
Hemiarthroplasty for femoral neck fractures in lower limb amputees requires meticulous planning, and special maneuvers may be indicated for stump manipulation during surgery.
Gowtham Sushruth, Sushrutha Multispeciality Hospital, Siddipet, Telangana, India. E-mail:sushruthgowtham@gmail.com
Abstract
Introduction: Femoral neck fractures in lower limb amputees are uncommon. Technical difficulties include patient positioning, stump manipulation, and poor bone quality due to osteoporosis. We report the case of a 55-year-old woman with a femoral neck fracture and an ipsilateral below-knee amputation (BKA), managed with hemiarthroplasty.
Case Report: The patient was diagnosed with a femoral neck fracture on the right side after she had a fall at home. She had undergone BKA due to complications of a diabetic foot 9 months earlier. We performed uncemented hemiarthroplasty with an Austin-Moore prosthesis using the posterior approach. No special devices or maneuvers were required for the manipulation of the stump during surgery. The post-operative period was uneventful, and the patient began weight-bearing with a walker and prosthetic limb about 10 days after surgery. Throughout the 25-month follow-up period, no clinical or radiological complications related to the hemiarthroplasty were identified, and her final Hip Disability and Osteoarthritis Outcome Score, Joint Replacement (HOOS, JR) score improved to 80.55. The patient succumbed to breast cancer 1 month following the most recent follow-up.
Conclusion: Hemiarthroplasty remains a reliable option for managing femoral neck fractures in below-knee amputees. However, difficulties in limb manipulation must be anticipated. Gentle handling and meticulous surgical technique are critical in avoiding iatrogenic complications.
Keywords: Hemiarthroplasty, Austin-Moore prosthesis, below-knee amputee, lower limb amputee, femoral neck fracture, femur neck fracture.
Femoral neck fractures in lower limb amputees are uncommon and present a challenge to both orthopedic surgeons and the rehabilitation team. This can be challenging to manage due to technical difficulties, including patient positioning, ideal surgical approach, and stump manipulation for the reduction of prosthesis. In lower limb amputees, the incidence of ipsilateral hip fractures has increased, largely due to decreased bone mineral density, particularly among those using prosthetic limbs [1]. We report the case of a 55-year-old woman with a femoral neck fracture and an ipsilateral below-knee amputation (BKA), managed with hemiarthroplasty.
The patient, a 55-year-old woman, was brought to the hospital with a complaint of pain in the right hip after a fall at home. She had undergone a BKA of the right lower limb 9 months earlier due to complications of a diabetic foot. After the amputation, she began walking with a below-knee prosthesis and a walker inside her domicile. Based on the observations of her family members, she had not fully adapted to the prosthesis, which eventually led to a fall while walking on a patch of unpaved ground in the courtyard of her domicile. Radiographs revealed a right-sided femoral neck fracture (Fig. 1a). We also obtained a scanogram of the lower limbs (Fig. 1b).
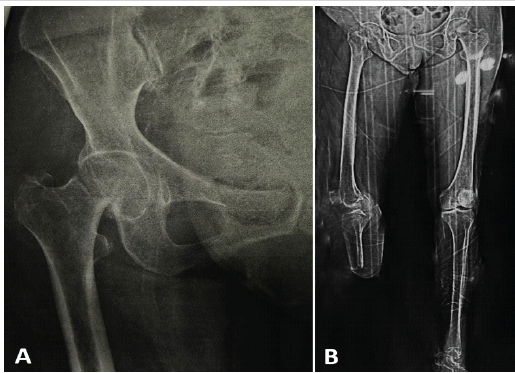
Figure 1: (a) Pre-operative radiograph of the right hip showing a fracture in the neck of the femur, (b) full-length scanogram of both the lower limbs.
