
Although gender has no impact, older age and a longer duration of osteoarthritis significantly increase the risk of Complex Regional Pain Syndrome, an early post-operative complication following total knee arthroplasty that typically presents within weeks of surgery and becomes uncommon after 3 months under the Budapest criteria, highlighting the need for early recognition and close follow-up.
Dr. Sandeep Vellarakkat, Department of Orthopaedics, Malabar Medical College Hospital and Research Centre, Ulliyeri, Kozhikode, Kerala, India. E-mail: dr.sandeep.v@gmail.com
Abstract
Introduction: Osteoarthritis is a degenerative joint disease commonly affecting the knee, especially the medial compartment, causing cartilage loss, joint space narrowing, deformity, and limited mobility. Radiological severity is graded by the Kellgren–Lawrence system. Advanced or tricompartmental disease requires total knee arthroplasty (TKA). Complex regional pain syndrome (CRPS) is a rare but recognized complication following TKA.
Objectives: The objective of the study was to determine the proportion of patients developing CRPS after TKA and to assess factors associated with its development.
Materials and Methods: This prospective observational study was conducted at a tertiary care center and included 110 patients undergoing primary TKA. Patients were followed up at 2 weeks, 6 weeks, and 12 weeks postoperatively. CRPS was diagnosed clinically using the Budapest criteria. Quantitative variables were expressed as mean and standard deviation, while qualitative variables were presented as frequencies and percentages. Associations were assessed using the Chi-square test, with P < 0.05 considered statistically significant.
Results: The incidence of CRPS was 19.1% at 2 weeks, 9.1% at 6 weeks, and 1.8% at 12 weeks postoperatively. Increasing age and longer duration of osteoarthritis (OA) symptoms showed a statistically significant association with the development of CRPS.
Conclusion: The study found a high initial proportion of CRPS at 2 weeks post-TKA, which declined progressively by 12 weeks, indicating that CRPS is an early but largely transient complication when diagnosed by the Budapest criteria. Advancing age and a longer duration of pre-operative OA symptoms were identified as significant factors associated with its development, whereas gender showed no significant correlation. After 3 months of follow-up, CRPS was found to be uncommon following TKA.
Keywords: Osteoarthritis, total knee arthroplasty, complex regional pain syndrome, Budapest criteria.
Total knee arthroplasty (TKA) is considered the most prevalent therapy for end-stage knee osteoarthritis (OA). TKA is also a prudent option for several other underlying conditions, including inflammatory arthritis, fracture (post-traumatic OA and/or malformation), dysplasia, and malignancy [1]. An arthroplasty involves rebuilding a sick, damaged, or ankylosed joint. This can be accomplished via natural component change, synthetic substitutes, or a combination of the two. A TKA involves the removal of abnormal knee articular surfaces, with metal and polyethylene components being used largely to resurface the knee [1]. Complex regional pain syndrome (CRPS) is the term most frequently employed to characterise a variety of signs and symptoms associated with an enhanced pain response following trauma. The terms ‘reflex sympathetic dystrophy’ and ‘Sudeck’s atrophy’ were used before the classifications ‘Type I CRPS’ (occurring without known nerve damage) and ‘Type II CRPS’ (which takes place when an identified nerve lesion exists) were established [2]. It is associated with severe discomfort and impairment. It is thought to arise and persist due to a harmful proinflammatory response, disturbance in sympathetically mediated vasomotor activity, and changes in both peripheral and central neuronal plasticity [3]. Although its precise aetiology is unidentified, ideas include abnormalities in central sensory-motor processing and how it interacts with the peripheral and parasympathetic nervous systems [2]. The International Association for the Study of Pain (IASP) published the first CRPS diagnostic criteria in 1994. At a conference in Budapest in 2004, the worldwide association for the study of pain adopted new standards. These requirements are now followed globally, replacing the previous ones that had been introduced in the decade prior. These requirements were called the Budapest Criteria. CRPS is an excessively elevated physiological response to injury. According to the little information available, stiffness is the most typical symptom, and knee injuries are assumed to invariably affect the patellofemoral joint. The Budapest clinical criteria maintained the excellent sensitivity of the IASP criteria (0.99) while greatly increasing the specificity (0.68) using a variety of indications and symptoms to evaluate the presence of CRPS following surgery or trauma [4]. The rationale for conducting this study was driven by the need to address a significant gap in clinical data regarding post-operative complications in the Indian population. While TKA is the standard treatment for end-stage OA, CRPS remains a poorly understood but debilitating complication that can severely hinder rehabilitation. The researchers identified a lack of regional literature on CRPS following TKA and sought to provide clarity amidst conflicting global data; previous studies often reported vastly different incidence rates depending on the diagnostic standards used. By employing the modern Budapest Criteria, which balances high sensitivity with improved specificity, the study aimed to establish a more accurate clinical baseline. Furthermore, by identifying specific risk factors such as age and the duration of pre-operative symptoms, the study provides a foundation for early recognition and targeted multidisciplinary management, ultimately aiming to reduce long-term morbidity and improve functional outcomes for high-risk patients.
