
Fracture of the ZMR modular stem is a rare, catastrophic complication in revision hip arthroplasty, often caused by cantilever fatigue; monoblock stems may reduce this risk.
Dr. Osama Aldowekat, Department of Pediatric Orthopedics, Children’s Hospital of New Orleans, Louisiana state University, New Orleans, Louisiana. E-mail: Osamahabbadi1993@gmail.com
Abstract
Introduction: Zimmer modular revision (ZMR)® femoral stems are widely utilized in revision total hip arthroplasty (rTHA) due to their intraoperative customization that offers surgical flexibility in reconstructing complex hip joints. However, despite these advantages, the modular junction is prone to localized stress concentration, which may transfer cantilever loads distally. This mechanical environment possibly causes a fracture, often in the body-stem junction, where the cross-sectional area is reduced. Moreover, patient-based factors in addition to implant-related factors can both contribute to such rare but catastrophic failure. Factors such as bone quality, implant design, and surgical technique must be evaluated. These assessments will help in the formulation of a long-term management plan, along with a strategy to prevent this issue.
Case Report: In this report, we present a 70-year-old male patient with a past medical history of hypertension and a past surgical history of a left THA in 2011, a right THA in 2016, and a revision left THA using ZMR secondary to a periprosthetic fracture in 2021. In December 2023, he presented to the emergency department with a 2-day history of sudden atraumatic left groin pain. Imaging revealed a femoral stem fracture at the body-stem junction.
Conclusion: Although rare, cantilever fatigue of the ZMR stem is a serious complication. It is linked to both patient related factors (advanced age, high BMI, poor proximal bone stock), and implant factors (shorter length, smaller diameter, extended offset), with failure often occurring at the body–stem junction.
Keywords: Zimmer modular revision, total hip arthroplasty, cantilever load, implant failure, modular stem, non-modular revision.
Total hip arthroplasty (THA) has improved significantly over the time since it was first performed in Germany in 1891 by Doctor Thistocles Gluck, who used nickel screws to secure the ivory prosthesis to replace the tuberculosis-destroyed hip joints [1,2]. The advancements since then contribute to further improvements in implant designs, instrumentation, and surgical techniques based on the expertise of orthopedic surgeons. This improvement is noticed in both primary and revision cases of THA. Modular femoral implants are widely used in revision THA (rTHA) due to their precise intraoperative flexibility, enabling adjustments of limb length, offset, and anteversion according to individual anatomy, specifically, proximal femoral bone quality. The Zimmer modular revision (ZMR)® stem (Zimmer Biomet, Warsaw, IN, USA) is among the most commonly utilized systems designed for this purpose [3]. The ZMR system achieves modularity by having two components: the stem and the body. The stem has three different options: Taper (the most commonly utilized), porous, and spline. Each stem type provides certain lengths and diameters available, but in general, the length ranges from 115 to 260 mm, and the diameter ranges from 12 to 25.5. The body comes in three different types: Cone, which is used most often, as well as spout and calcar options [4]. Conversely, despite its intraoperative advantages, the concept of modularity introduces mechanical junctions that are susceptible to cantilever fatigue [5,6]. Cantilever fatigue refers to a mechanical failure that occurs when repeated bending stresses are applied to a component, such as the femoral stem or modular junction, due to its cantilevered position (fixed at one end and free at the other). This is applied in ZMR if it is distally fixed in a context of proximal bone deficiency [7]. Although ZMR stem failure is rare – reported around 4.6% in a survivorship study with follow-up periods of 15 years [8], Cantilever fatigue usually happens in the context of proximal femoral bone deficiency, where the load is transferred distally and concentrated at the modular junction. Hence, understanding the relationship between modular implants flexibility and their mechanical limitations is essential to optimize pre-operative planning and intraoperative interventions for better long-term implant survival. In this article, we present a case report of a ZMR femoral stem fracture and provide a literature review for similar cases. We also discuss patient-related and implant-related risk factors contributing to this complication and considerations for prevention.
We present the case of a 70-year-old male patient with a known history of hypertension. He was a retired office worker at a governmental institute and an independent ambulator with no significant functional limitations before presentation. His orthopedic history is notable for bilateral cementless total hip arthroplasties performed for primary hip osteoarthritis. The left THA (Zimmer) was performed in 2011, followed by the right THA (also Zimmer) in 2016. In 2021, the patient sustained a fall onto his left side, resulting in a periprosthetic proximal femoral fracture, classified as a Vancouver B2 (Fig. 1). He underwent surgical management involving stem exchange using a long revision stem (ZMR Stem), with revision of the acetabular shell (Fig. 2), the approach for femoral stem removal required a standard trochanteric osteotomy with application of cerclage wires. The post-operative course was uneventful, and he regained his baseline mobility and independence.
