
Melorheostosis, a rare disease, can be effectively treated with conservative management, including injections of zoledronic acid, analgesics, and splints for limb support.
Dr. Sharan Mallya, Department of Orthopaedics, All India Institute of Medical Sciences, Guwahati - 781 101, Assam, India. E-mail: sharanmallya@gmail.com
Abstract
Introduction: Melorheostosis is an exceptionally rare mesodermal mixed sclerosing bone dysplasia that sometimes affects the surrounding soft tissue. There are no established guidelines for its management, as it is not a curable condition. Treatment primarily focuses on symptom relief and necessitates a coordinated multimodal approach involving orthopaedics, physical medicine and rehabilitation, and pain management to achieve optimal results. Bisphosphonates have shown efficacy in this condition, alleviating pain and reducing disease severity. The literature contains only nine reports concerning the use of zoledronate in the treatment of melorheostosis.
Case Report: We report a case involving a 24-year-old female diagnosed with melorheostosis affecting the radius and ulna, accompanied by subcutaneous hemangiomatosis, which was effectively managed with intravenous zoledronate and physiotherapy.
Conclusion: This case report emphasises the key characteristics of melorheostosis, the involvement of soft tissues in this condition, and the application of zoledronate in its treatment, while highlighting the need for and potential of future research in this area.
Keywords: Melorheostosis, zoledronic acid, bisphosphonates, bone dysplasia, rehabilitation.
Melorheostosis is an extremely rare non-hereditary mesodermal mixed sclerosing bone dysplasia that affects bones, occasionally involving adjacent soft tissues [1,2]. A review of the literature indicates that there are fewer than 500 formal publications on this mesenchymal disorder to date [2,3]. The occurrence of melorheostosis with involvement of surrounding soft-tissue structures is quite rare, with limited literature available [4]. The skin may exhibit thickening, a shiny appearance, or display characteristics like linear scleroderma or mottled livedo-reticularis. Associated symptoms may include erythema, excessive hair growth, subcutaneous oedema, fibrosis, fibromas or fibrolipomas, abnormal pigmentation, neurofibromatosis, patches resembling scleroderma, and vascular or lymphatic lesions. Infiltration of nearby joint structures, such as capsules, muscles, tendons, and ligaments, can lead to soft-tissue deformities, as well as muscle and joint contractures [5,6]. There are currently no established management guidelines for treating this condition, as it is not curable; however, literature has demonstrated successful outcomes with the use of bisphosphonates [7]. Our literature review concerning the management of melorheostosis with zoledronate has revealed only nine reports thus far. Evidence regarding the long-term effectiveness of zoledronate administration in this condition is limited. We present a case of melorheostosis affecting the radius and ulna of the left forearm in a female in her mid-twenties, along with a long-term follow-up on disease mitigation achieved through yearly administration of zoledronate.
A woman in her mid-twenties reported experiencing pain in her right forearm for the past 2.5 months. The pain began gradually, fluctuating in intensity, characterised as dull and aching, non-progressive, and ranging from mild-to-moderate in severity, impacting her quality of life, without any radiation. There were no clear aggravating factors identified, although the pain was alleviated by occasional non-steroidal anti-inflammatory drugs. She observed swelling in her right forearm accompanying the pain for the last 1.5 months. This swelling also developed gradually, was non-progressive and mild, but was diffusely distributed across her right forearm. There was no reported history of trauma. In addition, there was no indication of fever, weight loss, night pain, or night cries, nor any recent or past infections. No signs of infection were present in the patient. She did not indicate any contact history with tuberculosis, nor did she have any personal history of the disease. Her family medical history was unremarkable for any illnesses. The visual analogue scale (VAS) score and the disabilities of the arm, shoulder, and hand (DASH) score at the time of presentation were 6.5 and 25, respectively. On examination, mild tenderness was noted upon deep palpation of the right radius and ulna. Movements of the shoulder, elbow, wrist, and hand joints were found to be normal. A diffuse, ill-defined, pitting, circumferential boggy swelling of the right forearm was observed. There were no lesions or thickening of the skin, erythema, or localised increase in temperature in the affected forearm (Fig. 1).