Objectives of the study:
- To determine the proportion of patients developing CRPS
- To assess the factors associated with the development of CRPS.
This research was designed as a longitudinal study conducted within the Department of Orthopaedics at Malabar Medical College Hospital and Research Centre. The study spanned a duration of 18 months, from January 2023 to June 2024. Institutional Ethics Committee approval was obtained on January 05, 2023, vide reference number MMCH&RC/IEC/2022/24. The sample size was calculated based on a previously reported CRPS prevalence of 62.7% at 6 weeks post-surgery [5]. Using a formula for a single proportion with a 95% confidence level (Z = 1.96) and a relative precision of 15% of the prevalence, the required sample size was determined to be 106. To account for potential loss to follow-up, 110 patients were included for the study.
Inclusion criteria:
- All patients presented to the Orthopaedic department, Malabar Medical College Hospital and Research Centre, undergoing unilateral TKA
- Those who are willing to participate in the study
- Those who are willing for regular follow-up in postoperative rehabilitation.
Exclusion criteria:
- Patients who are under treatment for neuropathic pain, low back ache, intervertebral disc prolapse
- Patients with peripheral vascular disease, rheumatoid arthritis, history of psychiatric illness
- Patients with previous injuries/infections to the knee.
After obtaining Institutional Ethics Committee approval and written informed consent, 110 patients undergoing TKA were followed up at 2, 6, and 12 weeks postoperatively. At each visit, symptoms and signs were assessed using the Budapest criteria [6], including sensory, sudomotor, vasomotor, motor, and trophic changes through a structured questionnaire. Data were entered in Microsoft Excel and analysed using the Statistical Package for the Social Sciences version 21; quantitative variables were expressed as mean ± standard deviation and qualitative variables as frequencies and percentages. The chi-square test was applied, with a P < 0.05 considered statistically significant. Participant confidentiality was maintained throughout the study, and no financial burden was imposed on the participants.
Baseline characteristics:
Out of 110 patients, the mean age was 61.0 ± 7.4 years, with the majority being between 50 and 70 years of age (87 patients, 79.1%). Forty-seven patients (42.7%) were aged 50–60 years, 44 patients (40.0%) were aged 61–70 years, and 19 patients (17.3%) were aged 71–80 years. There was a marked female predominance, with 101 female patients (91.8%) and 9 male patients (8.2%). The mean duration of osteoarthritic symptoms was 6.8 ± 5.1 years, with most patients reporting symptoms for <10 years (93 patients, 84.6%). Fifty-two patients (47.3%) reported symptoms for <5 years, 41 patients (37.3%) for 5–10 years, 8 patients (7.3%) for 11–15 years, 7 patients (6.4%) for 16–20 years, and 2 patients (1.8%) for 21–25 years. Right-sided knee involvement was more common, observed in 71 patients (64.5%), compared with left-sided involvement in 39 patients (35.5%) (Table 1).
