
Early diagnosis and prompt surgical treatment to restore the anatomical surface are crucial for achieving favourable outcomes and reducing the risk of future complications and disability.
Duwarkesh B Kavlekar, Department of Orthopaedic Surgery, Goa Medical College, Bambolim, Goa, India. E-mail: duwa.kavlekar@gmail.com
Abstract
Introduction: The navicular bone is a tarsal bone of the foot. It is an important bone that supports the medial arch of the foot. Navicular bone fractures are a rare injury. Fractures may occur as a result of stress or trauma. In both scenarios, it may be considered high risk due to poor blood supply to the bone. It is more common in athletes while kicking, sprinting, twisting, or falling. We report a case of a comminuted navicular fracture in an individual fixed with the Joshi external stabilisation system (JESS).
Case Report: A 40-year-old male presented with injury to the right foot. The patient met with an accident; he was brought to the casualty department. He was conscious, cooperative, and alert. No other bony injury was noted. There was no history of blunt abdominal trauma; however, blunt chest trauma was noted. No history of diabetes mellitus. The patient was newly detected as hypertensive and was treated with tablet amlodipine 5 mg bd and tablet telmisartan 40 mg at night.
Conclusion: Navicular bone fracture is a rare injury. It results from either stress fractures or trauma. Early diagnosis of suspicion and prompt treatment are key to success. JESS was the choice of treatment in this case. Other cases may need open reduction and internal fixation.
Keywords: Navicular ,comminuted, Joshi external stabilization system.
Navicular bone fractures tend to occur following stress or trauma. It is a rare injury. In both scenarios, it is considered high risk due to poor blood supply. Stress fractures of the navicular bone represent up to one-third of all stress fractures [1,2]. The majority of cases are seen in athletes while kicking, twisting, or sprinting. Traumatic navicular bone fractures account for a small proportion of cases. Being high risk for complications, it is often necessary to have open reduction and internal fixation in most cases of displaced fractures. However, in severely comminuted, shattered, crushed bone fractures, the external fixator becomes the choice. Treatment should aim at maintaining anatomical congruity of the medial column of the foot to prevent a midfoot catastrophe, which can leave the individual with permanent disability. The navicular bone is a biconcave (boat-shaped) tarsal bone. It articulates with the talus, three cuneiform bones, the calcaneus, and the cuboid. It is the “keystone” of the medial longitudinal arch [3]. It provides attachment to the posterior tibialis tendon.
A 40-year-old male presented with injury to the right foot. The patient met with an accident; he was brought to the casualty department. He was conscious, cooperative, and alert. No other bony injury was noted. There was no history of blunt abdominal trauma; however, blunt chest trauma was noted. There was no history of diabetes mellitus. The patient was newly diagnosed as hypertensive in our ward. On examination, there was severe swelling of the foot; however, dorsalis pedis pulsations were felt equally on both sides. The patient was able to move his toes. There were no signs of compartment syndrome. Small abrasions were present. Laboratory tests revealed a haemoglobin of 14.8%, packed cell volume of 43.6%, and platelet count of 2.96 lakhs. Liver function tests were abnormal with total serum bilirubin 2.0 mg/dL (N 0.3–1.2). Serum glutamic-oxaloacetic transaminase 69 and serum glutamic-pyruvic transaminase 49 were slightly raised. The albumin/globulin ratio was maintained. Serum calcium and vitamin D3 were normal. The hepatitis B surface antigen (HBsAg) test was positive, the hepatitis B surface antibody (anti-HBs) positive, and the immunoglobulin M anti-HBs negative, indicating a chronic hepatitis B virus (HBV) infection. Other viral hepatitis, such as hepatitis A virus and hepatitis C virus, was ruled out. Human immunodeficiency virus, as a routine investigation, was negative. The X-ray showed a comminuted, shattered fracture of the navicular bone (Fig. 1).
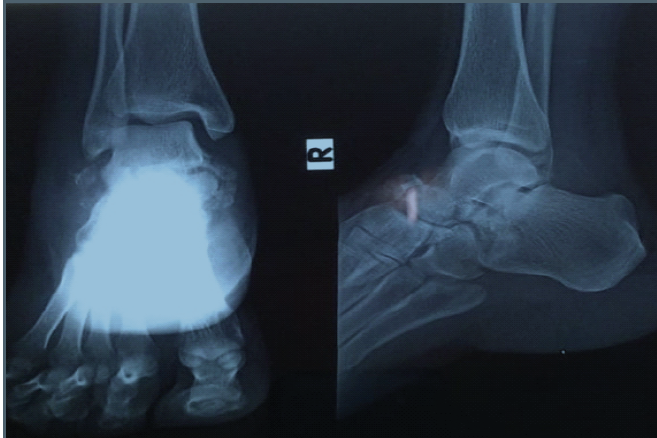
Figure 1: Pre-operative X-ray showing comminuted, shattered navicular bone fracture.