Figure 1: The clinical examination of the patient’s right forearm reveals noticeable swelling. This swelling extends from 7 cm below the elbow joint line to the wrist joint. The maximum girth difference between the right and left forearms measures 15 mm.
X-ray imaging has confirmed the diagnosis of melorheostosis affecting both the radius and ulna (Fig. 2).
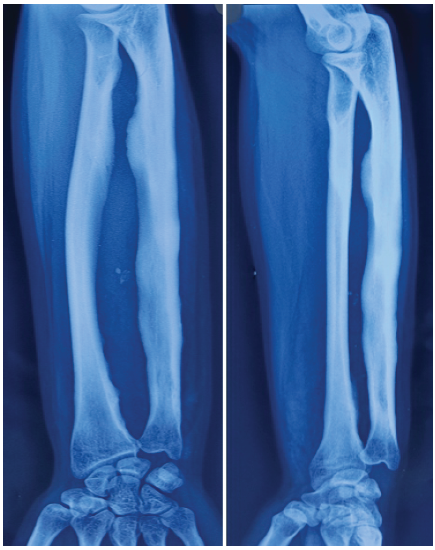
Figure 2: The X-ray displays both anteroposterior and oblique views of the radius and ulna in the right forearm. There is a notable presence of extensive, dense, irregular cortical and endosteal hyperostosis, which resembles the appearance of dripping candle wax, accompanied by a narrowing of the medullary canal in the affected radius and ulna.
In addition, magnetic resonance imaging (MRI) findings indicate significant subcutaneous hemangiomatosis in the right forearm, alongside the melorheostosis of the radius and ulna (Fig. 3).
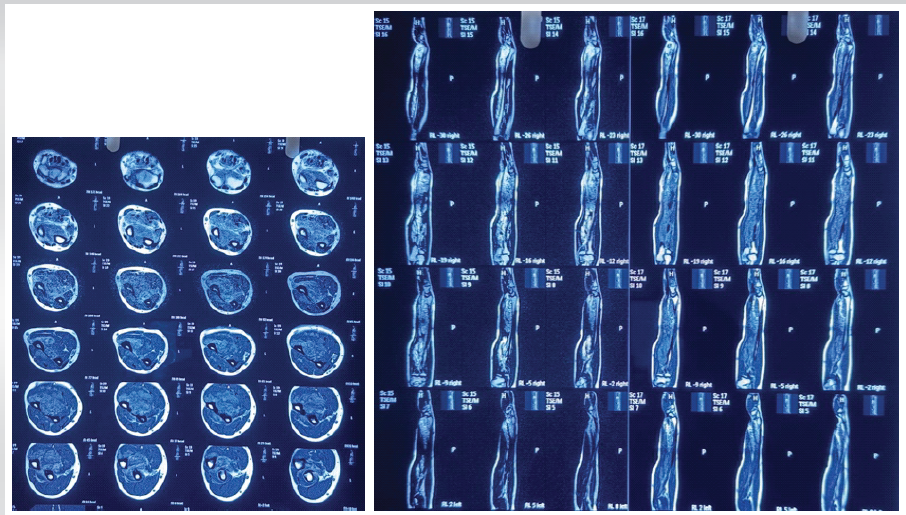
Figure 3: The magnetic resonance imaging of the right forearm done before Inj zoledronic acid management (serial axial images and sagittal images) – illustrates extensive homogeneous osteoid overgrowth within the cortex of the radius and ulna, which has encroached into the medullary cavity. There is also a localized decrease in signal intensity observed in the affected bones across all pulse sequences.
The patient was scheduled for bisphosphonate therapy utilising intravenous zoledronic acid, along with regular follow-up appointments. The management of hemangiomatosis was designated for serial observation under a “wait and watch” approach. Comprehensive evaluations, including complete blood counts, kidney function tests, alkaline phosphatase, serum calcium, phosphorus, vitamin D, parathyroid hormone, C-reactive protein, and erythrocyte sedimentation rate levels, were conducted, and all results were within normal limits. The patient’s dental examination yielded normal findings. The patient received intravenous zoledronate at a dosage of 5 mg over a duration of 60 min, following intravenous hydration with 0.9% normal saline. No adverse reactions were observed during or after the administration of the zoledronate infusion. The patient was instructed to engage in regular physiotherapy for the affected limb. At the 1-year follow-up, the patient reported considerable pain relief. The VAS score and DASH score were recorded at 2 and 17.5, respectively. The follow-up X-ray is illustrated in (Fig. 4).