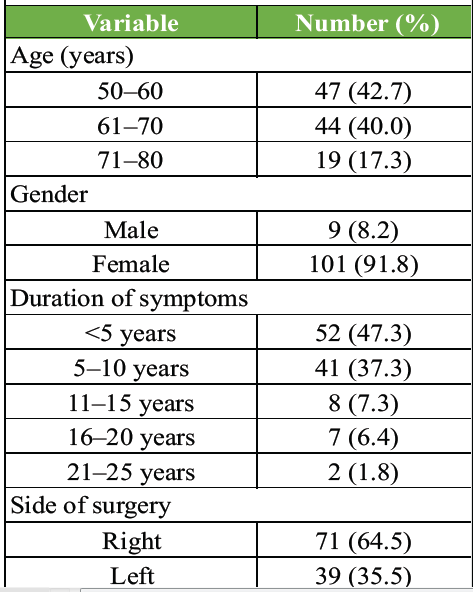
Table 1: Baseline demographic and clinical characteristics (n=110)
Incidence of CRPS:
At the first post-operative review (2 weeks), 21 patients (19.1%) fulfilled the Budapest criteria for CRPS. At the second review (6 weeks), CRPS was present in 10 patients (9.1%). By the third review (12 weeks), only 2 patients (1.8%) continued to demonstrate features of CRPS (Table 2 and Fig. 1).
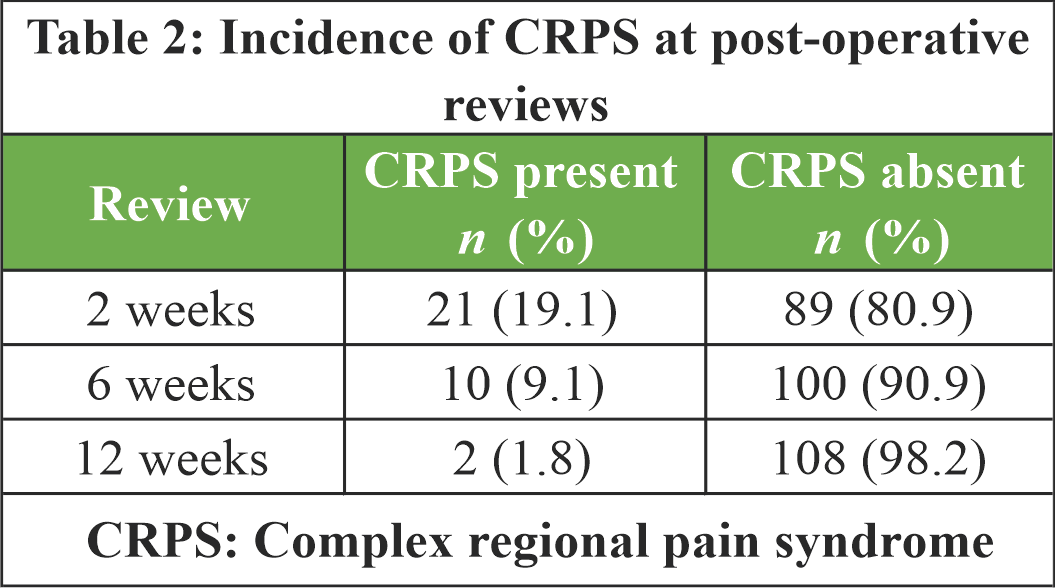
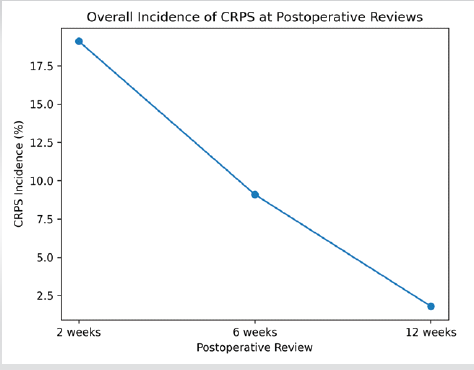
Figure 1: Overall incidence of complex regional pain syndrome at post-operative reviews.