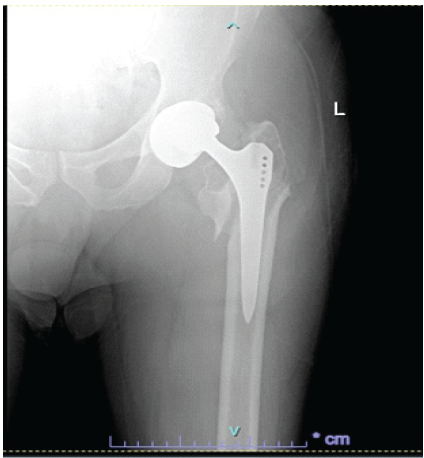
Figure 1: Vancouver B2 periprosthetic fracture of the left total hip arthroplasty.
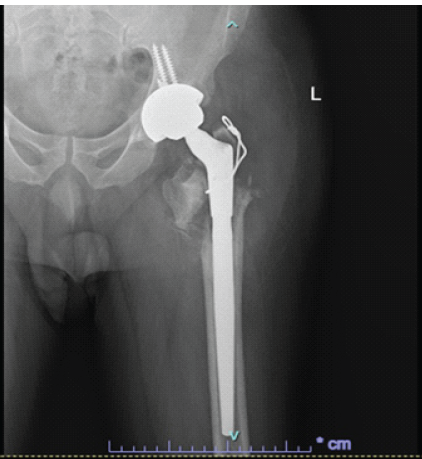
Figure 2: Revision of the left total hip arthroplasty using Zimmer modular revision stem.
On December 06, 2023, the patient presented to the emergency department with a complaint of acute-onset left hip pain of 2 days duration. Before this episode, he had been ambulating well and was asymptomatic. He denied any recent trauma, fever, chills, or rigors. The pain was described as sudden in onset and progressively worsening to the point where he became unable to bear weight on the affected limb. On physical examination, the patient was alert, oriented, and hemodynamically stable. His BMI is recorded as 27 kg/m2. There were no visible deformities, skin discoloration, bruising, or swelling over the hip or thigh. Local examination revealed tenderness over the proximal thigh and groin area. Neurovascular examination of the affected limb was intact. Given the patient’s history and clinical presentation, an urgent radiographic evaluation was performed. The X-ray images obtained in the emergency department are shown in Fig. 3a and b, showing a catastrophic failure of the system at the stem junction, noted along the cone taper stem junction. The patient was admitted for pain management and pre-operative planning.
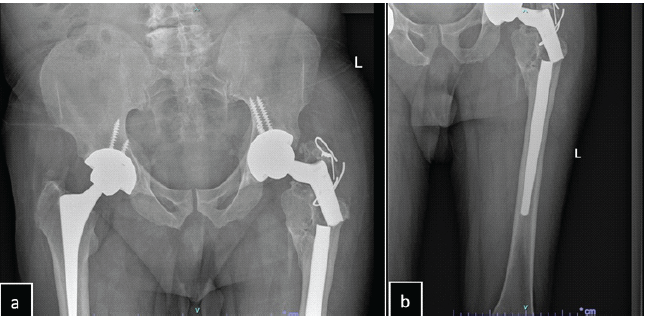
Figure 3: (a) Pelvic X-ray demonstrating failure of the left Zimmer modular revision system at the body-stem junction; (b) Left femur radiograph showing the same stem failure at the body-stem junction. Both images also reveal non-union of the greater trochanteric osteotomy from the prior revision surgery, with the distal stem appearing well-fixed.
He underwent revision hip arthroplasty for the femoral component with retention of the acetabular cup and reinforcement of the construct with multi-level cerclage wiring. Intraoperatively, a direct lateral approach was utilized, as it had been employed in the patient’s previous two arthroplasty procedures. The incision was extended distally to allow adequate exposure of the fractured femoral component. The cone module of the failed femoral component was found detached and was easily extracted. The polyethylene liner was removed, and revealed a stable, well-placed acetabular shell, which was left untouched. The distal stem was well fixed and difficult to extract. A longitudinal osteotomy along the stem was first performed to dilate the canal and facilitate stem removal; however, this approach was inadequate. Therefore, a diamond-tip drill bit was used to create a precise hole in the stem’s taper to enable the insertion of a punch, which allows retrograde hammering. This technique, which was described by Hafez et al., enables easier stem manipulation and prevents further femoral bone loss [9]. The failed stem is shown in Fig 4.

Figure 4: Clinical photograph showing the failed Zimmer modular revision stem.
Nasr et al. [10] also described a similar technique for a Revitan® stem removal. In their method, drilling was performed from beneath the stem through a midline incision over the knee with a medial parapatellar approach, and then a 16 mm drill was used to gain entry to the distal femoral metaphysis, and a custom-made instrument was inserted retrograde to punch the well-fixed femoral component towards the proximal femur. After thorough irrigation and bone preparation, a nonmodular Zimmer Wagner stem SL (size 16 mm diameter, 305 mm length) was implanted, ensuring a proper femoral anteversion. A reinforcement of the construct with multi-level cerclage wiring was applied, later followed by insertion of a ceramic head (size 52 mm, offset +0 mm) coupled with a new polyethylene liner (Fig. 5).
