor coactivator 2 genes, a hallmark that aids in its definitive diagnosis [1]. While AFST predominantly affects the lower extremities, cases involving atypical locations such as intra-articular spaces have been documented [1,4]. These cases underscore the tumour’s potential for diverse anatomical presentations, complicating the clinical differential diagnosis. Radiologically, AFSTs typically present as well-defined masses with iso- to slightly hypointense signals on T1-weighted magnetic resonance imaging (MRI) sequences and hyperintense signals on T2-weighted sequences, with variable enhancement patterns on contrast studies [6,7]. However, these features are not exclusive to AFST and can overlap with other soft-tissue neoplasms, further emphasising the need for histopathological and molecular confirmation. In the present case report, we discuss a rare presentation of bilateral knee pain and swelling in a 77-year-old male patient, with a specific focus on the right knee, which exhibited a soft-tissue mass.
A 77-year-old male presented with bilateral knee pain for 10 years and swelling of the right knee for 6 months. The patient was unable to stand and walk for a prolonged period. He has been a known case of chronic kidney disease for 2 years. On examination, bilateral knee varus deformity of 20° on both knees. The swelling was present in the anteromedial aspect of the right knee, which started with the size of a peanut and gradually attained the size of a ball of volume 5 × 3 × 2 cm, approximately. The consistency varied from soft to firm in the different areas of the swelling. The skin above the swelling was pinchable. The swelling has a positive cross-fluctuation test and is non-transilluminant in nature. The radiographic examination of bilateral knees in a standing position revealed Kellgren-Lawrence Grade IV knee osteoarthritis with 20° of genu varus deformity over both knees along with a soft-tissue swelling noticed in the medial aspect of the right knee (Fig. 1).

Figure 1: Plain radiograph of right knee (AP and Lateral) showing Grade IV knee osteoarthritis along with soft-tissue swelling over the medial aspect of the right knee.
MRI of the right knee revealed a cystic collection in the right anteromedial knee – subcutaneous plane, measuring 7.6 × 4 × 2.8 cm in size, with the contents appearing hypointense in T1W images and hyperintense in T2W images. There was an encysted collection with multiple septations seen in the medial knee joint level, measuring approximately 4.9 × 4.7 × 2.0 cm, adjoining the collateral ligament content, appearing hypointense in T1W images and hyperintense in T2W images with the possibility of a ganglion cyst (Fig. 2).
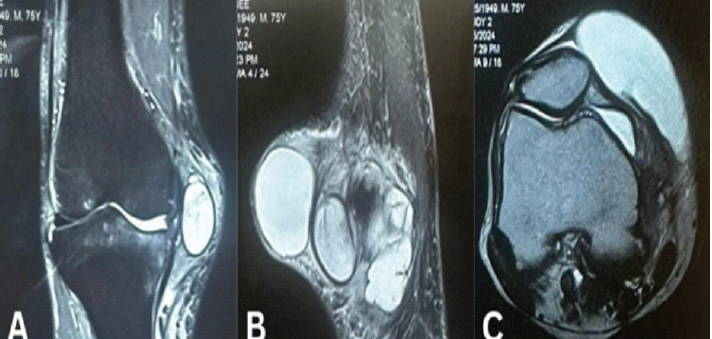
Figure 2: T2W-magnetic resonance imaging of right knee (a) coronal and (c) axial view showing superficial ganglion cyst (7.6 × 4 × 2.8 cm) and (b) sagittal view showing both superficial ganglion cyst (7.6 × 4 × 2.8 cm) and deep angiofibroma of knee (4.9 × 4.7 × 2.0 cm).