She was a known case of Type II diabetes mellitus. At the time of presentation, she had maintained good glycemic control with the use of oral hypoglycemic drugs. The patient was from a low socioeconomic background. After carefully deliberating the pros and cons of osteosynthesis and hemiarthroplasty, we advised hemiarthroplasty to the patient. Physical examination did not reveal any vascular or neurological complications. The stump was healthy except for a pressure sore on the lateral aspect of the leg due to the ill-fitting socket of the prosthesis (Fig. 2a and b).
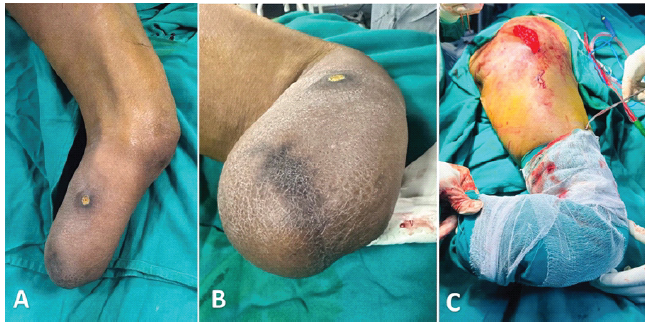
Figure 2: (a) Skin condition of the amputation stump, (b) Pressure sore due to an ill-fitting prosthetic limb on the lateral aspect of the leg, (c) Image to demonstrate the positioning of the stump during surgery.
After medical clearance and pre-anesthetic evaluation, we performed uncemented unipolar hemiarthroplasty under spinal anesthesia through the posterior approach to the hip using an Austin-Moore prosthesis (AMP). The patient was kept in the left lateral position. Anticipating difficulty in maneuvering the limb during surgery, we kept a bone hook and Schanz pins ready. Perumal et al. have described a technique for above-knee amputees (AKA) where two perpendicular Schanz pins (anteroposterior and sagittal) are placed in the distal part of the stump to help in limb manipulation during surgery [2]. Intraoperative limb manipulation was more straightforward than anticipated. We did not require the placement of Schanz pins or any special maneuvers (Fig. 2 c). We manipulated the limb gently while making the neck cut and preparing the femoral canal to avoid iatrogenic fractures and inadvertent injuries to the adjacent structures. The head size was found to be 43 mm. A 43 mm AMP was implanted, and the prosthesis was relocated into the hip joint. The wound was closed in layers. The post-operative period was uneventful.
After surgery, we started hip and knee range of motion exercises for the patient. An order was placed for a new below-knee prosthesis as the old one had a poor fit. The new prosthesis arrived in 1 week, after which the patient underwent guided rehabilitation and gait training. She was able to bear weight on the operated limb with ease 10 days after the surgery with the below-knee prosthesis and support of a walker. Suture removal was done on the 10th post-operative day.
The patient was followed regularly during the first 6 months after surgery (Fig. 3).
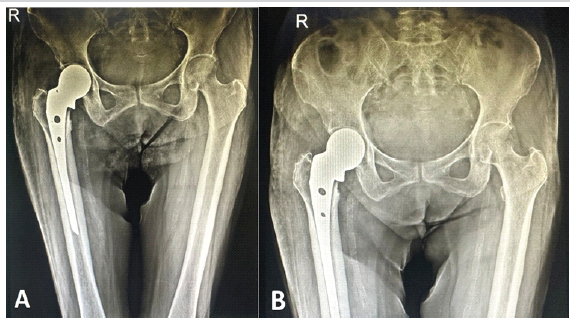
Figure 3: (a) Immediate post-operative radiograph, (b) radiograph at 6 months of follow-up.
About 10 months postoperatively, she was diagnosed with breast cancer and subsequently began receiving treatment at another hospital. At her most recent evaluation, 25 months after the hemiarthroplasty, her Hip Disability and Osteoarthritis Outcome Score, Joint Replacement (HOOS, JR) score was 80.55. There were no clinical concerns, and radiographs showed no evidence of prosthetic loosening or subsidence (Fig. 4). Unfortunately, she succumbed to breast cancer 1 month later. Throughout the 25-month follow-up period, no clinical or radiological complications related to the hemiarthroplasty were identified.