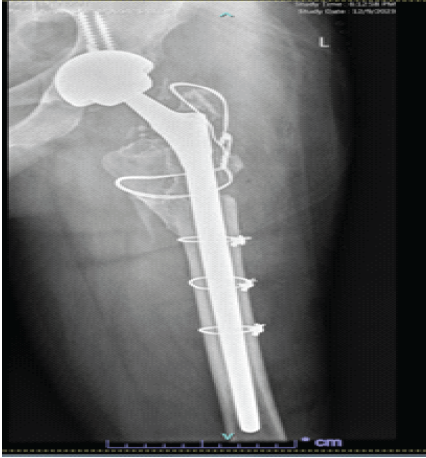
Figure 5: Post-operative radiograph demonstrating revision of the failed Zimmer modular revision stem using a monoblock, non-modular femoral component (Wagner SL Revision, length 305, diameter 16 mm).
Careful handling of the soft-tissue envelope was paramount in such revision surgery, particularly as it was the patient’s third major hip procedure, which in itself introduced another level of difficulty to this case. Special attention was given to the delicate abductor fibers, which were gently mobilized and reconstructed using transosseous sutures. This step was important to reduce the risk of post-operative dislocation. The total operative time was 2 h and 30 min, performed under spinal anesthesia. The patient received prophylactic intravenous second-generation cephalosporins (Cefuroxime) 1 h before incision. In addition, 1 gram of intravenous tranexamic acid was used to reduce the risk of major bleeding. Intraoperatively, 1 unit of packed red blood cells was transfused based on an estimated blood loss of 1000 mL and the calculated maximum allowable blood loss as determined by the anesthesiology team. The intraoperative course was uneventful, and the patient was sent to the recovery room in a hemodynamically stable condition. It is notable that intraoperative bacterial cultures were obtained, which later revealed no bacterial growth. The post-operative period included an adequate pain management regimen with a physiotherapy course including protected weight bearing for 6 weeks. The patient was discharged on post-operative day 4 with no recorded complications. An outpatient X-ray 3 months after the surgery is shown in Fig. 6a and 6b.
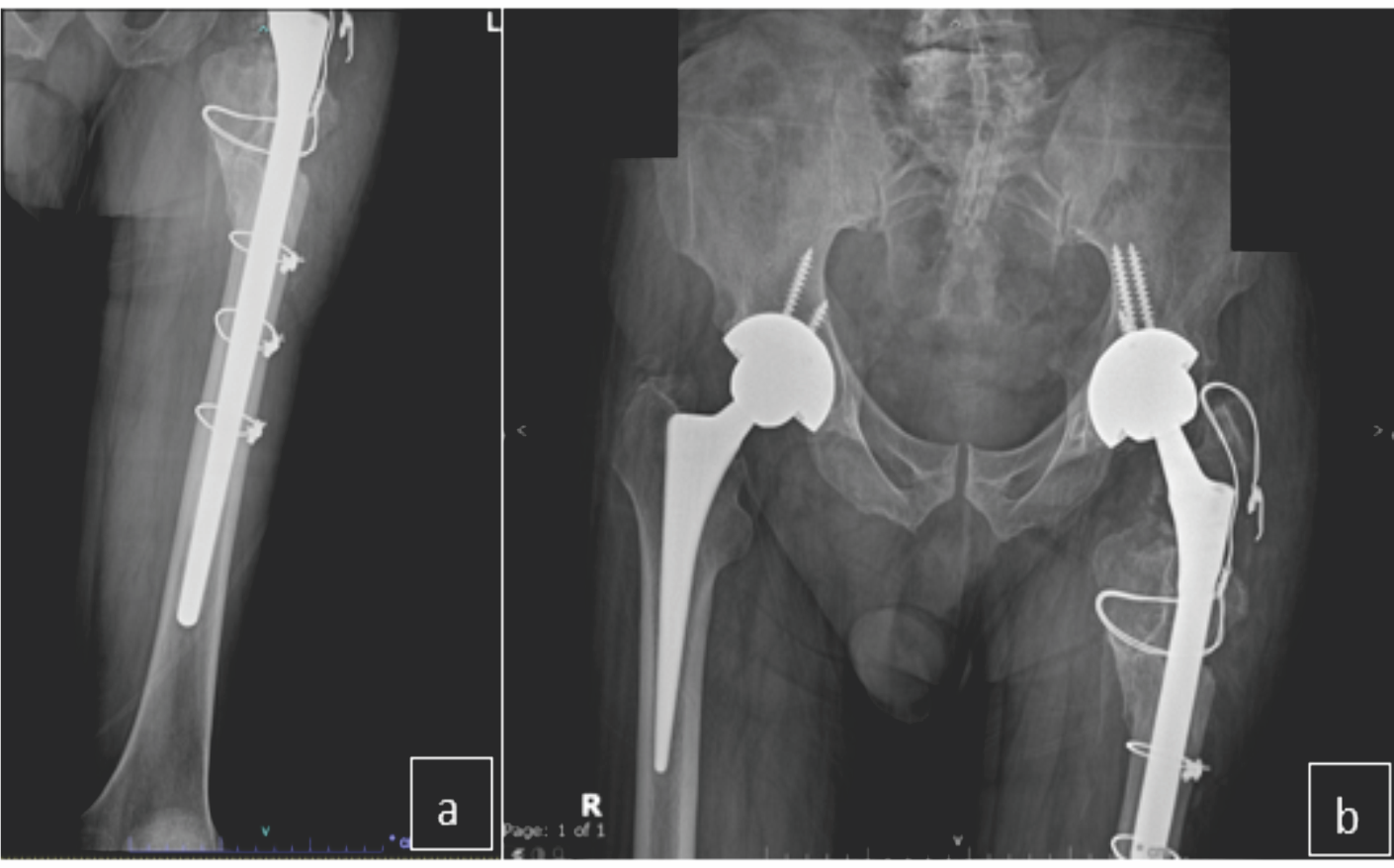
Figure 6: (a and b) Follow up left femur and pelvis AP radiographs, showing the revision using a Wagner SL stem remains well-fixed along with the cables and wires.