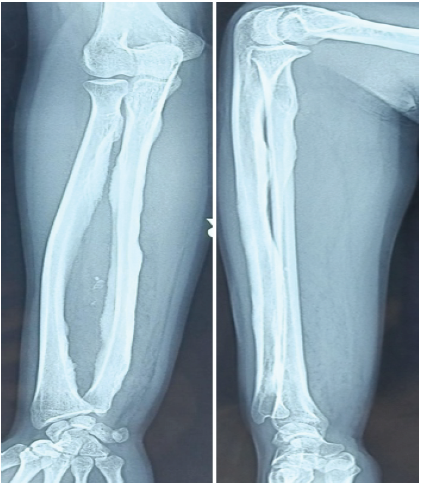
Figure 4: X-ray (anteroposterior and lateral views) after 1 year of treatment with zoledronic acid showing reduction of the cortical and endosteal hyperostosis, and appearance of lucency in the medullary canal of the affected radius and ulna.
In addition, there was a reduction in soft-tissue swelling, with the maximum difference in girth between the right and left forearms measuring 10 mm. A repeat dental check-up and routine investigations were performed, both of which returned normal results. The patient was given a second dose of intravenous zoledronate, again at 5 mg over 60 min, after intravenous hydration with 0.9% normal saline. No adverse events were noted during or after this infusion. The patient was advised to persist with physiotherapy for the affected limb. At the 2-year follow-up, both the VAS score and DASH score were recorded as zero. The maximum difference in girth between the right and left forearms further diminished to 7 mm (Fig. 5). The patient was entirely asymptomatic. The 2-year follow-up X-ray is depicted in Fig. 6 and MRI in Fig. 7.

Figure 5: Clinical picture of the right forearm of the patient showing the significant reduction of the swelling of the forearm, at 2 years follow-up.
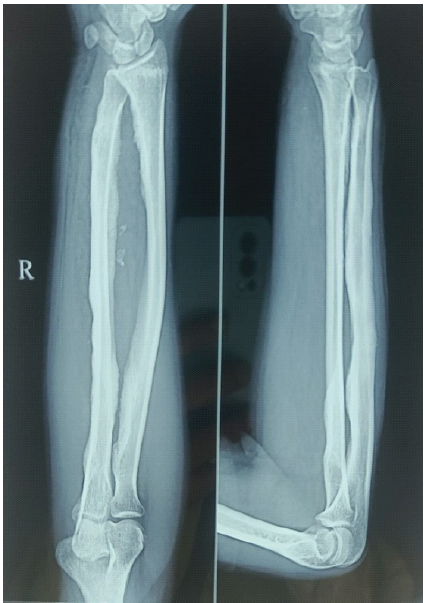
Figure 6: X-ray (anteroposterior and lateral views) of the radius and ulna of the right forearm. There is further improvement with reduction of the hyperostosis, and medullary canal lucency being prominent at 2 years follow-up.
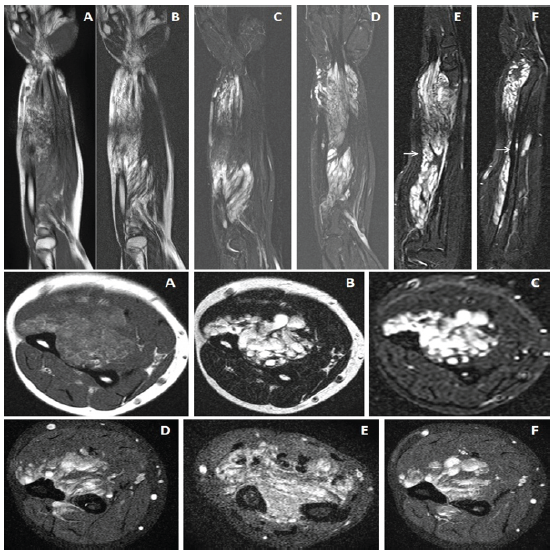
Figure 7: Magnetic resonance imaging of right forearm done after 2 years of initiation of Inj zoledronic acid (sagittal and axial serial images) showing widening of the medullary cavity with minimization of the hyperostosis. Vascular malformations were also noted in the sequences.