Computed tomography 3D Recon was done to see a 3D view and cut sections of the foot to plan the management (Fig. 2).
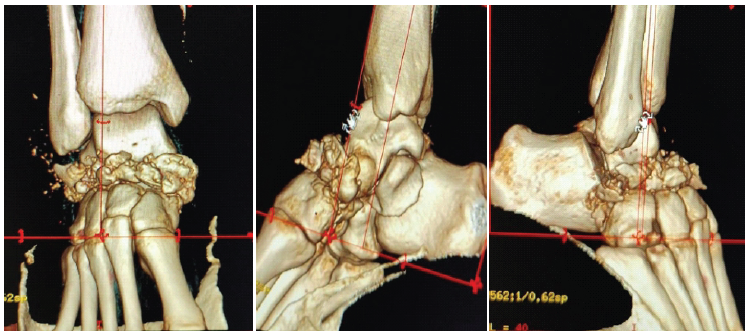
Figure 2: 3D volume rendering technique image.
Other investigations, such as an electrocardiogram, chest radiograph, and arterial blood gases, were normal. Treatment was started with a below-knee plaster as a first-aid measure, limb elevation on a Böhler-Brown splint, anti-oedema measures, analgesics, calcium, and vitamin D3. Simultaneously, the patient was also treated for hepatitis B. The patient was also started on antihypertensives. After going through all the reports, the decision was finally taken to operate on the patient with Joshi’s external stabilisation system (JESS). All the universal precautions were taken in the operating theatre, and the patient was operated on. The main aim of the operation was to distract the joint and manually milk all the fragments between the talus and cuneiform bones. Three pins were placed distally in the first metatarsal, 1 pin in the talus body, and 1 pin in the calcaneus, connected with a null rod and round clamps. Distraction was achieved with traction and countertraction, and the clamps were tightened. Reduction was achieved and confirmed with C-arm (Fig. 3).
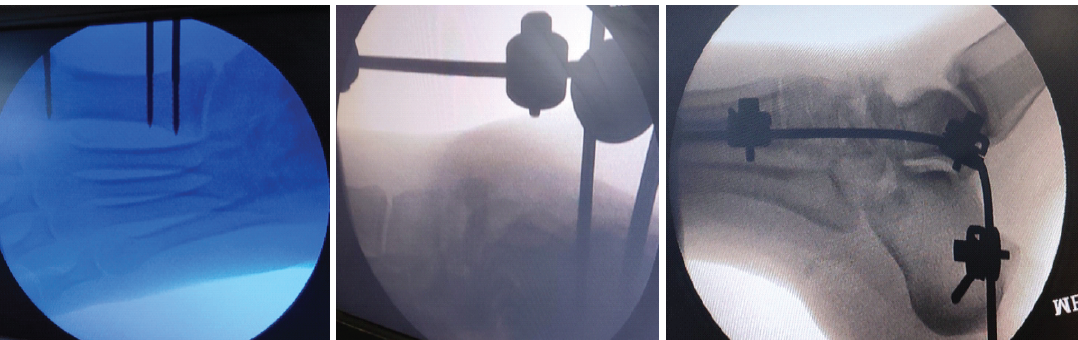
Figure 3: Intraoperative C-arm images.
Postoperatively (Fig. 4), ankle range of motion was started after 2 weeks as the patient tolerated pain and swelling had significantly reduced.

Figure 4: Post-operative X-ray.
The patient came for follow-up at 2 weeks and 1 month (Fig. 5).
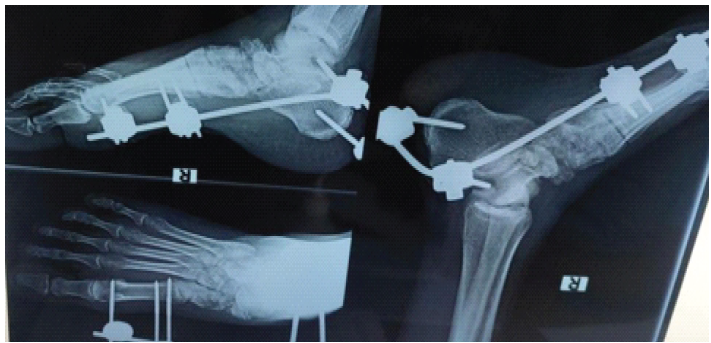
Figure 5: Follow-up at 1 month.