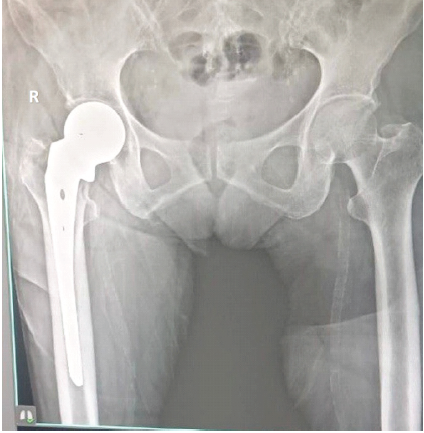
Figure 4: Follow-up radiograph at 25 months.
Femoral neck fractures in the setting of BKA are uncommon and very challenging to treat. There are no well-established guidelines, and only a few studies have reported long-term outcomes among amputees [3]. Osteosynthesis for femoral neck fractures is often challenging and has a high risk of complications and failure rates due to altered limb biomechanics, including risk of avascular necrosis, osteoporosis, muscle atrophy, and early onset of hip osteoarthritis [4]. Limb amputation leads to musculoskeletal changes in both the amputated and contralateral limbs, including increased osteoporosis on the amputated side, higher rates of osteoarthritis in the intact limb, and muscle wasting on both sides due to anatomical and surgical factors [5,6]. Studies have shown that lower extremity amputees are at a higher risk of ipsilateral hip fractures, attributed to reduced bone density and the mechanical stresses imposed by prosthetic use [7,8]. Although bipolar hemiarthroplasty and total hip arthroplasty (THA) are generally preferred for femoral neck fractures, an AMP was chosen in this case due to the patient’s significant financial constraints. In addition, THA involves longer operative time and higher resource requirements. Hence, after discussion with the patient and her family members, unipolar hemiarthroplasty with an AMP was considered a pragmatic option to facilitate early pain relief and mobilization. Several cases of femoral neck fractures in lower limb amputees have been reported in the literature (Table 1), managed using osteosynthesis [9,10], bipolar hemiarthroplasty [2,11], or THA [4,12,13,14].
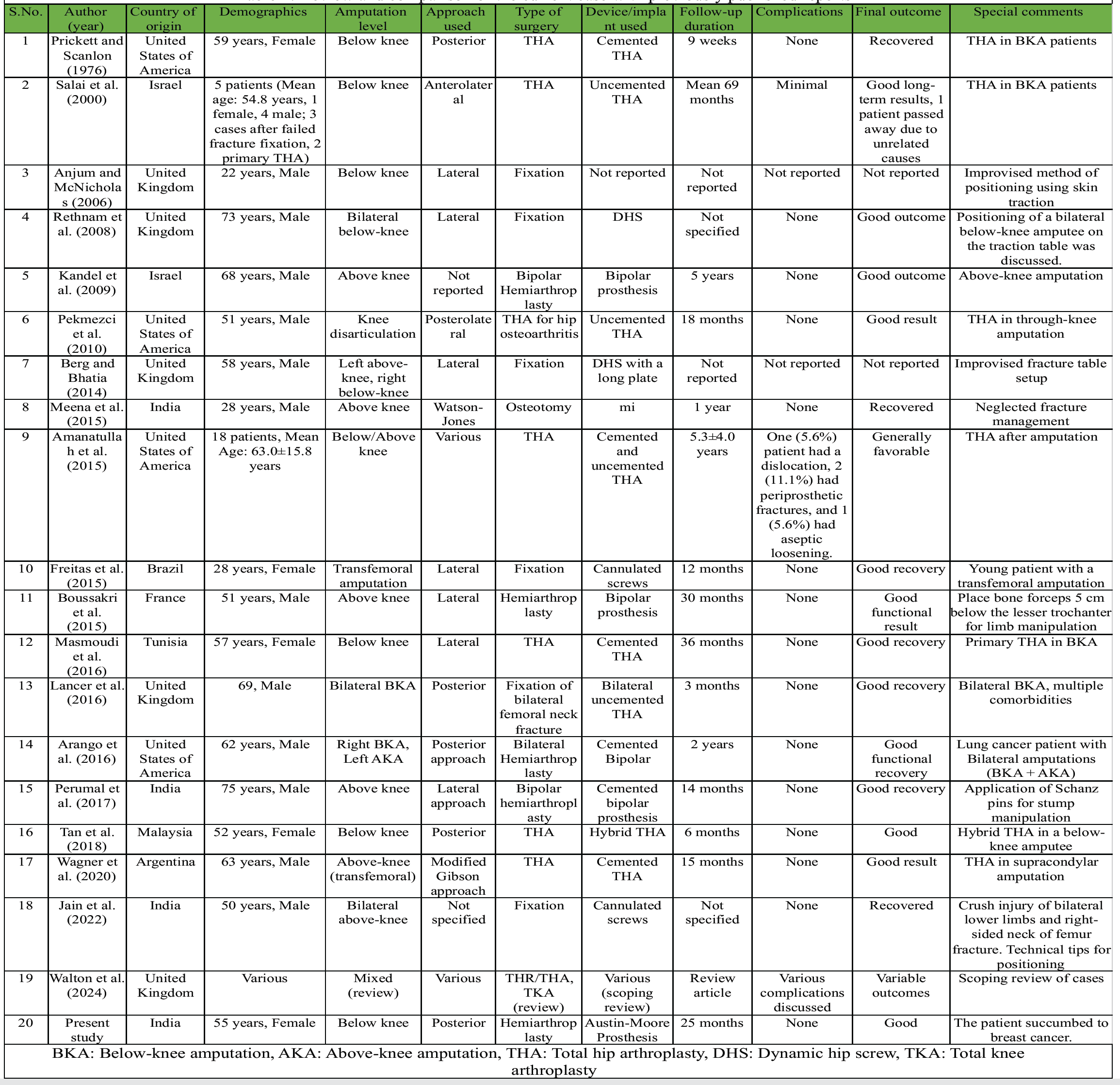
Table 1: Review and comparison of the current case with previously published reports