Melorheostosis is a rare condition that impacts fewer than one in a million individuals, showing no preference for gender, race, ethnicity, or environmental factors. The condition typically affects a single bone (monostotic), multiple bones (polyostotic), or a single limb (monomelic), with generalised bone involvement also possible. The most prevalent form is monomelic involvement. Associated vascular and lymphatic conditions with melorheostosis include: Hemangioma, vascular nevi, glomus tumors, varices, arteriovenous malformations, aneurysms, lymphedema, trophedema, and lymphangiectasia. In most instances, melorheostosis occurs sporadically; however, it can coexist with other hyperostotic bone disorders such as osteopoikilosis, osteopathia striata, Buschke-Ollendorf syndrome, or mixed sclerosing bone dysplasia. Most sporadic cases of melorheostosis are linked to mutations in the MAP2K1 gene, while LEMD3 germ-line mutations [8] do not occur in sporadic cases without the presence of osteopoikilosis or Buschke-Ollendorf syndrome. A small percentage of cases may be associated with KRAS mutations. Both MAP2K1 and KRAS mutations are related to sporadic extracranial arteriovenous malformations and are involved in the RAS/RAF/MAPK signalling pathways [9,10,11]. Furthermore, melorheostosis can resemble other conditions such as osteoma, myositis ossificans, and parosteal osteosarcoma. However, genetic or molecular testing was not performed in this case due to resource limitations. Incorporating molecular diagnostics could have strengthened the mechanistic understanding of the disease and may have implications for targeted therapies in the future. While changes typically manifest during childhood, individuals with this condition may remain asymptomatic until they reach early adulthood. The primary symptom often consists of bone or joint pain that intensifies with movement [12]. Additional symptoms may include: Joint stiffness, restricted range of motion, contracture, or limb deformity. Joint impingement syndromes and nerve entrapment syndromes (such as carpal tunnel syndrome and spinal nerve compression) may also arise. In some cases, soft-tissue abnormalities over the bone can serve as a key indicator of underlying osseous involvement. Although soft-tissue component involvement is uncommon, a thorough examination for soft-tissue issues is recommended in cases of melorheostosis. Early identification of soft-tissue involvement in melorheostosis can aid in preventing severe complications. Diagnosis is typically confirmed through X-rays, which reveal the characteristic “flowing or melting candle wax appearance” resulting from irregular, dense, eccentric hyperostosis affecting both the endosteal and periosteal surfaces of the bone cortices. Other patterns observable in Melorheostosis include “osteoma-like” hyperostosis that impacts only the inner surface of the long axis of the bone, “osteopathia striata-like” hyperostosis that produces dense, long, unilateral striations on the inner bony cortex, and a “myositis-ossificans-like” pattern of soft-tissue ossifications, with or without intraosseous hyperostosis [13]. Occasionally, there may be an overlap of one or more of the four radiological patterns [14]. Laboratory tests measuring calcium, phosphorus, alkaline phosphatase, vitamin D, parathyroid hormone, kidney function, and bone formation/resorption markers typically remain unaffected and within normal ranges in melorheostosis. In the present case, although routine biochemical parameters were within normal limits, specific bone turnover markers (such as serum CTX or P1NP) and advanced quantitative imaging modalities were not serially assessed. The inclusion of such objective biomarkers would enhance the evaluation of treatment response in future studies. Nonetheless, instances of rheumatoid arthritis [15] and hypophosphatemic rickets [16] have been reported in conjunction with melorheostosis. Patients with melorheostosis can derive the greatest benefit from a multimodal management approach that is coordinated among orthopaedics, physical medicine and rehabilitation, and pain management. The primary approach to treatment focuses on non-surgical methods for pain management and physiotherapy. When necessary, surgical procedures referenced in the literature may include: Tendon