Association between age and CRPS:
At the first post-operative review, CRPS incidence increased significantly with advancing age, with the highest proportion observed in the 71–80-year age group (57.9%) (χ2 = 27.33, P = 0.001). A similar statistically significant age-related trend persisted at the second post-operative review (χ2 = 16.33, P = 0.001). At the third review, CRPS was observed only in patients aged above 60 years; however, this association was not statistically significant (χ2 = 2.18, P = 0.335) (Table 3 and Fig. 2).
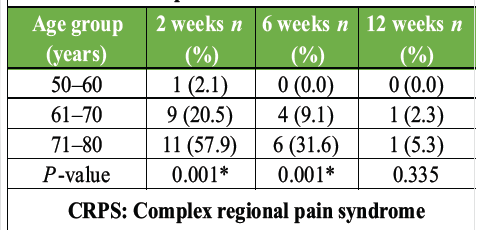
Table 3: Age-wise distribution of CRPS at post-operative reviews
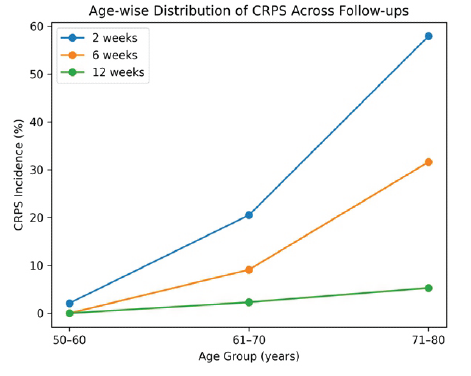
Figure 2: Age wise distribution of complex regional pain syndrome across follow-ups.
Association between gender and CRPS:
Females constituted the majority of CRPS cases at all post-operative reviews. At the first review, 19 of the 21 CRPS cases occurred in females. At the second review, 8 of the 10 cases were females, and at the third review, both cases were females. No statistically significant association was found between gender and CRPS at any post-operative review (P > 0.05) (Table 4 and Fig. 3).
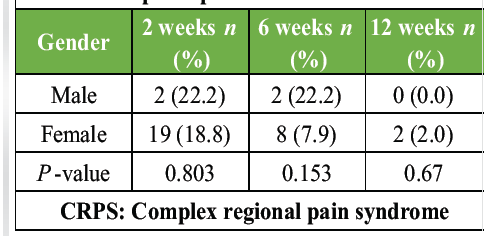
Table 4: Gender-wise distribution of CRPS at post-operative reviews
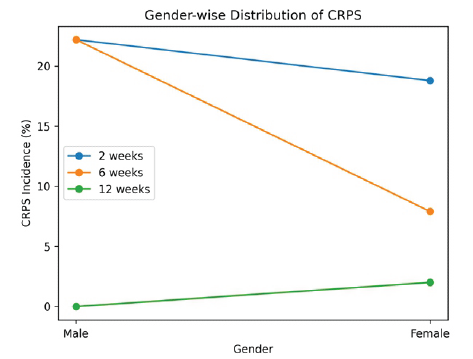
Figure 3: Gender-wise distribution of complex regional pain syndrome.
Association between duration of symptoms and CRPS:
A statistically significant association was observed between longer duration of osteoarthritic symptoms and CRPS at all post-operative reviews. At the first review, CRPS incidence increased progressively with symptom duration, reaching 100% in patients with symptoms lasting 21–25 years (χ2 = 29.08, P = 0.001). At the second review, no CRPS cases were observed in patients with symptoms of <5 years’ duration, whereas both patients with symptoms exceeding 20 years developed CRPS (χ2 = 48.09, P = 0.001). At the third review, CRPS was observed only in patients with a symptom duration of 16 years or more (χ2 = 33.98, P = 0.001) (Table 5 and Fig. 4).
