
The use of ultrasound guidance improves the accuracy of targeting the superficial branches of the sural nerve by avoiding injury to nearby vessels, thereby giving satisfactory long-term pain relief in patients with Haglund deformity.
Dr. Sidharth Verma, Department of Anaesthesia and Pain Medicine, DY Patil University, Navi Mumbai, Maharashtra, India. E-mail: sidharth2008@gmail.com
Abstract
Introduction: Haglund’s deformity is an abnormality of the bone and soft tissue of the foot, also known as retrocalcaneal exostosis, Mulholland deformity, and “pump bump”. The etiology is not well known. Probable causes include a tight Achilles tendon, a high arch of the foot, and hereditary. The clinical features consist of pain at the posterior aspect of the heel which is predominantly present when the patient begins to walk after a period of rest or inactivity.
Case Report: We report a case of a 60-year-old teacher with left heel pain for 3 years, unable to stand or walk for more than 15 min due to pain. We diagnosed him as a case of Haglund’s deformity and treated him with ultrasound-guided injections targeting the superficial branches of the sural nerve. This case report illustrates a rarely described modality for the management of heel pain due to Haglund’s deformity. Targeting superficial branches of the Sural nerve under ultrasound guidance can act as a superior treatment modality for the management of heel pain due to Haglund’s deformity.
Conclusion: Haglund's deformity is a cause of pain in the hindfoot that should be taken into account in the differential diagnosis of any patient presenting with heel pain. Ultrasonography has proved to be an important cost-effective tool in the diagnosis and management of various ankle pathologies like Haglund’s deformity, thereby reducing the sole dependence on surgical management. Targeting the superficial (cutaneous) branches of the sural nerve can give satisfactory long-term relief of heel pain in patients with Haglund deformity.
Keywords: Haglund’s deformity, heel pain, ultrasound-guided injection, sural nerve, rehabilitation.
Patrick Haglund first described Haglund’s deformity in 1927 as Retrocalcaneal exostosis, Mulholland deformity, and “Pump Bump.” This poorly understood clinical condition is an abnormality of the bone and soft tissues in the foot which is triggered by an enlargement of the bony section of the heel where the Achilles tendon is inserted (Fig. 1). The soft tissue near the back of the heel can become irritated when the large, bony lump rubs against rigid shoes. The etiology is not well understood and may include a tight Achilles tendon, a high arch of the foot, and hereditary (Table 1) [1].
Haglund’s deformity is a common cause of posterior heel pain, characterized clinically by prominent bursal bony projection. Dorsiflexion between the Achilles tendon and the calcaneal tuberosity results in bursal inflammation secondary to impingement or mechanical irritation [2]. Presenting complaints include pain at the posterior aspect of the heel which usually is triggered when the patient begins to walk after a period of rest or inactivity. Diagnosing this condition is usually difficult as the clinical picture may mimic other causes of heel pain, such as isolated retrocalcaneal bursitis and systemic arthropathies such as Reiter’s syndrome or rheumatoid arthritis (Table 2). With the increasing utilization of sonography as a diagnostic modality in the evaluation of foot and ankle pathology, the management of pain associated with Haglund deformity has become easier [3].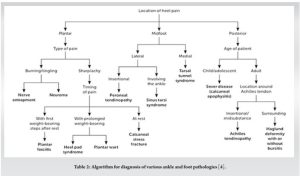
A 60-year-old male, a teacher by profession, came with chief complaints of left heel pain for 3 years. The pain was continuous, dull aching, non-radiating, and restricted to the left heel posterior aspect. It was aggravated by prolonged standing and walking for more than 15 min, and was relieved by taking rest. The patient did not have any hindrance to the range of motion at the ankle joint. The patient had a history of a road traffic accident in childhood wherein he had a fracture of his left tibia lower 1/3rd, for which open reduction and internal fixation were done. He has had diabetes for the past 6 years and hypertension for the past 4 years. His family history was normal. The patient had consulted multiple orthopedic surgeons before our consultation, who had advised him painkillers (celecoxib and diclofenac), steroids (prednisolone), calcium, and Vitamin-D supplements, but had no relief with all the above medications. He was also given the option of surgical excision of the bony exostosis, but the patient did not want to go ahead with the surgical option. General examination and systemic examination did not reveal anything significant. Local examination revealed a bony prominence at the posterior aspect of the left heel, associated with tenderness (Fig. 2). It was not associated with any redness or increased temperature. The stability of ankle and foot joints was conserved, and the Thompson test was negative. A lateral radiograph of the ankle revealed swelling of the soft tissue of the distal third of the Achilles tendon and a posterosuperior prominence of the calcaneus. Hence, we diagnosed him as a case of Haglund deformity. His visual analog score was recorded before the procedure and was noted to be 7/10. The patient was initiated on Gabapentin 100 mg twice a day, Baclofen 5 mg twice a day, Thiocolchicoside 4mg twice a day, and Type 2 collagen supplement once a day, for 1 week, and was also advised a proper physiotherapy regimen under the observation of a trained physiotherapist. The patient did not have any pain relief with the above medications. The patient was offered an ultrasound-guided left ankle injection under local anesthesia.