The patient was counselled for surgical excision, where intraoperatively, the mass appeared to be adhered to the underlying knee joint. Both masses were removed in toto and sent for histopathological examination. The gross examination of the superficial swelling appeared to be a cystic swelling of 5 × 3 × 2 cm with synovial fluid as its content, and the deep swelling appeared to be a firm swelling of 4 × 3 × 2 cm with areas of necrosis and haemorrhage. Histopathological examination of the superficial mass revealed a cyst wall lined by flattened cuboid cells admixed with fibro-collagenous tissue with focal myxoid areas and multiple congested blood vessels with areas of haemorrhage suggestive of a ganglion cyst, whereas the deep swelling revealed a cyst wall lined by flattened cuboid cells with underlined stroma showing fibro-myxoid changes and focal chondroid areas with the collection of stellate cells with dark-staining nuclei and scant eosinophilic cytoplasm with proliferating blood vessels and few multinucleated giant cells suggestive of an angiofibroma (Fig. 3). The immunohistochemical markers of epithelial membrane antigen (EMA), S-100, and Vimentin were found to be negative. The patient is under regular follow-up for 12 months (Fig. 4).

Figure 3: (a) (×10) and (b) (×40) showing cyst wall lined by flattened cuboid cells with fibro-myxoid changes and focal chondroid areas with few multinucleated giant cells along with proliferating vascular changes suggestive of angiofibroma.
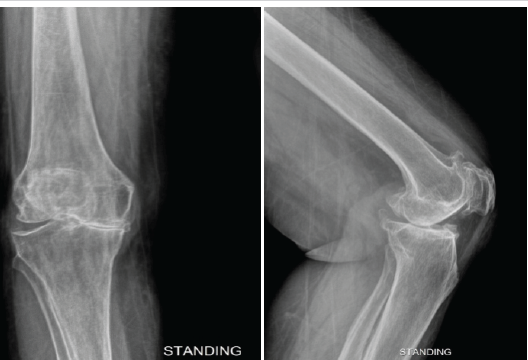
Figure 4: A 1-year follow-up radiograph of right knee showing no recurrence of angiofibroma.
AFST is a rare benign neoplasm, primarily identified in the lower extremities and characterised by distinctive histopathological and genetic features. Since its initial description by Mariño-Enríquez and Fletcher in 2012, AFST has been recognised for its unique presentation, typically affecting middle-aged adults with a slight female predominance [2]. This discussion aims to elucidate the clinical, radiological, and histopathological features of AFST, especially focusing on cases involving the knee joint, as summarised in Table 1.
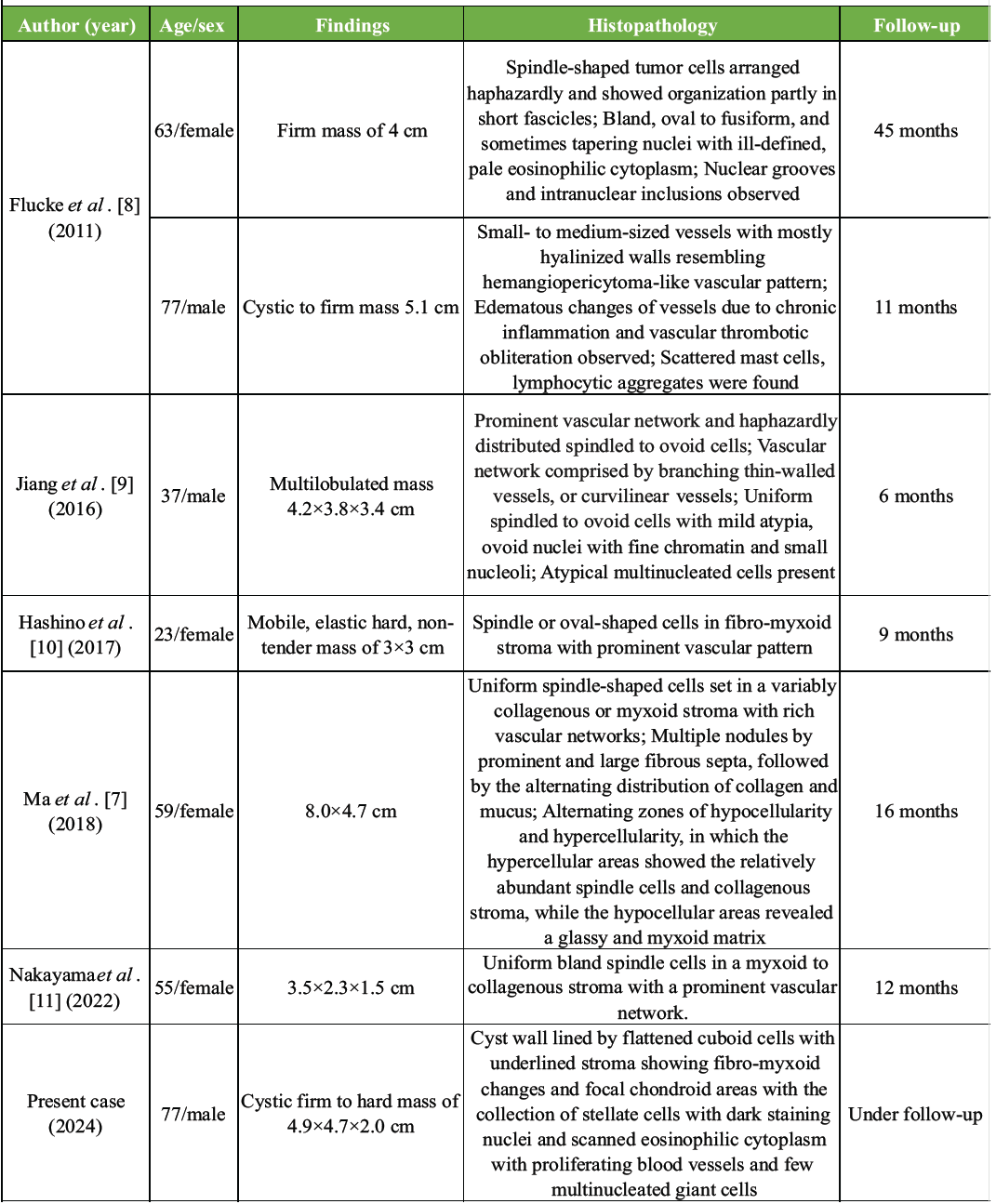
Table 1: The available evidence of knee angiofibroma
The current case report of a 77-year-old male with bilateral knee pain and a complex mass in the right knee provides further insight into the variability and diagnostic challenges associated with AFST. The patient presented with a long history of bilateral knee pain and recent swelling in the right knee. Chronic kidney disease and a significant varus deformity further complicated the clinical picture. Such presentations are not uncommon in elderly patients, making the differential diagnosis extensive and challenging. Initial radiographs revealed severe osteoarthritis and a notable soft-tissue mass, while MRI