release or lengthening, release of contractures or fibrous tissue, corrective osteotomies, capsulotomy, fasciotomy, excision of ossified soft-tissue lesions, nerve blocks, sympathectomy, and, in severe cases, even amputation [17,18]. Surgical intervention should be considered only when conservative therapy fails, when pain is intractable, and when the pain’s location corresponds with the area affected by the soft-tissue component of melorheostosis [16]. Trametinib is an oral inhibitor that targets the kinase activity of MEK1 and MEK2, demonstrating potential as a treatment for vascular anomalies associated with the RAS/RAF/MEK kinase pathway in melorheostosis. Research on the application of trametinib for addressing vascular abnormalities linked to melorheostosis is quite limited. Interventional radiology presents a valuable approach for managing complex vascular malformations that do not respond to pharmacological treatments. The treatment options available for these extensive vascular malformations have been restricted; techniques such as sclerotherapy, embolisation, surgery, and laser ablation, whether utilised individually or in combination, frequently fail to achieve complete resolution. Bisphosphonates serve to inhibit osteoclast-mediated bone resorption, reduce bone vascularity, and alleviate pain. Zoledronate acts as a potent angiogenesis inhibitor in vitro [19,20]. The bone pain experienced in melorheostosis may result from increased osteoclastic bone resorption, the activation of pain receptors, elevated intraosseous pressure, and heightened vascularity. Therefore, zoledronate can contribute to reducing inflammation and pain receptor activation, decreasing bone resorption, and enhancing vascularity in melorheostosis [21] through various pathways. It is crucial to emphasise that maintaining good dental hygiene and normal serum vitamin D levels is vital before commencing bisphosphonate therapy due to the risk of jaw osteonecrosis [19]. In addition, conditions such as hypocalcaemia and renal impairment or insufficiency necessitate caution when administering zoledronate. We conducted a literature review regarding the management of melorheostosis with intravenous zoledronate and identified only nine reports to date (Table 1).
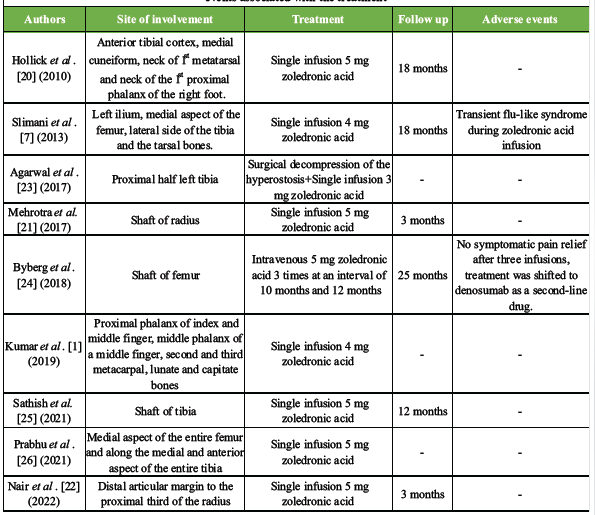
Table 1: Overview of the studies documented in the literature concerning the use of intravenous zoledronate for treating melorheostosis. This table emphasizes the site of involvement, treatment protocol, follow-up, and any adverse events associated with the treatment
Among these, Mehrotra et al. [22] and Nair et al. [23] have documented the use of zoledronate for melorheostosis affecting the radius. However, a longer follow-up is required to confirm the durability of clinical and radiological improvement in this condition. As a single case report, the study lacks a control group or comparative group, which limits the ability to definitively attribute the observed clinical and radiological improvement solely to zoledronic acid therapy. The contribution of the natural disease course and concurrent physiotherapy cannot be excluded. Comparative studies evaluating different bisphosphonates, targeted therapies such as trametinib, and surgical interventions are needed to establish optimal management strategies. We present the first case of melorheostosis involving both the radius and ulna, accompanied by soft-tissue involvement in the form of subcutaneous hemangiomatosis, which was successfully managed non-operatively through a “wait and watch” strategy utilising intravenous zoledronate and physiotherapy.
Limitations:
This report describes a single case of melorheostosis, which inherently limits the generalisability of the findings. The clinical response to zoledronic acid may vary among patients due to heterogeneity in disease distribution, activity, and associated soft-tissue involvement. Larger case series or controlled studies are required to validate the reproducibility of these outcomes. Although the patient demonstrated sustained clinical and radiological improvement over a 2-year follow-up period, melorheostosis is a chronic condition with an unpredictable course. Longer-term follow-up is necessary to determine the durability of symptom relief and to monitor for potential recurrence or progression.