The patient was explained about the procedure and informed consent was taken. The patient was made to lie down in the right lateral position. Under strict aseptic precautions, parts were prepared and draped. Ultrasound guidance was used to locate the superficial branches of the sural nerve. The Achilles tendon and retrocalcaneal bursa were visualized and were found to be normal. The skin was infiltrated with 2% lignocaine at the site of needle entry (Fig. 3). The needle was inserted at the site of pain under ultrasound visualization near the superficial branches of the sural nerve, just next to the artery (Fig. 4).
The drug containing a mixture of 0.5% bupivacaine 20 mg + dexamethasone 4 mg + 250 mg amikacin, a total of 5 ml volume, was deposited under vision near the nerve, avoiding the artery as well as the Achilles tendon (Fig. 5).
The patient had 100% pain relief (visual analog scale [VAS] of 0/10) immediately after the procedure. Post-procedure, the patient was continued with the pharmacological agents (gabapentin 100 mg twice a day, baclofen 5 mg twice a day, thiocolchicoside 4 mg twice a day, Type 2 collagen supplement once a day) along with a physiotherapy regimen. The patient was also advised on shoe modification. The patient continued to have sustained 100% pain relief at 2 weeks and 1-month post-procedure follow-up (VAS 0/10). His medications were slowly tapered 2 weeks post-procedure and then stopped after 1 month. Physiotherapy exercises were however continued. At 2-month, 3-month, 6-month, 9-month, and 1-year post-procedure follow-up, the patient still had sustained 100% pain relief (VAS 0/10). A follow-up ultrasound scan of the Achilles tendon was done and was found to be normal (no images were saved as the scans were normal).
Haglund’s deformity also known as retrocalcaneal bursitis was described by Haglund in 1928 as an abnormal protuberance of the posterosuperior border of the calcaneus, usually seen in people wearing hard shoes [3]. It can occur in one or both feet and can usually present with the following symptoms:
- A prominent bump on the back of the heel
- Pain at the attachment site of the Achilles tendon (posterior aspect)
- Swelling in the back of the heel
- Redness may or may not be present.
A prominent plantar osseous projection alters the bone–soft-tissue interface of the hindfoot. Diagnosing Haglund’s syndrome solely from a clinical examination may be challenging as well as difficult to distinguish from other causes of hindfoot pain such as Reiter’s disease, rheumatoid arthritis, or isolated local conditions such as superficial Achilles Tendinosis secondary to poor shoe fit. Finding out the specific etiology is a key factor for initiating appropriate treatment [3].
Treatment options include
Surgery
Retrocalcaneal decompression and calcaneal osteotomy or osteotomy has been tried for many years, but most of these usually present with a recurrence of symptoms due to inadequate bone resection. Some may also present with post-surgical complications like scar formation with nerve entrapment, weakening or rupture of the Achilles tendon, and non-union of the calcaneal osteotomy [3].
Conservative treatment
Change of footwear, use of heel inserts, combined eccentric training, and conventional physical therapy including calf muscle and thigh muscle stretches have been tried but usually offer short-term relief. Ice massage on the Achilles tendon may help reduce inflammation [5].
Extracorporeal shock wave therapy (ESWT)
Recently, high and low-energy ESWT has been tried for the treatment of pain from Haglund’s deformity but has shown only moderate outcomes with fewer patients showing long-term relief [5].
