
Giant ganglion cysts of the tibialis anterior tendon are exceedingly rare and may harbor concurrent degenerative tendinopathy requiring surgical management beyond simple excision; platelet-rich plasma augmentation and meticulous post-operative surveillance are essential components of comprehensive care.
Dr. Suraj Sajeev [1.1], Department of Orthopaedic Surgery, Sengkang General Hospital, Sengkang, Singapore. E-mail: surajsajeev1988@gmail.com
Abstract
Introduction: Ganglion cysts of the tibialis anterior tendon [2.1] (ATT) are exceedingly rare. We report a case of a giant ATT ganglion cyst associated with adult-acquired flatfoot deformity and underlying degenerative tendinopathy and describe a systematic multimodal surgical technique for its management.
Case Report: A 55-year-old male construction worker presented with a 4-month history of a progressively enlarging left ankle swelling that prevented him from wearing protective footwear. Magnetic resonance imaging (MRI) demonstrated a lobulated cyst measuring 4.4 × 3.9 × 11.7 cm with internal septations and extensive underlying ATT degenerative change. Surgical management comprised an anterior elliptical incision, cyst decompression, tendon debridement, tubularization with Vicryl 4-0 sutures, platelet-rich plasma injection, and sheath marsupialization. Approximately 4 weeks postoperatively, the patient developed infective tenosynovitis, confirmed on repeat MRI, with a subcentimeter susceptibility focus raising suspicion for a retained foreign body.
Conclusion: Giant ATT ganglion cysts may harbor significant underlying degenerative tendinopathy requiring active surgical management beyond simple excision. A systematic approach combining cyst excision, debridement, tubularization, and biologic augmentation is described. Surgeons should maintain a low threshold for repeat MRI when post-operative infective tenosynovitis is suspected following ATT surgery.
Keywords: Tibialis anterior tendon, ganglion cyst, tenosynovitis, adult-acquired flatfoot deformity, platelet-rich plasma, tubularization.
Ganglion cysts are the most common benign soft-tissue masses of the extremities, typically arising from tendon sheaths or joint capsules. Giant ganglion cysts of the tibialis anterior tendon (ATT) remain exceedingly rare, with only isolated reports in the orthopedic literature [1,2,3]. The ATT is the principal dorsiflexor and invertor of the foot, playing a critical role in gait mechanics and dynamic arch support. Dysfunction of this tendon carries significant functional morbidity, particularly when compounded by concurrent structural deformities such as adult-acquired flatfoot [4]. The combination of a voluminous tendon sheath cyst with underlying degenerative tendinopathy presents a complex surgical challenge. This case report describes the clinical presentation, pre-operative imaging, operative management, and post-operative course, alongside a focused review of the relevant literature.
A 55-year-old male construction worker presented with a 4-month history of a progressively enlarging swelling over the left dorsal ankle. The mass had become sufficiently large to prevent him from wearing protective work footwear, prompting orthopedic consultation. He reported no antecedent trauma but described prolonged occupational loading of the lower extremities over many years. His medical history was otherwise unremarkable. Physical examination demonstrated a large, fluctuant, non-tender ganglion mass arising from the region of the ATT, with tenderness on palpation over the medial cuneiform-navicular joint. Adult-acquired flatfoot deformity of the left foot was identified, with loss of the medial longitudinal arch and associated hindfoot valgus alignment. Ankle dorsiflexion range of motion was restricted by the mass. Distal neurovascular status was intact.
Imaging Findings:
Plain radiographs of the left ankle and foot demonstrated pes planus deformity with degenerative changes at the subtalar and tibiotalar joints. Magnetic resonance imaging (MRI) was subsequently performed, including sagittal T2-weighted fat-saturated (T2w FS) and T1-weighted (T1w) sequences, axial T2w FS and T1w sequences, and post-contrast sequences following intravenous Dotarem (10 mL) administration (Fig. 1).