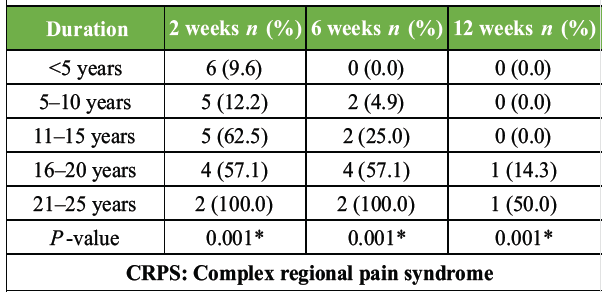
Table 5: Duration of osteoarthritic symptoms and CRPS
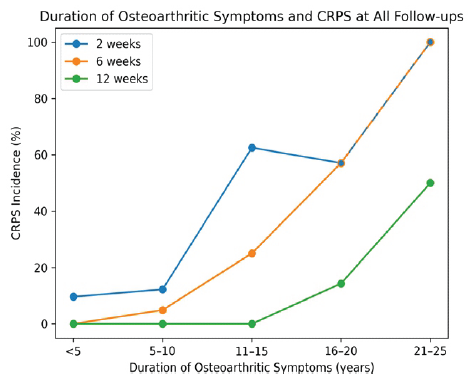
Figure 4: Duration of osteoarthritic symptoms and complex regional pain syndrome at all follow-ups.
The study showed that age had a significant association with CRPS at the 2-week and 6-week follow-up assessments. The duration of symptoms was significantly associated with CRPS at all review intervals. In contrast, gender did not demonstrate a significant association with the occurrence of CRPS.
CRPS most commonly develops following fractures or immobilisation and results from an exaggerated response to injury. It is characterised by trophic changes, sensory disturbances such as hyperaesthesia or allodynia, and sudomotor and vasomotor dysfunction. Although several international studies have evaluated CRPS following surgery, Indian literature on CRPS after TKA remains limited. According to the study on predictors of CRPS after knee arthroplasty [5], it has been concluded that at 6 weeks postoperatively, 62.7% had a diagnosis of CRPS, and 12.7% 6 months postoperatively. Nurdan and Osman [7] retrospectively analyzed 88 CRPS patients and assessed demographic and clinical characteristics, reporting a relatively balanced gender distribution. In contrast, our study population consisted predominantly of females (101 females, 9 males). Burns et al. [8] reported no significant association between age or gender and CRPS, while our study demonstrated a significant association with increasing age but no gender correlation, consistent with their findings. Several diagnostic criteria for CRPS have been proposed. The Orlando criteria, introduced by the IASP, were later refined into the Budapest criteria to reduce overdiagnosis. Kosy et al. [9] prospectively evaluated 100 primary TKA patients and reported CRPS diagnoses using Orlando criteria, but none using Budapest criteria. Similarly, in our study, the incidence of CRPS at the 3-month follow-up was low (1.8%, n = 2) when diagnosed using Budapest criteria. Early post-operative visits in our study showed higher CRPS-related symptoms, which decreased on subsequent follow-ups. Veldman et al. [10], in a prospective study of 829 patients, reported a high prevalence of pain, sensory disturbances, tremors, and incoordination. In comparison, our study noted temperature changes (66.7%), spasms (61.9%), swelling (38.1%), and hyperesthesia (23.8%) at the 2nd-week follow-up, with progressive reduction thereafter. Ott and Maihöfner [11] retrospectively compared CRPS patients with other pain disorders and reported that while the Orlando criteria had the highest sensitivity and the Bruehl criteria the highest specificity, the Budapest criteria offered the best balance. Accordingly, the Budapest criteria were used in our study. Kim et al. [12], in a population-based Korean study, reported an incidence of 29/100,000 person-years and found age and sex to be significant epidemiological factors, with an increasing proportion of CRPS Type I cases. The high early incidence of CRPS at 2 weeks (19.1%) followed by a sharp decline to 1.8% at 12 weeks indicates that post-TKA CRPS is primarily driven by an intense, acute perioperative inflammatory response and transient peripheral