Melorheostosis is a rare condition that presents significant treatment challenges and necessitates a coordinated multimodal management approach involving orthopedics, physical medicine and rehabilitation, and pain medicine to achieve optimal outcomes. The involvement of surrounding soft-tissues complicates the treatment of this disorder. While zoledronic acid appears promising in alleviating symptoms and improving radiological features, the evidence remains limited to case reports and small series. Future studies incorporating larger cohorts, molecular characterization, and objective biomarkers are essential to establish standardized treatment protocols.
Melorheostosis, a rare disease, can be managed effectively with conservative management, including injections of zoledronic acid, analgesics, and splints for limb support.
References
- 1. Kumar S, Jain VK, Prabhakar R. Melorheostosis of upper limb: A report of four rare cases. J Clin Orthop Trauma 2020;11:321-3. [Google Scholar] [PubMed]
- 2. Kotwal A, Clarke BL. Melorheostosis: A rare sclerosing bone dysplasia. Curr Osteoporos Rep 2017;15:335-42. [Google Scholar] [PubMed]
- 3. Wordsworth P, Chan M. Melorheostosis and osteopoikilosis: A review of clinical features and pathogenesis. Calcif Tissue Int 2019;104:530-43. [Google Scholar] [PubMed]
- 4. Chia K, Haron J, Nik Malek NF. Atypical presentation of melorheostosis with soft tissues involvement: A case report. Egypt J Radiol Nucl Med 2021;52:31. [Google Scholar] [PubMed]
- 5. Jain VK, Arya RK, Bharadwaj M, Kumar S. Melorheostosis: Clinicopathological features, diagnosis, and management. Orthopedics 2009;32:512. [Google Scholar] [PubMed]
- 6. Birtane M, Eryavuz M, Unalan H, Tüzün F. Melorheostosis: Report of a new case with linear scleroderma. Clin Rheumatol 1998;17:543-5. [Google Scholar] [PubMed]
- 7. Slimani S, Nezzar A, Makhloufi H. Successful treatment of pain in melorheostosis with zoledronate, with improvement on bone scintigraphy. BMJ Case Rep. 2013 Jun 21;2013:bcr2013009820. doi: 10.1136/bcr-2013-009820. PMID: 23813581; PMCID: PMC3702843. [Google Scholar] [PubMed] [CrossRef]
- 8. Charoenngam N, Nasr A, Shirvani A, Holick MF. Hereditary metabolic bone diseases: A review of pathogenesis, diagnosis and management. Genes (Basel) 2022;13:1880. [Google Scholar] [PubMed]
- 9. Queisser A, Seront E, Boon LM, Vikkula M. Genetic basis and therapies for vascular anomalies. Circ Res 2021;129:155-73. [Google Scholar] [PubMed]
- 10. Couto JA, Huang AY, Konczyk DJ, Goss JA, Fishman SJ, Mulliken JB, et al. Somatic MAP2K1 mutations are associated with extracranial arteriovenous malformation. Am J Hum Genet. 2017;100:546-54. [Google Scholar] [PubMed]
- 11. Al-Olabi L, Polubothu S, Dowsett K, Andrews KA, Stadnik P, Joseph AP, et al. Mosaic RAS/MAPK variants cause sporadic vascular malformations which respond to targeted therapy. J Clin Invest 2018;128:1496-508. [Google Scholar] [PubMed]
- 12. Freyschmidt J. Melorheostosis: A review of 23 cases. Eur Radiol 2001;11:474-9. [Google Scholar] [PubMed]
- 13. Smith GC, Pingree MJ, Freeman LA, Matsumoto JM, Howe BM, Kannas SN, et al. Melorheostosis: A retrospective clinical analysis of 24 patients at the mayo clinic. PM R 2017;9:283-8. [Google Scholar] [PubMed]