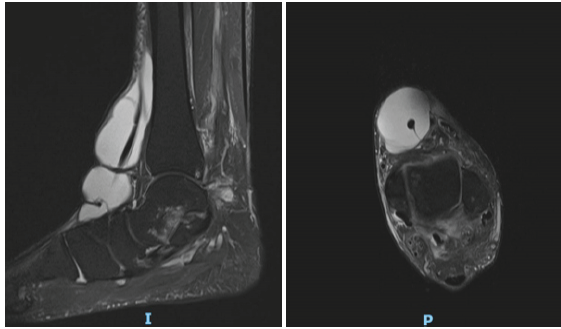
Figure 1: Pre-operative magnetic resonance imaging – Axial T1-weighted (left) and sagittal T2-weighted fat-saturated (T2w FS) (right). Left: A large, well-circumscribed lobulated cystic mass occupies the anterodorsal compartment, homogeneously hyperintense on T1-weighting, consistent with a fluid-filled ganglion of the tibialis anterior tendon sheath measuring 4.4 × 3.9 × 11.7 cm. Right: The sagittal T2w FS sequence demonstrates the full craniocaudal extent (~11.7 cm) of the lobulated hyperintense ganglion cyst, intimately associated with the tibialis anterior tendon as it courses toward its insertion on the medial cuneiform.
MRI demonstrated a single large lobulated cystic ganglion associated with the ATT measuring 4.4 × 3.9 × 11.7 cm (transverse × anteroposterior × craniocaudal), consistent with a chronic loculated tendon sheath effusion and stenosing tenosynovitis [1,2]. Internal septations and distal debris were present. Post-contrast sequences demonstrated no abnormal tendon sheath thickening or solid nodule. The underlying ATT showed extensive degenerative change adjacent to its insertion at the medial cuneiform, while the remaining extensor tendons appeared normal. Ligamentous assessment revealed severe attenuation of the anterior talofibular, calcaneofibular, and posterior talofibular ligaments, consistent with chronic high-grade partial tears. A 0.5 cm osteochondral defect was noted at the medial talar dome. An accessory of naviculare was also identified.
Surgical Technique:
Under general anesthesia with the patient in the supine position, an anterior longitudinal elliptical skin incision was fashioned over the dorsum of the ankle, incorporating the redundant skin created by the underlying mass. Careful circumferential dissection isolated the ATT beneath the extensor retinaculum. The ganglion sheath was then incised anteriorly, the mucinous gelatinous contents evacuated, and the cavity thoroughly irrigated (Fig. 2).

Figure 2: Intraoperative photograph – initial cyst exposure – Following anterior longitudinal elliptical incision over the left dorsal ankle, the large multilobulated ganglion cyst herniates through the wound, displaying its characteristic pearly-white, smooth, translucent, multilobulated appearance consistent with the septated morphology demonstrated on pre-operative magnetic resonance imaging. The extensor retinaculum is retracted using retractors.
Intraganglionic inspection revealed multiple longitudinal degenerative tears measuring approximately 4 cm in length, located 1 cm proximal to the ATT insertion at the medial cuneiform. Degenerated fibers were carefully excised using a curette to achieve a viable tissue bed. The tendon was reconstituted and tubularized using Vicryl 4-0 absorbable sutures, restoring its cylindrical architecture (Fig. 3) [5,6,7].
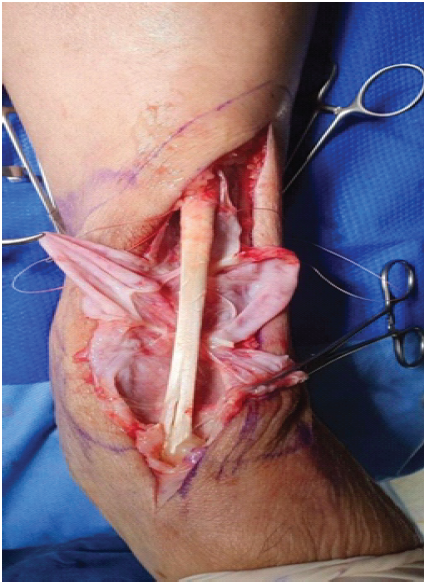
Figure 3: Intraoperative photograph – tibialis anterior tendon pathology and tubularization – Following cyst decompression and evacuation of its mucinous contents, the underlying tibialis anterior tendon is exposed, revealing multiple longitudinal degenerative tears (~4 cm in length, located 1 cm proximal to the medial cuneiform insertion) with splaying and fraying of tendon fibers. The patulous, redundant tendon sheath is clearly visible. Vicryl 4-0 sutures have been placed in preparation for tubularization to restore the cylindrical architecture of the tendon.
Four milliliters of intraoperatively prepared platelet-rich plasma (PRP) were then injected directly into the tendon substance to promote biologic healing [6,8,9]. The patulous and redundant tendon sheath was excised, and the remaining edges were marsupialized to the adjacent deep fascia to prevent re-accumulation of fluid. The extensor retinaculum was meticulously repaired in layers, followed by layered skin closure incorporating the removal of the redundant skin ellipse. A below-knee plaster slab was applied with the ankle in the neutral position.