neurovascular sensitization. This transient early inflation, followed by rapid resolution, highlights how classic post-operative over-representation mimics true pathology if stringent timelines are ignored [9]. The statistically significant correlation with advancing age and prolonged pre-operative OA symptoms points toward chronic central sensitization. Patients with decades of OA endure unremitting nociceptive input that alters central sensory-motor processing, lowers pain thresholds, and correlates directly with severe post-operative pain amplification [13]. When combined with age-related systemic low-grade inflammation, the surgical trauma of a TKA triggers a maladaptive, hyper-reactive sympathetic and vasomotor cascade. To mitigate this risk, clinical strategies must pivot from treating surgery as a delayed “last resort” to executing timely interventions before permanent central pain pathways stabilize. For high-risk older cohorts with long-standing OA, perioperative management should mandate preemptive multimodal analgesia – incorporating neuroleptics like gabapentinoids – to suppress acute peripheral spikes and down-regulate hypersensitized dorsal column pathways [14]. Furthermore, given that swelling and vasomotor changes peak within the initial weeks, introducing early, non-provocative physiotherapy is critical to restore range of motion and disrupt the pain-vasospasm cycle. Ultimately, implementing structured screening using the Budapest Criteria during the crucial 2–6-week post-operative window ensures immediate, multidisciplinary intervention, successfully preventing early, transient neurovascular distress from solidifying into chronic morbidity. In our study, age and duration of OA showed a statistically significant association with CRPS development, whereas gender did not. Sandroni et al. [15] demonstrated correlations between clinical features and autonomic laboratory indices in CRPS; however, laboratory parameters were not utilized in our study, and diagnosis was based solely on clinical signs and symptoms.
Limitations of the study:
This hospital-based study has limited generalisability. Reliance on the Budapest criteria may introduce subjective bias. The small sample size (n = 110) limits statistical power, and the short follow-up period restricts long-term assessment.
This study determined that the proportion of patients developing CRPS declines progressively over time, making it an uncommon complication by 3 months postoperatively when diagnosed using the Budapest criteria. Assessment of associated factors revealed that advanced age and a longer duration of pre-operative OA symptoms are significant risk factors for its development, whereas gender has no significant association. Consequently, early post-operative screening and close monitoring are essential for these identified high-risk cohorts to optimize recovery.
CRPS can occur in the early post-operative period following primary TKA, particularly in elderly patients and those with a long duration of OA symptoms. Early recognition using the Budapest criteria and prompt multidisciplinary management can lead to symptom resolution and prevent long-term functional impairment. Vigilant follow-up during the first 3 months after surgery is therefore essential.