A literature search was conducted to identify reported cases of ZMR stem failure or fracture using the databases PubMed, ResearchGate, and Google Scholar. The search terms included “ZMR failure,” “ZMR stem failure,” “cantilever fatigue of the ZMR,” and “ZMR stem fracture.” Relevant cases were identified from four institutions: six from Lakstein et al. [11] (Mount Sinai Hospital, Toronto, Canada); two from Afshin et al. [12] (Islamic Azad University, Tehran, Iran); two from Efe et al. [13] (University of Marburg Hospital, Hessen, Germany); and one from Ortega et al. [14] (University of Santa Catarina, Florianópolis-SC, Brazil). These cases were reviewed and compared with our current case, with particular attention on patient-specific and implant-related variables. Corresponding authors of the Lakstein et al. (11) cases were contacted, and radiographic imaging was obtained for further analysis. Efforts to contact the authors of the Afshin et al. [12], Efe et al. [13], and Ortega et al. [14] cases were made, but additional information and imaging could not be obtained. In addition to the previously mentioned case reports, several larger series and survivorship data have documented ZMR stem fractures, although most did not provide complete clinical details. Hickie et al. [8] reported five stem fractures in a cohort of 108 revision hips using ZMR components over a 14.5-year follow-up, but individual radiographic or demographic data were not disclosed. Similarly, further evidence is available from the U.S. FDA MAUDE database, where at least two adverse events involving ZMR stem failure have been reported [15,16]. Due to the limited and often incomplete nature of these reports—typically lacking patient age, sex, BMI, radiographic evaluation, and implant details—these cases could not be included in comparative analysis. Nonetheless, their presence highlights that ZMR stem fractures, though rare, are recognized in both the literature and device surveillance systems.
Patient-related factors
In terms of patient-related factors, Table 1 shows the patients characteristics of the cases. Advanced age (over 65 years) was observed in all cases except two. High BMI also appeared to be a contributing risk factor, as all patients were either overweight (BMI: 25.5–29.9 kg/m2) or obese (BMI: >30.0 kg/m2). In all cases, the ZMR stem failure occurred without a history of significant trauma and no pain before the catastrophic event, with the exception