Injection therapy
The current therapy of injections for treatment included sclerosing therapy, hyperosmolar dextrose injections, corticosteroid injections, and platelet-rich plasma (PRP) injections. However, high-quality evidence is lacking to support its use. Dextrose as well as PRP act by eliciting an exaggerated cellular response by inducing inflammation, and subsequent growth factor production, leading to increased fibroblast proliferation (either locally or systemic) and increased production of extracellular matrix materials [5]. These options are however more favorable for Achilles Tendinosis than for pain from Haglund’s Deformity. Corticosteroid injections have proven to be less efficacious in the treatment of this condition and are rarely used.
Ultrasound guided local anesthetic injection
Ultrasound guidance to inject the retrocalcaneal bursa is a simple, reliable method of ensuring accurate delivery of medication into the bursa under direct dynamic visualization, thereby avoiding any intratendinous or intra-articular injection. In the current case, the patient had complete relief of symptoms following the procedure. This non-surgical treatment regime, combined with modifications in daily shoe wear and physical therapy, is an appropriate goal-directed treatment modality for pain relief of Haglund’s Deformity [3,9,10]. The sural nerve is a cutaneous nerve, providing sensory innervation to the posterolateral aspect of the distal third of the leg and the lateral aspect of the foot, heel, and ankle. It is formed by terminal branches of the tibial nerve (medial sural cutaneous nerve) and common peroneal nerve (lateral sural cutaneous nerve), that join together in the superficial aspect of the distal third of the leg (Table 3).
 It is a purely sensory nerve and does not innervate any muscle group despite traveling between the two heads of the gastrocnemius muscle. These superficial cutaneous branches of the sural nerve can be located under ultrasound guidance and targeted for the management of heel pain [6,7,8,11,12,13]. Haglund’s deformity is a cause of pain in the hindfoot that should be taken into account in the differential diagnosis of any patient presenting with heel pain. It should be suspected in the light of the clinical characteristic finding, and be confirmed by radiological studies to ensure a correct diagnosis. Conservative treatment involving medical and physical therapy should be the first line of management. Ultrasonography has proved to be an important cost-effective tool in the diagnosis and management of various ankle pathologies like Haglund’s deformity, thereby reducing the sole dependence on surgical management. Targeting the superficial (cutaneous) branches of the sural nerve can give satisfactory long-term relief of heel pain in patients with Haglund deformity. Proper foot care as well as post-procedure physical therapy is also equally important in the adequate management of this condition, thereby ensuring that the patient gets long-term pain relief.
It is a purely sensory nerve and does not innervate any muscle group despite traveling between the two heads of the gastrocnemius muscle. These superficial cutaneous branches of the sural nerve can be located under ultrasound guidance and targeted for the management of heel pain [6,7,8,11,12,13]. Haglund’s deformity is a cause of pain in the hindfoot that should be taken into account in the differential diagnosis of any patient presenting with heel pain. It should be suspected in the light of the clinical characteristic finding, and be confirmed by radiological studies to ensure a correct diagnosis. Conservative treatment involving medical and physical therapy should be the first line of management. Ultrasonography has proved to be an important cost-effective tool in the diagnosis and management of various ankle pathologies like Haglund’s deformity, thereby reducing the sole dependence on surgical management. Targeting the superficial (cutaneous) branches of the sural nerve can give satisfactory long-term relief of heel pain in patients with Haglund deformity. Proper foot care as well as post-procedure physical therapy is also equally important in the adequate management of this condition, thereby ensuring that the patient gets long-term pain relief.
Haglund’s deformity is a cause of pain in the hindfoot that should be taken into account in the differential diagnosis of any patient presenting with heel pain. It should be suspected in the light of the clinical characteristic finding, and be confirmed by radiological studies to ensure a correct diagnosis. Conservative treatment involving medical and physical therapy should be the first line of management. Ultrasonography has proved to be an important cost-effective tool in the diagnosis and management of various ankle pathologies like Haglund’s deformity, thereby reducing the sole dependence on surgical management. Targeting the superficial (cutaneous) branches of the sural nerve can give satisfactory long-term relief of heel pain in patients with Haglund deformity. Proper foot care as well as post-procedure physical therapy is also equally important in the adequate management of this condition, thereby ensuring that the patient gets long-term pain relief.
Targeting the superficial branches of the sural nerve under ultrasound guidance can give satisfactory long-term relief of heel pain in patients with Haglund deformity.