However, there are no reported cases of a unipolar hip prosthesis being used for the treatment of ipsilateral femoral neck fractures in below-knee amputees. Arango et al. reported a case of bilateral femoral neck fractures occurring 6 months apart in a bilateral lower limb amputee, successfully managed with staged hemiarthroplasties using different stem designs based on the level of amputation [15].
Wagner et al. described a transfemoral amputee who underwent cemented THA for a femoral neck fracture, highlighting the use of a Steinmann pin for limb control during the procedure [4]. Lancer et al. presented a rare case of bilateral displaced femoral neck fractures in a bilateral below-knee amputee managed with synchronous bilateral uncemented THA, achieving good functional recovery [12]. Perumal et al. detailed the surgical challenges of performing hemiarthroplasty in an AKA and recommended the use of Schanz pins for limb control and version alignment [2]. Tan et al. reported good results with hybrid THR in a below-knee amputee [16].
Walton et al., in a systematic review, summarized the existing literature on hip and knee replacements in amputees, noting generally favorable outcomes but emphasizing the technical difficulties inherent to surgery in this population [3]. Jain et al. and Berg and Bhatia provided technical tips for internal fixation in bilateral AKA, stressing the need for innovative intraoperative positioning strategies [9,10]. Anjum and McNicholas described a novel method of applying skin traction to the BKA stump to secure the limb to the traction table [17]. Rethnam et al. discussed the challenges of positioning a bilateral below-knee amputee with an intertrochanteric fracture on a traction table. They suggested that the boot of the traction table can be secured directly to the stump, or that the patient’s prosthesis can be fitted onto the stump and the prosthetic foot then fixed to the boot, allowing effective application of traction during surgery [18].