of the Taheriazam et al. [12] and Ortega et al. [14] cases, for which some of this information was not available, as shown in Table 1. Infection workup was negative in all cases except Efe et al. [13], for which this information was missing. The failures were classified as late complications, occurring more than 2 years after the index surgery in all but four cases. Of the twelve cases, eight involved male patients and four involved female patients. To conclude, most patients were older than 65 and overweight or obese. Failures occurred late (>2 years post-operative), typically without major trauma. The majority were male (8 out of 12 cases). 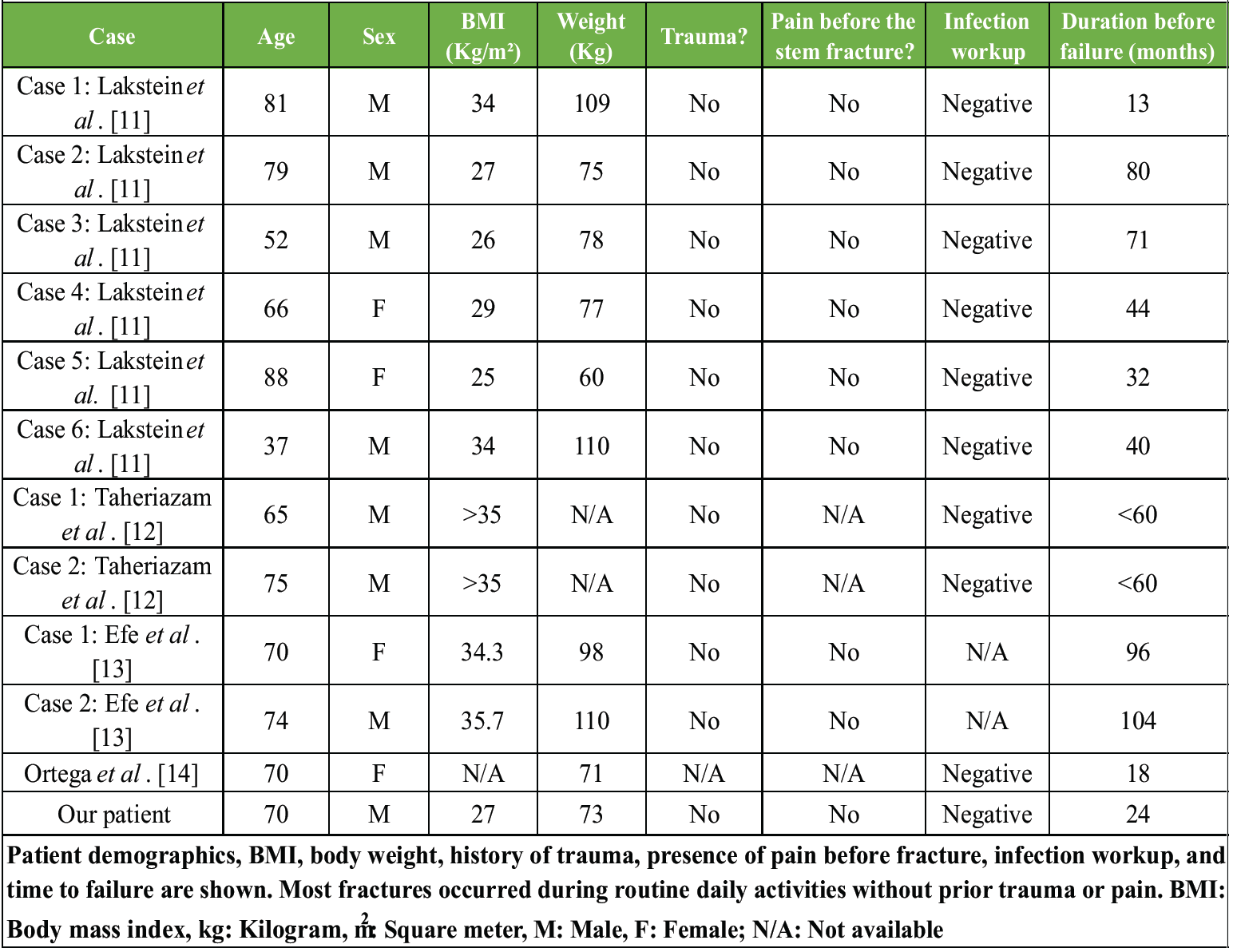
Table 1: Summary of reported ZMR stem fracture cases from the literature, including the present case
Implant-related factors
After careful review of all clinical photographs of the failed implants, a consistent finding was noted: the fracture occurred near the body-stem , precisely where the stem diameter tapers. The fracture lines were transverse, indicative of a high bending moment acting at this junction, ultimately resulting in this catastrophic failure [11-14] (Table 2).
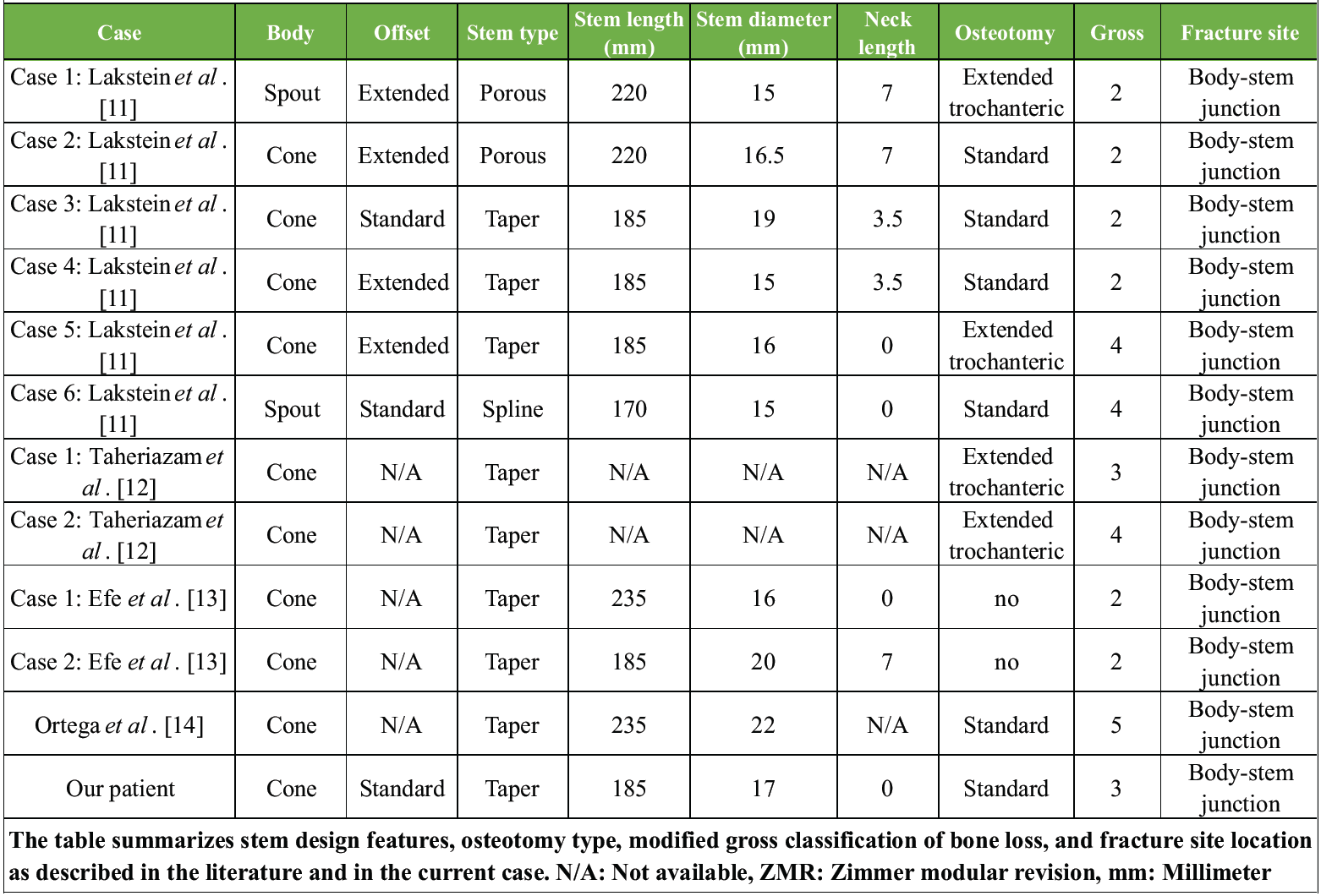
Table 2: Implant characteristics and fracture details of reported cases of ZMR stem failure
In this series, cone-type bodies were used in 10 out of 12 cases, with the remaining 2 being spout designs, and taper stems in 9 out of 12, with the remaining being 2 porous and 1 spline. However, given the predominance of cone-taper and spout-taper combinations in standard clinical practice, their frequency in this sample does not necessarily indicate an increased risk of ZMR failure; rather, they reflect the most commonly used configurations [8,17]. Extended offset stems were used in 4 out of 7 cases, with five cases not reporting this information, suggesting that extended offset may be a possible mechanical risk factor. The extended offset increases the horizontal distance between the hip joint reaction force and the stem axis, so we get a longer lever arm. This results in a greater bending moment at the body-stem (modular) junction, higher cyclic stresses during gait, and increased fatigue loading [18,19,20]. Consequently, this configuration may predispose the implant to crack initiation at its structurally weakest point – typically the junction where the cross-sectional diameter is reduced [21]. In terms of stem length, 6 out of 10 