At 2½ months, JESS was removed. The patient was asked to weight-bear with partial weight-bearing, followed by full weight-bearing. By 3 months, an X-ray showing consolidation at the fracture site (Fig. 6), the patient was back to his work; however, he had difficulty squatting but still managed to do his work with minimal pain, which would subside with a painkiller, and swelling would be reduced with limb elevation.

Figure 6: X-ray after ex-fix removal at 3 months.
After that, the patient could not follow up, as he was a daily wage worker and stayed quite far away.
Navicular bone fractures are uncommon injuries presenting to an emergency department. A high degree of suspicion may be necessary to establish the diagnosis. Early diagnosis and prompt treatment are beneficial in obtaining a favourable outcome. Traumatic injuries may result in a variety of fracture patterns, including avulsion fractures, tuberosity fractures, and body fractures. The Sangeorzan classification [4] of navicular body fractures is based on the fracture plane and degree of comminution.
- Type 1: Transverse fracture of the dorsal fragment that involves <50% of the bone.
No associated deformity
- Type 2: Oblique fracture, usually from dorsal-lateral to plantar-medial.
May have forefoot adduction deformity.
- Type 3: Central or lateral comminution.
Abduction deformity. According to a newer classification [5] system reflecting talonavicular joint damage, they are classified as follows:
- Type I: Two-part fractures
- Type II: Multifragmentary fractures
- Type III: Fractures with talonavicular joint dislocation and/or concomitant talar fractures.
Rarely, accessory navicular bone fractures may be present or mistaken for a fracture. Navicular stress fractures clinically present as vague, aching pain in the dorsal midfoot that may radiate along the medial arch. The pain typically increases with activity such as running and jumping. With continued participation, the pain occurs sooner during activity and lasts longer into post-activity rest periods [6,7]. A microangiopathic study of cadaveric feet showed that while the navicular bone is supplied by both the anterior and posterior tibial arteries, the branches enter at the small “waist” of cortical bone and branch out to supply the medial and lateral thirds. This design leaves the central one-third, the area of greatest stress, as an area of relative avascularity [8,9]. JESS works on the principle of creating distraction and ligamentotaxis. In this patient, apart from a fracture of the navicular bone, there was talonavicular and naviculocuneiform displacement, which is very rare. To maintain medial column length, we aimed to distract the joint space and manually milk fragments in the joint space without opening the fracture site, thus having an added advantage in haematoma preservation and fracture healing. Apart from this, HBsAg positivity in the patient did influence our treatment plan: not to open the fracture site and to get reduction as much as possible, also decreasing the risk of exposure to health professionals. Simple fractures can be treated by either screws or plates [10]. It is imperative that patients are fully counselled about the nature of the injury and the risk of chronic pain, stiffness, non-union, and post-traumatic arthritis [11]. Delay in treatment may result in complications such as non-union, avascular necrosis, delayed union, talonavicular arthritis, and persistent pain on weight-bearing and activity.
Treatment for navicular fractures includes the following (Chart 1) [12,13]:
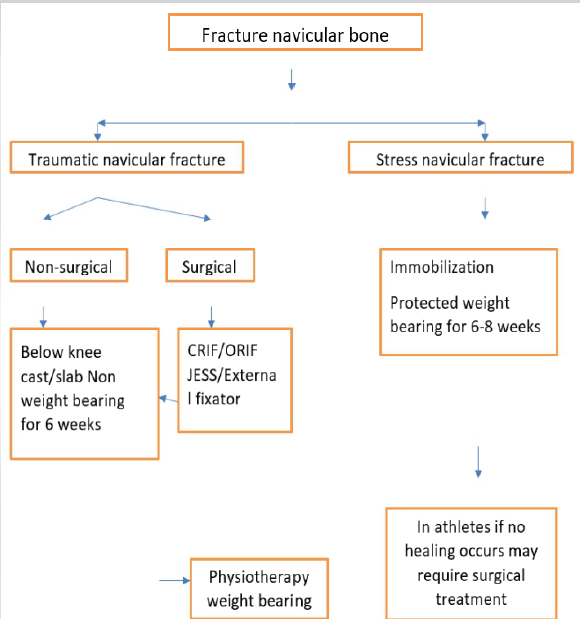
Chart 1: Treatment in navicular fractures includes.
In addition, chronic HBV infection in this patient can induce the production of inflammatory cytokines, such as tumour necrosis factor-alpha, interleukin-1, and interleukin-6, which increase receptor activator of nuclear factor kappa-B ligand to stimulate osteoclast genesis and bone resorption [14]. It increases the risk of osteoporosis. However, it has not been proven to cause osteoporotic fractures.
Navicular bone fracture is a rare injury. It results either from stress fractures or trauma. Early diagnosis of suspicion and prompt treatment are keys to success. JESS was the choice of treatment in this case. Other cases may need open reduction and internal fixation
Early diagnosis and prompt treatment are important factors for favourable outcomes. Simple fractures were treated by screws and/or tension band wiring, but in cases of comminution, the best choice of treatment remains the JESS with or without plates. The goal is to create optimal anatomical reduction, restore medial column length, and help in the early range of motion.