provided detailed imaging, highlighting cystic collections suggestive of a ganglion cyst. This initial diagnosis underscored the importance of comprehensive imaging studies in characterising soft-tissue masses and guiding further diagnostic procedures. Radiologically, AFST typically presents as a well-defined mass with variable signal characteristics on MRI. In our case, the MRI findings included a cystic collection with multiple septations and varying signal intensities on T1 and T2-weighted images. These features, while indicative of a ganglion cyst, are not exclusive and highlight the overlapping radiological characteristics of AFST with other soft-tissue neoplasms. Previous case reports, such as those summarised in Table 1, also demonstrate similar MRI findings, emphasising the role of detailed imaging in the initial assessment and differential diagnosis of knee masses. Histopathological examination remains the gold standard for diagnosing AFST. In our case, the superficial mass was identified as a ganglion cyst, while the deeper mass exhibited histological features consistent with AFST. These included a cyst wall lined by flattened cuboid cells, fibro-myxoid stroma, focal chondroid areas, stellate cells with dark-staining nuclei, and proliferating blood vessels with few multinucleated giant cells. Immunohistochemical markers such as EMA, S-100, and vimentin were negative, aligning with the typical profile of AFST. This comprehensive histopathological evaluation is crucial in distinguishing AFST from other benign and malignant soft-tissue tumours. Table 1 provides a summary of various reported cases of knee angiofibroma, illustrating the diverse histopathological presentations and clinical outcomes. For instance, Flucke et al. [8] reported a firm mass with spindle-shaped tumour cells and a vascular pattern resembling haemangiopericytoma, while Jiang et al. described a multilobulated mass with a prominent vascular network and mild cellular atypia. These cases underscore the heterogeneity of AFST and the importance of detailed histopathological analysis in confirming the diagnosis. The current case report adds to the existing literature by presenting a unique instance of AFST in an elderly male with chronic kidney disease and bilateral knee deformities. Comparative analysis with previous reports reveals several common features, such as the presence of spindle cells, myxoid stroma, and prominent vascular networks. However, the current case also exhibited unique characteristics, including focal chondroid areas and stellate cells, which have been less commonly reported. Flucke et al. [8] described a 63-year-old female and a 77-year-old male with firm and cystic masses, respectively, highlighting the variability in tumour consistency and histological features. The presence of hyalinised vessels and chronic inflammation observed in these cases