stems measured <200 mm, with an average length in all cases of 200.5 mm. This information was not reported in two cases. It is believed that shorter stems may be a risk factor for failure. Because shorter stems do not bypass the proximal bone deficiency adequately, the unsupported part of the stem acts as a long lever arm. This increases the bending moment at the modular junction and increases the likelihood of fatigue failure at the junction. In contrast, longer stems are more effective in distributing mechanical stress along their length more evenly and reduce cantilever forces – provided they achieve sufficient distal fixation and are supported by sufficient bone quality [11,22]. The stem diameter ranges from 15 to 22 mm for all included cases, with an average of 17.15 mm. All reported cases, except two, had stem diameters below 20 mm, with two other cases not reporting this information. Smaller stem diameters (<20 mm) may also explain the increased failure risk; this is because it is known that the bending strength of a cylindrical stem is proportional to the fourth power of its diameter (d4). Accordingly, even small reductions in diameter can lead to a substantial decrease in resistance to bending stress, increasing the likelihood of fatigue loading and fracture at high-stress junctions [20,23].
Bone-related factors
On review of the radiographs, all cases exhibited some degree of proximal femoral bone deficiency. This was mainly due to prior surgical interventions – most cases involved femoral osteotomies (10 out of 12) (Fig. 7 is showing various types of trochanteric osteotomies), with six reported as extended trochanteric osteotomies and four classified as standard trochanteric osteotomies. The type of osteotomy was determined based on radiographic evaluation, specifically the position of cerclage and/or cable wires, as not all the original articles specify the technique. It was not possible to distinguish whether a sliding or conventional osteotomy was performed in any of the cases. Four cases had persistent greater trochanteric non-unions. Such proximal bone stock deficiency resulted in inadequate support around the stem and contributed to a cantilever effect, intensifying the bending moment on the implant.
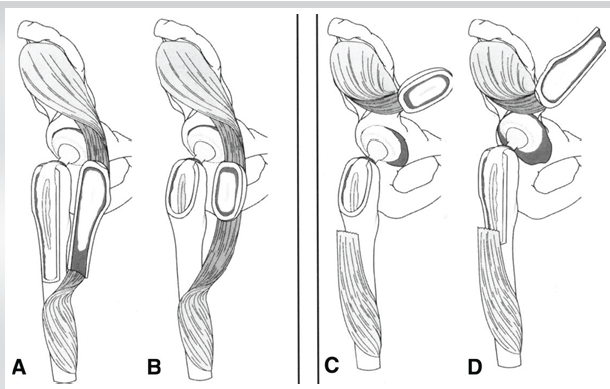
Figure 7: Sliding and conventional versions of the trochanteric osteotomy. (a) Extended slide; (b) simple slide; (c) conventional osteotomy; (d) extended conventional [25].