- 14. Todesco S, Bedendo A, Punzi L, D’Angelo A, Romani S. Melorheostosis and rheumatoid arthritis. Clin Exp Rheumatol 1983;1:349-52. [Google Scholar] [PubMed]
- 15. Lee SH, Sanderson J. Case report: Hypophosphataemic rickets and melorheostosis. Clin Radiol 1989;40:209-11. [Google Scholar] [PubMed]
- 16. Salaria AK, Singh G, Dogra E, Kumar N, Sodavarapu P, Neradi D. A highly unusual clinical presentation and imaging appearance of a rare diseases: Melorheostosis. J Orthop Case Rep 2020;10:72-5. [Google Scholar] [PubMed]
- 17. Hasegawa S, Kanda S, Imada H, Yamaguchi T, Akiyama T. Melorheostosis with recurrent soft-tissue components: A histologically confirmed case. Skeletal Radiol 2017;46:399-404. [Google Scholar] [PubMed]
- 18. Theriault RL. Zoledronic acid (Zometa) use in bone disease. Expert Rev Anticancer Ther 2003;3:157-66. [Google Scholar] [PubMed]
- 19. Wood J, Bonjean K, Ruetz S, Bellahcène A, Devy L, Foidart JM, et al. Novel antiangiogenic effects of the bisphosphonate compound zoledronic acid. J Pharmacol Exp Ther 2002;302:1055-61. [Google Scholar] [PubMed]
- 20. Hollick RJ, Black A, Reid D. Melorheostosis and its treatment with intravenous zoledronic acid. BMJ Case Rep. 2010;2010:bcr04.2009.1757. doi: 10.1136/bcr.04.2009.1757. Epub 2010 Apr 5. PMID: 22479293; PMCID: PMC3047172. [Google Scholar] [PubMed] [CrossRef]
- 21. Mehrotra R, Kumar P, Chaudhary D, Patel P, Singh A. Melorheostosis: Case report of rare disease. Int J Orthop Sci 2018;4:456-8. [Google Scholar] [PubMed]
- 22. Nair NR, Bagchi S, Mallya S. Melorheostosis of the radius bone: An incidental finding. Online J Health Allied Sci 2021;20:14. [Google Scholar] [PubMed]
- 23. Agarwal S, Khanna V, Varghese M, Suresh B. Localised melorheostosis. Int J Res Orthop 2017;3:635-8. [Google Scholar] [PubMed]
- 24. Byberg S, Abrahamsen B, Kassem M, Ralston S, Schwarz P. Clinical improvement in a patient with monostotic melorheostosis after treatment with denosumab: A case report. J Med Case Rep 2018;12:278. [Google Scholar] [PubMed]
- 25. Sathish M, Girinivasan C, Srinivasacholan C, Gowtham P. Bisphosphonate therapy in the management of symptomatic melorheostosis of tibia. J Orthop Case Rep 2021;11:103-6. [Google Scholar] [PubMed]
- 26. Prabhu B, Venkatesh Gupta SK, Anvith Shetty, Gurudarshan R (2021) Case report of a rare disease: Melorheostosis. J Med Case Rep Case Series 2(18): https://doi.org/10.38207/JMCRCS/2021/0218245 [Google Scholar] [PubMed] [CrossRef]




Related Articles in Journal of Orthopaedic Case Reports
 September 10, 2021 Bisphosphonate Therapy in the Management of Symptomatic Melorheostosis of Tibia
September 10, 2021 Bisphosphonate Therapy in the Management of Symptomatic Melorheostosis of Tibia August 1, 2026 Bisphosphonate-Related Pathological Femoral Fracture in a Child with ACTG2-Related Intestinal Failure and Metabolic Bone Disease: A Case Report
August 1, 2026 Bisphosphonate-Related Pathological Femoral Fracture in a Child with ACTG2-Related Intestinal Failure and Metabolic Bone Disease: A Case Report August 1, 2026 Post-operative C5 Palsy Following Posterior Cervical Decompression and Fusion: A Case Report
August 1, 2026 Post-operative C5 Palsy Following Posterior Cervical Decompression and Fusion: A Case Report July 1, 2026 A Rare Case of Giant Cell tumor of Bone in Distal Tibia
July 1, 2026 A Rare Case of Giant Cell tumor of Bone in Distal Tibia