Meena et al. presented a neglected femoral neck fracture in an AKA managed with valgus osteotomy, suggesting that fractures in amputees should be treated with similar urgency and principles as in non-amputees [19]. In comparison, our case involved a below-knee amputee with a femoral neck fracture successfully managed with unipolar hemiarthroplasty (AMP), achieving good functional recovery without the need for complex intraoperative modifications.
This case adds to the limited body of literature on the management of ipsilateral femoral neck fractures in below-knee amputees. Hemiarthroplasty is a reliable treatment option with outcomes comparable to those reported in non-amputee populations when meticulous surgical technique is employed.
A limitation in this case report is that the patient was followed up on only for 2 years, as the patient succumbed to breast cancer. With a growing number of lower limb amputee populations around the world, future studies can analyze the long-term outcomes of various treatment modalities for femoral neck fractures in amputees, along with an analysis of biomechanical challenges unique to this patient population, which may influence surgical decision-making and rehabilitation strategies.
Hemiarthroplasty remains a reliable option for managing femoral neck fractures in below-knee amputees, offering the advantages of early mobilization, full weight-bearing, and return to daily activities. However, difficulties in limb manipulation must be anticipated. Gentle handling and meticulous surgical technique are critical in avoiding iatrogenic complications. Thorough pre-operative planning, with a readiness to adapt intraoperatively, is key to achieving successful outcomes in this unique patient population.
Hemiarthroplasty for femoral neck fractures in lower-limb amputees requires careful planning and may need special stump manipulation techniques intraoperatively to facilitate reduction and accurate implant positioning.
References
- 1. Freitas A, Souto DR, Da Silva JF, Dantas BR, De Paula AP. Treatment of an acute fracture of the femoral neck in a young female adult with a transfemoral amputation: A case report. JBJS Case Connect 2015;5:e58. [Google Scholar] [PubMed]
- 2. Perumal R, Gaddam SR, Vasudeva J, Dheenadhayalan J, Rajasekaran S. Bipolar hemiarthroplasty in a patient with above-knee amputation: Surgical technique. J Orthop Case Rep 2017;7:54-7. [Google Scholar] [PubMed]
- 3. Walton TJ, Chatterton AL, Goodwin VA. Hip and knee replacement in lower limb amputees: A scoping review. BMC Musculoskelet Disord 2024;25:239. [Google Scholar] [PubMed]
- 4. Wagner EG, Quiroga R. Reemplazo total de cadera en un paciente con amputación supracondílea homolateral. Rev Asoc Argent Ortop Traumatol 2020;85:151-6. [Google Scholar] [PubMed]
- 5. Masmoudi K, Rbai H, Fradj AB, Saâdena J, Boughattas A. Primary total hip replacement for a femoral neck fracture in a below-knee amputee. J Orthop Case Rep 2016;6:63-6. [Google Scholar] [PubMed]
- 6. Boussakri H, Alassaf I, Hamoudi S, Elibrahimi A, Ntarataz P, ELMrini A, et al. Hip arthroplasty in a patient with transfemoral amputation: A new tip. Case Rep Orthop 2015;2015:593747. [Google Scholar] [PubMed]
- 7. Pekmezci M, Nunley RM, Barrack RL. Technique for total hip arthroplasty in a patient with through-knee amputation. J Arthroplasty 2010;25:659.e1-3. [Google Scholar] [PubMed]
- 8. Amanatullah DF, Trousdale RT, Sierra RH. Total hip arthroplasty after lower extremity amputation. Orthopedics 2015;38:e394-400. [Google Scholar] [PubMed]