parallels the findings in our patient, suggesting a potential spectrum of histopathological changes in AFST. Jiang et al. [9] reported a 37-year-old male with a multilobulated mass, emphasising the prominent vascular network and mild cellular atypia, which aligns with the vascular features observed in our case. The presence of atypical multinucleated cells in Jiang’s report further underscores the histopathological diversity of AFST. Hashino et al. [10] described a 23-year-old female with a mobile, non-tender mass characterised by spindle or oval-shaped cells in a fibro-myxoid stroma. This case demonstrates the benign nature of AFST and its relatively straightforward histological presentation, contrasting with the more complex features observed in our patient. Ma et al. [7] and Nakayama et al. [11] further contribute to the understanding of AFST by documenting cases with significant histological diversity, including uniform spindle cells, collagenous or myxoid stroma, and rich vascular networks. These reports highlight the importance of considering AFST in the differential diagnosis of knee masses, particularly in cases with atypical or complex histological features. Surgical excision remains the treatment of choice for AFST, with a favourable prognosis and low recurrence rates. In our case, both the superficial and deep masses were successfully excised, and the patient is currently under regular follow-up with no signs of recurrence in the last 12 months. Previous reports, as summarised in Table 1, also demonstrate successful outcomes following surgical excision, with follow-up periods ranging from 6 to 45 months. The benign nature of AFST and its low potential for malignant transformation underscore the importance of early and accurate diagnosis. Histopathological and immunohistochemical analyses are critical in confirming the diagnosis and guiding appropriate treatment. In cases with complex or atypical presentations, as illustrated by our patient, a multidisciplinary approach involving radiologists, pathologists, and orthopaedic surgeons is essential for optimal management.
Comprehensive diagnostic evaluations, including radiological and histopathological analyses, were crucial in identifying the coexistence of a ganglion cyst and AFST. This case emphasises the importance of considering AFST in the differential diagnosis of soft-tissue masses, the need for thorough histopathological examination, and a multidisciplinary approach to ensure accurate diagnosis and effective treatment. Continued documentation and research on AFST will enhance our understanding and management of this rare tumour.
- Accurate diagnosis of AFST requires comprehensive radiological and histopathological analyses due to its rarity and diverse presentations
- Successful management through surgical excision and ongoing follow-up ensures a favourable prognosis.