References
- 1. Elsevier.Total knee arthroplasty – an overview [Internet]. ScienceDirect Topics; Available from:https://www.sciencedirect.com/topics/medicine-and-dentistry/total-knee-arthroplasty. [Last accessed on 15 Mar 2026]. [Google Scholar] [PubMed]
- 2. Vaienti E, Scita G, Ceccarelli F, Pogliacomi F. Understanding the human knee and its relationship to total knee replacement. Acta Bio-Medica Atenei Parm 2017;88:6-16. [Google Scholar] [PubMed]
- 3. Fox AJS, Wanivenhaus F, Burge AJ, Warren RF, Rodeo SA. The human meniscus: A review of anatomy, function, injury, and advances in treatment. Clin Anat 2015;28:269-87. [Google Scholar] [PubMed]
- 4. Chang A, Breeland G, Black AC, Hubbard JB. Anatomy, bony pelvis and lower limb: Femur. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2024. [Google Scholar] [PubMed]
- 5. Bruehl S. Complex regional pain syndrome. BMJ 2015;351:h2730. [Google Scholar] [PubMed]
- 6. Harden RN, Bruehl S, Perez RS, Birklein F, Marinus J, Maihofner C, et al. Validation of proposed diagnostic criteria (the “budapest criteria”) for complex regional pain syndrome. Pain 2010;150:268-74. [Google Scholar] [PubMed]
- 7. Nurdan Y, Osman D. The demographic and clinical characteristics of the patients with complex regional pain syndrome: A tertiary clinic experience. Fiziksel Tıp ve Rehabil Bilimleri Derg 2020;23152-7. [Google Scholar] [PubMed]
- 8. Burns AW, Parker DA, Coolican MR, Rajaratnam K. Complex regional pain syndrome complicating total knee arthroplasty. J Orthop Surg 2006;14:280-3. [Google Scholar] [PubMed]
- 9. Kosy JD, Middleton SW, Bradley BM, Stroud RM, Phillips JR, Toms AD. Complex regional pain syndrome after total knee arthroplasty is rare and misdiagnosis potentially hazardous-prospective study of the new diagnostic criteria in 100 patients with no cases identified. J Knee Surg 2018;31:797-803. [Google Scholar] [PubMed]
- 10. Veldman PH, Reynen HM, Arntz IE, Goris RJ. Signs and symptoms of reflex sympathetic dystrophy: Prospective study of 829 patients. Lancet 1993;342:1012-6. [Google Scholar] [PubMed]
- 11. Ott S, Maihöfner C. Signs and symptoms in 1,043 patients with complex regional pain syndrome. J Pain 2018;19:599-611. [Google Scholar] [PubMed]
- 12. Kim H, Lee CH, Kim SH, Kim YD. Epidemiology of complex regional pain syndrome in Korea: An electronic population health data study. PloS One 2018;13:e0198147. [Google Scholar] [PubMed]
- 13. Kim MS, Kim JJ, Kang KH, Kim MJ, In Y. Diagnosis of central sensitization and its effects on postoperative outcomes following total knee arthroplasty: A systematic review and meta-analysis. Diagnostics (Basel) 2022;12:1248. [Google Scholar] [PubMed]
- 14. Hunter CW, Deer TR, Jones MR, Chang Chien GC, D’Souza RS, Davis T, et al. Consensus guidelines on interventional therapies for knee pain (STEP Guidelines) from the American society of pain and neuroscience. J Pain Res 2022;15:2683-745. [Google Scholar] [PubMed]
- 15. Sandroni P, Low PA, Ferrer T, Opfer-Gehrking TL, Willner CL, Wilson PR. Complex regional pain syndrome I (CRPS I): Prospective study and laboratory evaluation. Clin J Pain 1998;14:282-9. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Stepwise Surgical Correction of Fixed Flexion Deformity in Total Knee Arthroplasty: Functional Outcomes
July 1, 2026 Stepwise Surgical Correction of Fixed Flexion Deformity in Total Knee Arthroplasty: Functional Outcomes February 1, 2026 Conventional Total Knee Arthroplasty in Severe Anterolateral Femoral Bowing: Lateralized Femoral Entry Point to Approach Navigation Level Alignment – A Case Report
February 1, 2026 Conventional Total Knee Arthroplasty in Severe Anterolateral Femoral Bowing: Lateralized Femoral Entry Point to Approach Navigation Level Alignment – A Case Report June 1, 2025 Total Knee Arthroplasty following Genicular Artery Embolization: A Case Report
June 1, 2025 Total Knee Arthroplasty following Genicular Artery Embolization: A Case Report August 1, 2026 The Boba Tea Sign: A Novel Magnetic Resonance Imaging Finding in Synovial Chondromatosis of the Knee – A Case Report
August 1, 2026 The Boba Tea Sign: A Novel Magnetic Resonance Imaging Finding in Synovial Chondromatosis of the Knee – A Case Report