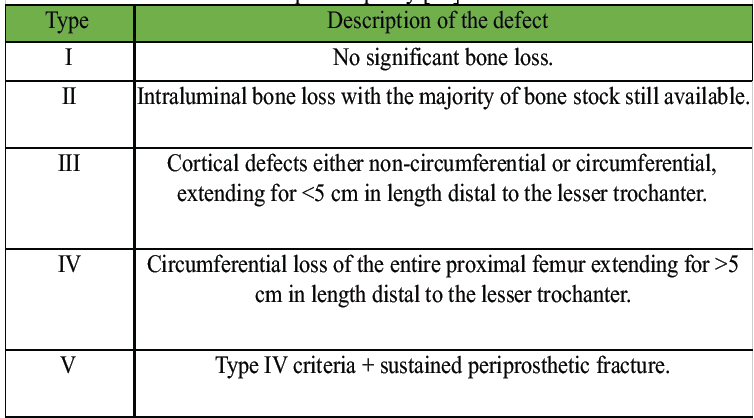
Table 3: Modified gross classification of femoral bone loss during revision total hip arthroplasty [24].
The ZMR system offers modularity, but it is susceptible to mechanical failure. Despite its rarity, cantilever fatigue of the ZMR stem is a catastrophic adverse event. This adverse event is associated with patient-related and implant-related risk factors. The patient-related risk factors include advanced age, high BMI, and a compromised proximal bone stock, whereas implant-related factors include the use of shorter ZMR stems (<200 mm), smaller stem diameter, and extended offset designs, all of which are frequently reported to be common in many cases of stem failure that typically occurs at the body-stem junction.
In high-risk patients, a monoblock femoral stem may be a safer option. Our patient underwent a prompt revision surgery using a Wagner SL monoblock stem and had a satisfactory early recovery, highlighting the clinical relevance of this recommendation. With the limited number of reported cases and the retrospective nature of them, further prospective, multicenter studies are recommended to better define the risk factors and establish techniques and strategies to prevent ZMR stem failure.
References
- 1. Learmonth ID, Young C, Rorabeck C. The operation of the century: Total hip replacement. Lancet 2007;370:1508-19. [Google Scholar] [PubMed]
- 2. Bastian JD. Total hip arthroplasty-current challenges. Medicina (Kaunas) 2023;59:1011. [Google Scholar] [PubMed]
- 3. Van Houwelingen AP, Duncan CP, Masri BA, Greidanus NV, Garbuz DS. High survival of modular tapered stems for proximal femoral bone loss in revision total hip arthroplasty. Clin Orthop Relat Res 2013;471:503-10. [Google Scholar] [PubMed]
- 4. Zimmer Biomet. Zimmer Modular Revision (ZMR) Hip System: Surgical Technique Manual. Warsaw, IN: Zimmer Biomet; 2010. Available from: https://www.zimmerbiomet.com/content/dam/zimmer-biomet/medical-professionals/hip/ZMR%20Hip%20System/zmr-hip-system.pdf. [Last accessed on 25 Jan 2010]. [Google Scholar] [PubMed]
- 5. Grupp TM, Weik T, Bloemer W, Knaebel HP. Modular titanium alloy neck adapter failures in hip replacement–failure mode analysis and influence of implant material. BMC Musculoskelet Disord 2010;11:3. [Google Scholar] [PubMed]
- 6. Huddleston JI 3rd, Tetreault MW, Yu M, Bedair H, Hansen VJ, Choi HR, et al. Is there a benefit to modularity in ‘simpler’ femoral revisions? Clin Orthop Relat Res 2016;474:415-20. [Google Scholar] [PubMed]
- 7. Mohan R, Unnikrishnan N, Gudena R. Cantilever failure of modular uncemented femoral revision stem in patients with poor proximal femoral support; how to avoid it? Arch Bone Jt Surg 2024;12:240-4. [Google Scholar] [PubMed]
- 8. Hickie KL, Neufeld ME, Howard LC, Greidanus NV, Masri BA, Garbuz DS. Long-term outcomes of revision total hip arthroplasty with the zimmer modular revision hip system. Bone Joint J 2024;106-B 5 Supple B:112-7. [Google Scholar] [PubMed]
- 9. Hafez MA. Removal of well-fixed, fluted cementless femoral stem: Revisiting the antegrade drilling technique for easier stem extraction. Orthop J Extremity Dis 2024;6:121-5. [Google Scholar] [PubMed]
- 10. Nasr PJ, Keene GS. Revision of a fractured uncemented revision stem using a custom designed punch and retrograde through-knee approach. Case Rep Orthop 2015;2015:485729. [Google Scholar] [PubMed]
- 11. Lakstein D, Eliaz N, Levi O, Backstein D, Kosashvili Y, Safir O, et al. Fracture of cementless femoral stems at the mid-stem junction in modular revision hip arthroplasty systems. J Bone Joint Surg Am 2011;93:57-65. [Google Scholar] [PubMed]
- 12. Taheriazam A, Khanmohammadi B, Asadollah A, Dindar M. Zimmer modular revision stem failure on total hip arthroplasty due to stem fracture from cone taper stem junction. J Res Orthop Sci 2022;9:57-64. [Google Scholar] [PubMed]
- 13. Efe T, Schmitt J. Analyses of prosthesis stem failures in noncemented modular hip revision prostheses. J Arthroplasty 2011;26:665.e7-12. [Google Scholar] [PubMed]