References
- 1. Wang C, Fan Y, Wei J, Xu Q, Ru G, Zhao M. Angiofibroma of soft tissue: A clinicopathological study of eight cases with emphasis on the diagnostic utility of fluorescence in situ hybridisation detection for NCOA2 rearrangement. Front Oncol 2022;12:900411. [Google Scholar] [PubMed]
- 2. Mariño-Enríquez A, Fletcher CD. Angiofibroma of soft tissue: Clinicopathologic characterisation of a distinctive benign fibrovascular neoplasm in a series of 37 cases. Am J Surg Pathol 2012;36:500-8. [Google Scholar] [PubMed]
- 3. Ohshika S, Saruga T, Ogawa T, Ono H, Ishibashi Y. Distinction between benign and malignant soft tissue tumours based on an ultrasonographic evaluation of vascularity and elasticity. Oncol Lett 2021;21:281. [Google Scholar] [PubMed]
- 4. Ali Z, Anwar F. Angiofibroma of soft tissue: A newly described entity; a case report and review of literature. Cureus 2019;11:e6225. [Google Scholar] [PubMed]
- 5. Yamada Y, Yamamoto H, Kohashi K, Ishii T, Iura K, Maekawa A, et al. Histological spectrum of angiofibroma of soft tissue: Histological and genetic analysis of 13 cases. Histopathology 2016;69:459-69. [Google Scholar] [PubMed]
- 6. Xiao L, Yang L, Wang Y, Li L. Angiofibroma of soft tissue on MRI and FDG PET/CT image. Clin Nucl Med 2022;47:e315-7. [Google Scholar] [PubMed]
- 7. Ma HJ, Huang HN, Li L, Chen S, Zhang RY. Clinicopathological characteristics of angiofibroma of soft tissue: Report of three cases. Int J Clin Exp Pathol 2018;11:3777-84. [Google Scholar] [PubMed]
- 8. Flucke U, Van Krieken JH, Mentzel T. Cellular angiofibroma: Analysis of 25 cases emphasizing its relationship to spindle cell lipoma and mammary-type myofibroblastoma. Mod Pathol 2011;24:82-9. [Google Scholar] [PubMed]
- 9. Jiang GY, Fan F, Dai SD, Yu JH, Wang EH, Lin XY. Angiofibroma of soft tissue: Report of two cases and review of literature. Int J Clin Exp Pathol 2016, 9:4545–54. [Google Scholar] [PubMed]
- 10. Hashino Y, Nishio J, Maeyama A, Aoki M, Nabeshima K, Yamamoto T. Intra-articular angiofibroma of soft tissue of the knee: A case report. Mol Clin Oncol 2017;7:229-32. [Google Scholar] [PubMed]
- 11. Nakayama S, Nishio J, Nagao S, Aoki M, Nabeshima K, Yamamoto T. Arthroscopic Excision of intra-articular AHRR-NCOA2-positive angiofibroma of soft tissue of the knee: A case report. Cancer Diagn Progn 2022;2:592-7. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 The Boba Tea Sign: A Novel Magnetic Resonance Imaging Finding in Synovial Chondromatosis of the Knee – A Case Report
August 1, 2026 The Boba Tea Sign: A Novel Magnetic Resonance Imaging Finding in Synovial Chondromatosis of the Knee – A Case Report August 1, 2026 Intra-articular Ganglionic Cysts of Knee: A Cause for Anterior Knee Pain
August 1, 2026 Intra-articular Ganglionic Cysts of Knee: A Cause for Anterior Knee Pain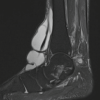 May 1, 2026 Giant Ganglion Cyst of the Tibialis Anterior Tendon Presenting with Adult-Acquired Flatfoot Deformity: A Case Report
May 1, 2026 Giant Ganglion Cyst of the Tibialis Anterior Tendon Presenting with Adult-Acquired Flatfoot Deformity: A Case Report May 1, 2026 Simultaneous Anterior Cruciate Ligament Avulsion Fracture with Bilateral Posterior Meniscal Root Tears of the Knee: A Case Report
May 1, 2026 Simultaneous Anterior Cruciate Ligament Avulsion Fracture with Bilateral Posterior Meniscal Root Tears of the Knee: A Case Report