References
- 1.Vaishya R, Agarwal AK, Azizi AT, Vijay V. Haglund’s syndrome: A commonly seen mysterious condition. Cureus 2016;8:e820. [Google Scholar | PubMed]
- 2.Dave M, Dave HM, Rathava R, Moradiya NP. Surgical treatment of insertional Achilles tendinosis and Haglunds deformity by using central tendon-splitting approach. J Foot Ankle Surg 2019;6:18-22. [Google Scholar | PubMed]
- 3.Sofka CM, Adler RS, Positano R, Pavlov H, Luchs JS. Haglund’s syndrome: Diagnosis and treatment using sonography. HSS J 2006;2:27-9. [Google Scholar | PubMed]
- 4.Tu P. Heel pain: Diagnosis and management. Am Fam Physician 2018;97:86-93. [Google Scholar | PubMed]
- 5.Zhi X, Liu X, Han J, Xiang Y, Wu H, Wei S, et al. Nonoperative treatment of insertional Achilles tendinopathy: A systematic review. J Orthop Surg Res 2021;16:233. [Google Scholar | PubMed]
- 6.Martín FJ, Valdazo MD, Peña G, Herrero DH, García FD. Haglund’s syndrome. Two case reports. Reumatol Clin 2017;13:37-8. [Google Scholar | PubMed]
- 7.Sammarco GJ, Taylor AL. Operative management of Haglund's deformity in the nonathlete: A retrospective study. Foot Ankle Int 1998;19:724-9. [Google Scholar | PubMed]
- 8.Miniato MA, Nedeff N. Anatomy, Bony Pelvis and Lower Limb, Sural Nerve. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2022. [Google Scholar | PubMed]
- 9.Coraci D, Giovannini S, Bernetti A, Cordenonssi JT, Erra C, Piccinini G, Padua L, et al. Nerve ultrasound to prevent and treat iatrogenic sural nerve injury. J Electromyogr Kinesiol 2019;44:173-4. [Google Scholar | PubMed]
- 10.D’Souza RS, Johnson RL. Sural nerve block. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2022. Available: https://www.ncbi.nlm.nih.gov/books/NBK519541 [Last accessed on 2022 May 29]. [Google Scholar | PubMed]
- 11.Rbia N, Nijhuis TH, Roukema GR, Selles RW, Van der Vlies CH, Hovius SE, et al. Ultrasound assessment of the sural nerve in patients with neuropathic pain after ankle surgery. Muscle Nerve 2018;57:407-13. [Google Scholar | PubMed]
- 12.Wagle S, Glazebrook K, Moynagh M, Smith J, Sellon J, Skinner J, et al. Role of ultrasound-guided perineural injection of the posterior antebrachial cutaneous nerve for diagnosis and potential treatment of chronic lateral elbow pain. Skeletal Radiol 2021;50:425-30. [Google Scholar | PubMed]
- 13.Mol FM, Jansen CH, Boelens OB, Stronks DL, Eerten PV, Huygen FJ, et al. Adding steroids to lidocaine in a therapeutic injection regimen for patients with abdominal pain due to anterior cutaneous nerve entrapment syndrome (ACNES): A single-blinded randomized clinical trial. Scand J Pain 2018;18:505-12. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Aneurysmal Bone Cyst of Calcaneum in a Young Adult: A Rare Case Report
July 1, 2026 Aneurysmal Bone Cyst of Calcaneum in a Young Adult: A Rare Case Report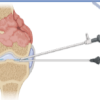 June 1, 2026 Creatine Supplementation in Pediatric Orthopedic Rehabilitation: A Translational Review and Proposed Clinical Trial Framework
June 1, 2026 Creatine Supplementation in Pediatric Orthopedic Rehabilitation: A Translational Review and Proposed Clinical Trial Framework June 1, 2026 Zoledronic Acid in the Management of Melorheostosis of Radius and Ulna – A Rare Case Report with Literature Review
June 1, 2026 Zoledronic Acid in the Management of Melorheostosis of Radius and Ulna – A Rare Case Report with Literature Review May 1, 2026 Surgical Treatment of Anchor-induced Heel Pain after Minimally Invasive Repair of Acute Achilles Tendon Rupture Using Percutaneous Achilles Repair System Achilles Midsubstance SpeedBridge™ Repair: A Case Report
May 1, 2026 Surgical Treatment of Anchor-induced Heel Pain after Minimally Invasive Repair of Acute Achilles Tendon Rupture Using Percutaneous Achilles Repair System Achilles Midsubstance SpeedBridge™ Repair: A Case Report