References
- 1. Ramadorai MU, Beuchel MW, Sangeorzan BJ. Fractures and dislocations of the tarsal navicular. J Am Acad Orthop Surg 2016;24:379-89. [Google Scholar] [PubMed]
- 2. Khan KM, Brukner PD, Kearney C, Fuller PJ, Bradshaw CJ, Kiss ZS. Tarsal navicular stress fracture in athletes. Sports Med 1994;17:65-76. [Google Scholar] [PubMed]
- 3. Eichenholtz SN, Levine DB. Fractures of the tarsal navicular bone. Clin Orthop Relat Res 1964;34:142-57. [Google Scholar] [PubMed]
- 4. Sangeorzan BJ, Benirschke SK, Mosca V, Mayo KA, Hansen ST Jr. Displaced intra-articular fractures of the tarsal navicular. J Bone Joint Surg Am 1989;71:1504-10. [Google Scholar] [PubMed]
- 5. Schmid T, Krause F, Gebel P, Weber M. Operative treatment of acute fractures of the tarsal navicular body: Midterm results with a new classification. Foot Ankle Int 2016;37:501-7. [Google Scholar] [PubMed]
- 6. Orava S, Karpakka J, Hulkko A, Takala T. Stress avulsion fracture of the tarsal navicular. An uncommon sports-related overuse injury. Am J Sports Med 1991;19:392-5. [Google Scholar] [PubMed]
- 7. Ting A, King W, Yocum L, Antonelli D, Moynes D, Kerlan R, et al. Stress fractures of the tarsal navicular in long-distance runners. Clin Sports Med 1988;7:89-101. [Google Scholar] [PubMed]
- 8. Van Langelaan EJ. A kinematical analysis of the tarsal joints. An x-ray photogrammetric study. Acta Orthop Scand Suppl 1983;204:1-269. [Google Scholar] [PubMed]
- 9. Torg JS, Pavlov H, Cooley LH, Bryant MH, Arnoczky SP, Bergfeld J, et al. Stress fractures of the tarsal navicular. A retrospective review of twenty-one cases. J Bone Joint Surg Am 1982;64:700-12. [Google Scholar] [PubMed]
- 10. Sanders R, Serrano R. Navicular body fractures – surgical treatment and radiographic results. J Orthop Trauma 2020;34 Suppl 1:S38-44. [Google Scholar] [PubMed]
- 11. Patel NG. Navicular fractures: Aetiology and management. Orthop Trauma 2018;32:423-7. [Google Scholar] [PubMed]
- 12. Shakked RJ, Walters EE, O’Malley MJ. Tarsal navicular stress fractures. Curr Rev Musculoskelet Med 2017;10:122-30. [Google Scholar] [PubMed]
- 13. Rosenbaum AJ, Uhl RL, DiPreta JA. Acute fractures of the tarsal navicular. Orthopaedics 2014;37:541-6. [Google Scholar] [PubMed]
- 14. Gilbert L, He X, Farmer P, Rubin J, Drissi H, Van Wijnen AJ, et al. Expression of the osteoblast differentiation factor RUNX2 (Cbfa1/AML3/Pebp2alphaA) is inhibited by tumour necrosis factor-alpha. J Biol Chem 2002;277:2695-701. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2026 Functional Outcome of Curettage and Chemical Cauterization with Bone Grafting and Fixation with Neo-Adjuvant Denosumab Therapy in a Case of Giant Cell Tumor of Navicular Bone of a Young Adult – A Case Report
March 1, 2026 Functional Outcome of Curettage and Chemical Cauterization with Bone Grafting and Fixation with Neo-Adjuvant Denosumab Therapy in a Case of Giant Cell Tumor of Navicular Bone of a Young Adult – A Case Report April 1, 2025 Minimally Invasive Posterior Plating for Comminuted Middle to Distal One-Third Humeral Shaft Fractures: A Case Report
April 1, 2025 Minimally Invasive Posterior Plating for Comminuted Middle to Distal One-Third Humeral Shaft Fractures: A Case Report October 1, 2024 The Joshi External Stabilization System: Simple yet Versatile
October 1, 2024 The Joshi External Stabilization System: Simple yet Versatile October 1, 2024 Outcome Analysis of Fixed angle Locking Plate in Comminuted Patella Fractures: A Single-center Prospective study from South India with Early Results
October 1, 2024 Outcome Analysis of Fixed angle Locking Plate in Comminuted Patella Fractures: A Single-center Prospective study from South India with Early Results