- 9. Jain A, Bansal H, Mittal S, Kumar A, Trikha V. Intracapsular fracture of the proximal femur in a bilateral above-knee amputee: A case report with technical tips for intraoperative positioning and literature review. Chin J Traumatol 2022;25:306-10. [Google Scholar] [PubMed]
- 10. Berg AJ, Bhatia C. Neck of femur fracture fixation in a bilateral amputee: An uncommon condition requiring an improvised fracture table positioning technique. BMJ Case Rep 2014;2014:bcr2013203504. [Google Scholar] [PubMed]
- 11. Kandel L, Hernandez M, Safran O, Schwartz I, Liebergall M, Mattan Y. Bipolar hip hemiarthroplasty in a patient with an above knee amputation: A case report. J Orthop Surg Res 2009;4:30. [Google Scholar] [PubMed]
- 12. Lancer HR, Smitham P, Ray P. Bilateral neck of femur fractures in a bilateral below-knee amputee: A unique case. Case Rep Orthop 2016;2016:7083671. [Google Scholar] [PubMed]
- 13. Prickett NM, Scanlon CJ. Total joint replacement in extremities with below-knee amputations. Phys Ther 1976;56:925-7. [Google Scholar] [PubMed]
- 14. Salai M, Amit Y, Chechik A, Blankstein A, Dudkiewicz I. Total hip arthroplasty in patients with below-knee amputations. J Arthroplasty 2000;15:999-1002. [Google Scholar] [PubMed]
- 15. Arango D, Tiedeken NC, Gershkovich G, Shaffer G. Bilateral hemiarthroplasty in a patient with below-knee and above-knee amputations: A case report. JBJS Case Connect 2016;6:e3. [Google Scholar] [PubMed]
- 16. Tan JB, Ong JH, Ngim HL, Chua HS, Lee KH, Zulkiflee O. Primary total hip arthroplasty (THA) in a below knee amputee with neck of femur fracture (NOF) Allows Early Ambulation. Malays J Orthop 2018; Supplements/2018/EA15. [Google Scholar] [PubMed]
- 17. Anjum SN, McNicholas MJ. Innovative method of traction on fracture table in femoral neck fracture fixation in a below knee amputee. Inj Extra 2006;37:277-8. [Google Scholar] [PubMed]
- 18. Rethnam U, Yesupalan RS, Shoaib A, Ratnam TK. Hip fracture fixation in a patient with below-knee amputation presents a surgical dilemma: A case report. J Med Case Rep 2008;2:296. [Google Scholar] [PubMed]
- 19. Meena U, Meena R, Balaji S, Gaba S. Management of neglected femoral neck fracture in above knee amputated limb: A case report. Chin J Traumatol 2015;18:370-2. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Cemented versus Uncemented Hemiarthroplasty in Femoral Neck Fractures: A Comparative Case Series Using Singh Index for Surgical Decision-Making
June 1, 2026 Cemented versus Uncemented Hemiarthroplasty in Femoral Neck Fractures: A Comparative Case Series Using Singh Index for Surgical Decision-Making June 1, 2026 Managing Periprosthetic Fracture of the Proximal Femur Using Total Hip Arthroplasty in a Patient with Sequelae of Poliomyelitis: Case Report and Literature Review
June 1, 2026 Managing Periprosthetic Fracture of the Proximal Femur Using Total Hip Arthroplasty in a Patient with Sequelae of Poliomyelitis: Case Report and Literature Review June 1, 2026 A Rare Neglected Ipsilateral Humeral Triad: Comminuted Proximal Humerus Nonunion with Avascular Necrosis, Mid-Shaft Fracture, and High Radial Nerve Palsy Managed with Staged Reconstruction
June 1, 2026 A Rare Neglected Ipsilateral Humeral Triad: Comminuted Proximal Humerus Nonunion with Avascular Necrosis, Mid-Shaft Fracture, and High Radial Nerve Palsy Managed with Staged Reconstruction April 1, 2026 Outcomes of Total Hip Arthroplasty for Traumatic versus Non-Traumatic Hip Pathology: A Prospective Cohort Study
April 1, 2026 Outcomes of Total Hip Arthroplasty for Traumatic versus Non-Traumatic Hip Pathology: A Prospective Cohort Study