Post-operative course and cmplications:
The immediate post-operative period was uneventful. Approximately 4 weeks following the index procedure, the patient re-presented with systemic sepsis (temperature 39°C) and signs of left ankle infective tenosynovitis, including swelling, erythema, and cutaneous fluctuance. Repeat MRI of the left ankle was performed and compared with the prior study (Fig. 4).
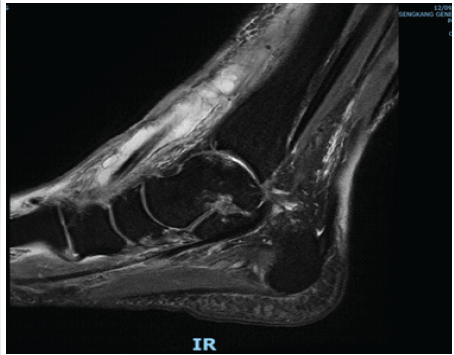
Figure 4: Post-surgical sagittal post-contrast magnetic resonance imaging (approximately 4 weeks post-operative) – Diffuse enhancement of the anterior ankle soft tissues consistent with cellulitis. The ATT tendon sheath collection extends proximally to surround the myotendinous junction with intramuscular extension and irregularly thickened, enhancing walls consistent with an infective collection. A subcentimeter susceptibility focus is identified in the subdermal layer adjacent to the ATT, raising suspicion for a retained foreign body that is radiographically occult on plain radiographs.
Post-surgical MRI demonstrated diffuse circumferential cellulitis involving the distal calf, ankle, hindfoot, and midfoot. The ATT tendon sheath was markedly distended with intermediate-signal debris-laden fluid within irregularly thickened, enhancing walls, consistent with an infective collection extending proximally to surround the myotendinous junction with intramuscular extension. A subcentimeter susceptibility focus in the subdermal layer adjacent to the ATT was identified across all sequences, raising suspicion for a retained foreign body, not visible on plain radiographs. Histopathology from the index procedure had demonstrated chronic inflammation. There were no MRI features of frank septic arthritis. The patient was managed with surgical debridement and culture-directed antibiotic therapy.
Giant ganglion cysts of the ATT are rare, with only a handful of cases previously documented in the literature [1,2]. The ATT is subject to considerable repetitive mechanical stress, particularly in occupations requiring prolonged weight-bearing and manual load-carrying. Chronic occupational loading in this construction worker likely contributed to progressive degenerative tendinopathy and subsequent reactive tenosynovitis, predisposing to cyst formation. The extraordinary craniocaudal extent of 11.7 cm reflects the insidious natural history of this condition and the high threshold many patients maintain before seeking intervention. The coexistence of adult-acquired flatfoot deformity adds significant biomechanical complexity to this case [4]. Flatfoot deformity redistributes forces across the foot and ankle, potentially accelerating tendon degeneration across multiple compartments beyond the classically implicated tibialis posterior. The identification of concurrent ATT degenerative tears intraoperatively underscores the importance of thorough inspection of the tendon when managing large ATT tendon sheath collections, since simple cyst excision without addressing the underlying tendinopathy would have been inadequate. The surgical approach employed – combining cyst excision, tendon debridement, tubularization, sheath marsupialization, and PRP augmentation – addresses both the structural and biologic dimensions of the pathology simultaneously. Tubularization restores the mechanical integrity and cylindrical architecture of the tendon [5], while PRP provides a concentrated autologous source of growth factors including platelet-derived growth factor, transforming growth factor-beta, and vascular endothelial growth factor, which promote collagen synthesis and neovascularization [6,8]. Although the clinical evidence base for PRP in tendon surgery continues to evolve, its application as an adjunct in cases of significant degenerative tendon burden is supported by current biological rationale [8]. The post-operative infective tenosynovitis represents an important clinical lesson. The identification of a suspicious susceptibility focus on post-surgical MRI – consistent with a retained foreign body not visible on plain radiographs – highlights the importance of meticulous intraoperative technique, thorough wound irrigation, and careful accounting of all surgical materials. MRI is the imaging modality of choice for evaluating post-operative complications of tendon surgery [10], and surgeons should maintain a low threshold for its use whenever post-operative infection is suspected.