- 14. Ortega PC, Medeiros WB Jr., Moré AD, Vasconcelos RF, Da Rosa E, Roesler CR. Failure analysis of a modular revision total HIP arthroplasty femoral stem fractured in vivo. Eng Fail Anal 2020;114:104591. [Google Scholar] [PubMed]
- 15. U.S. Food and Drug Administration. MAUDE Adverse Event Report: Zimmer Biomet Inc. ZMR Taper Stem Large Junction 22×185 Hip Prosthesis. Available at: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfmaude/detail.cfm?mdrfoi__id=7204180&pc=LWJ. [Last accessed on 15 Jan 2026]. [Google Scholar] [PubMed]
- 16. U.S. Food and Drug Administration. MAUDE Adverse Event Report: Zimmer Biomet Inc. ZMR XL Taper Stem Nitrided Cementless Hip Prosthesis. Available at: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfmaude/detail.cfm?mdrfoi__id=21917219&pc=JDI. Last accessed on 15 Jan 2026]. [Google Scholar] [PubMed]
- 17. McInnes J, Allen J, Garceau S, Warschawski Y, Rajgopal R, Safir O, et al. Revision hip arthroplasty using a porous-coated or taper ZMR implant: Minimum 10-year follow-up of implant survivorship. J Am Acad Orthop Surg 2021;29:e41-50. [Google Scholar] [PubMed]
- 18. Koch CN, Mateo LS, Kayiaros S, Cassidy KA, Jerabek SA, Gonzalez Della Valle A. Spontaneous fractures of a modern modular uncemented femoral stem. HSS J 2016;12:250-4. [Google Scholar] [PubMed]
- 19. Zdero R, El-Osta B, Schemitsch EH. The biomechanical effect of offset stem design in a cementless modular femoral stem. J Arthroplasty 2011;26:1415-22. [Google Scholar] [PubMed]
- 20. Rueckl K, Boettner F, Bechler U, Baral EC, Wright TM, Sculco PK. Fracture of an S-ROM stem at the sleeve-stem junction. Arthroplast Today 2018;4:295-9. [Google Scholar] [PubMed]
- 21. Bischel OE, Suda AJ, Böhm PM, Bormann T, Jäger S, Seeger JB. Breakage of tapered junctions of modular stems in revision total hip arthroplasty-high incidence in a consecutive series of a single institution. Bioengineering (Basel) 2023;10:341. [Google Scholar] [PubMed]
- 22. Govilkar S, Gandhi MJ, Bhachu DS, Spencer-Jones R. The survivorship of revision total hip replacement with severe proximal bone deficiency using a modular taper fluted prosthesis. Acta Orthop Belg 2022;88:303-9. [Google Scholar] [PubMed]
- 23. Mirza SB, Dunlop DG, Panesar SS, Naqvi SG, Gangoo S, Salih S. Basic science considerations in primary total hip replacement arthroplasty. Open Orthop J 2010;4:169-80. [Google Scholar] [PubMed]
- 24. Gross AE, Hutchison CR, Zhang L, Zhang L, Wang G. The use of structural allografts in revision total hip arthroplasty with severe femoral bone loss. Instr Course Lect 2011;60:105-16. [Google Scholar] [PubMed]
- 25. Engh CA Jr. Trochanteric sliding osteotomy hip arthroplasty exposure. Semin Arthroplasty JSES 2004;15:119-21. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Clinical-Radiological Dissociation after Failed Monteggia Fixation: Preserved Function at 2 Years Despite Proximal Ulnar Fibrous Non-union and Chronic Lateral Radial Head Dislocation
July 1, 2026 Clinical-Radiological Dissociation after Failed Monteggia Fixation: Preserved Function at 2 Years Despite Proximal Ulnar Fibrous Non-union and Chronic Lateral Radial Head Dislocation July 1, 2026 The Development of Metabolic Bone Failure as the Principal Manifestation of Undiagnosed Primary Hyperparathyroidism: A Rare Instance of Bilateral Femoral Neck Fractures
July 1, 2026 The Development of Metabolic Bone Failure as the Principal Manifestation of Undiagnosed Primary Hyperparathyroidism: A Rare Instance of Bilateral Femoral Neck Fractures July 1, 2026 Short-term Clinical Outcomes of Primary Total Hip Arthroplasty with the CoreHip Stem
July 1, 2026 Short-term Clinical Outcomes of Primary Total Hip Arthroplasty with the CoreHip Stem July 1, 2026 A Comparative Study of Functional Outcome Following Total Hip Replacement by Posterolateral and Anterolateral Approach
July 1, 2026 A Comparative Study of Functional Outcome Following Total Hip Replacement by Posterolateral and Anterolateral Approach