We describe a rare case of a giant ganglion cyst of the ATT associated with concurrent degenerative tendinopathy and adult-acquired flatfoot deformity. Surgical management with cyst excision, tendon debridement, tubularization, sheath marsupialization, and PRP augmentation represents a systematic and reproducible technique for this complex pathology. Surgeons should anticipate underlying tendon pathology when managing large ATT cysts and be prepared to address it. Post-operative infective tenosynovitis warrants prompt MRI evaluation and aggressive management.
Giant ganglion cysts of the ATT frequently harbor underlying degenerative tendinopathy that mandates active surgical management beyond simple cyst excision. A systematic approach combining debridement, tubularization, and platelet-rich plasma augmentation offers a reproducible and biologically sound solution. Post-operative infective tenosynovitis is a rare but clinically important complication – surgeons should maintain a low threshold for repeat MRI in any patient presenting with systemic sepsis following ATT surgery.
References
- 1. Iversen JR, Solgaard S. Ganglion of the tibialis anterior tendon sheath: A case report. Acta Orthop Scand 1987;58:561-2. [Google Scholar] [PubMed]
- 2. Young L, Bartell T, Logan SE. Ganglions of the hand and wrist. South Med J 1988;81:751-60. [Google Scholar] [PubMed]
- 3. Gude W, Morelli V. Ganglion cysts of the wrist: Pathophysiology, clinical picture, and management. Curr Rev Musculoskelet Med 2008;1:205-11. [Google Scholar] [PubMed]
- 4. Johnson KA, Strom DE. Tibialis posterior tendon dysfunction. Clin Orthop Relat Res 1989;239:196-206. [Google Scholar] [PubMed]
- 5. Steffner RJ, Bharam S. Management of tendon disorders of the foot and ankle. Sports Med Arthrosc Rev 2009;17:164-75. [Google Scholar] [PubMed]
- 6. Mishra A, Pavelko T. Treatment of chronic elbow tendinosis with buffered platelet-rich plasma. Am J Sports Med 2006;34:1774-8. [Google Scholar] [PubMed]
- 7. Longo UG, Ronga M, Maffulli N. Achilles tendinopathy. Sports Med Arthrosc Rev 2009;17:112-26. [Google Scholar] [PubMed]
- 8. De Vos RJ, Weir A, Van Schie HT, Bierma-Zeinstra SM, Verhaar JA, Weinans H, et al. Platelet-rich plasma injection for chronic Achilles tendinopathy: A randomized controlled trial. JAMA 2010;303:144-9. [Google Scholar] [PubMed]
- 9. Filardo G, Kon E, Di Martino A, Di Matteo B, Merli ML, Cenacchi A, et al. Platelet-rich plasma vs hyaluronic acid to treat knee degenerative pathology: Study design and preliminary results of a randomized controlled trial. BMC Musculoskelet Disord 2012;13:229. [Google Scholar] [PubMed]
- 10. Delfaut EM, Beltran J, Johnson G, Rousseau J, Marchandise X, Cotten A. Fat suppression in MR imaging: Techniques and pitfalls. Radiographics 1999;19:373-82. [Google Scholar] [PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Angiofibroma of Knee Masquerading as Ganglion Cyst – A Rare Case Report
July 1, 2026 Angiofibroma of Knee Masquerading as Ganglion Cyst – A Rare Case Report July 1, 2026 A Prospective Randomized Controlled Study Comparing the Efficacy of Platelet Rich Plasma Injection versus Steroid Injection in Lateral Epicondylitis
July 1, 2026 A Prospective Randomized Controlled Study Comparing the Efficacy of Platelet Rich Plasma Injection versus Steroid Injection in Lateral Epicondylitis June 1, 2026 Standardized Preparation and Multi-Site Application of Leukocyte-Poor Platelet-Rich Plasma in Arthroscopic Anterior Cruciate Ligament Reconstruction: A Technical Note with Early Functional Outcomes
June 1, 2026 Standardized Preparation and Multi-Site Application of Leukocyte-Poor Platelet-Rich Plasma in Arthroscopic Anterior Cruciate Ligament Reconstruction: A Technical Note with Early Functional Outcomes April 1, 2026 Cavernous Hemangioma Masquerading as a Ganglion Cyst of the Flexors of the Index Finger: A Case Report
April 1, 2026 Cavernous Hemangioma Masquerading as a Ganglion Cyst of the Flexors of the Index Finger: A Case Report